
Abstract
BACKGROUND AND PURPOSE: Cerebellar hemangioblastomas (HBs) are traditionally classified into different morphologic types: cystic and solid. We have observed the progression from solid to cystic and have reviewed the cases seen at the regional von Hippel-Lindau (VHL) clinic to document the frequency of this progression.
METHODS: A retrospective review of the notes and images of all patients with VHL disease seen at a regional referral clinic since its inception in 1991. Sporadic HBs were not included in this study.
RESULTS: In eight patients, a total of 28 tumors were detected. Fourteen of these had or developed cysts. Of the 14 cystic tumors, eight increased in size over the follow-up period. Of the 14 solid tumors, only one increased in size without cystic change. In four patients, the tumor progressed from a cerebellar nodule to an enlarging cyst with a nodule, with the subsequent development of symptoms requiring surgical excision.
CONCLUSION: We have demonstrated that, in VHL, cerebellar HBs begin as nodules, and some subsequently develop enlarging cysts that cause pressure symptoms. In our patient population, tumors that remained solid were asymptomatic and well tolerated in the cerebellum.
Hemangioblastoma (HB) is a vascular tumor of the CNS. It occurs most often in the cerebellum, where it is the most common primary neoplasm in adults. HBs are less commonly seen in the spinal cord, and they rarely occur elsewhere in the CNS. Single tumors may be sporadic, but multiple tumors are almost always associated with von Hippel-Lindau (VHL) disease. Sporadic tumors appear in the 5th and 6th decades of life, whereas VHL-associated tumors manifest earlier, in the 3rd or 4th decades (1, 2). Richard et al (3) have shown that 34% of patients with cerebellar HBs have VHL disease.
Histologically (3) and radiologically (4), cerebellar HBs are traditionally described as four types. Type 1 (5% of posterior fossa HBs) is a simple cyst without a macroscopic nodule. Type 2 is a cyst with a mural nodule (60%). Type 3, or solid tumors (26%), and type 4, or solid tumors with small internal cysts (9%), are also seen in the cerebellum and predominate in the spinal cord. Some authors (2, 4) have stated that type 1 is actually rare.
Although the imaging findings of HB are well described, as is their appearance in and association with VHL disease, only one case report discusses the development of an enlarging cyst in association with a nodule in a spontaneous HB (5). To our knowledge, no longitudinal studies of patients with VHL disease have been performed to document this behavior. We retrospectively reviewed patients examined at a regional VHL clinic to determine if this change in tumor behavior is more common than reported. This information would be of importance for planning follow-up in these patients. We studied only patients with a diagnosis of VHL disease; sporadic HBs were not part of this study.
Methods
All patients with identified VHL disease in the Oxford region of the United Kingdom are referred to the multidisciplinary VHL clinic. Patients are given the option of undergoing baseline brain MR imaging during adolescence or at presentation, even if no CNS symptoms are present. Subsequent CNS imaging is performed for the evaluation of symptoms or for the follow-up of specific lesions. Thus, many patients undergo serial CNS imaging studies over many years. The notes and imaging records of all patients with VHL disease were reviewed. Only patients with an initial MR image that showed a tumor and only those with one or more follow-up MR examinations were included in the study. The images of these patients were examined, and the presence, size, and morphology (solid, cystic, or mixed) of cerebellar HBs were recorded. Signs, symptoms, surgical procedures, and histologic features were noted.
In all patients, the diagnosis of VHL disease was based on conventional criteria; therefore, sporadic HBs were not part of this study.
Results
A total of 39 patient records were reviewed. Eight patients had HBs, as demonstrated with MR imaging, with traceable follow-up images. The patients included one man and seven women, with a mean age at first traceable imaging of 34 years (range, 23–50 years). There were a mean of 2.75 solid tumors per patient at first traceable imaging (range, 1–10 tumors), with a mean size of 8 mm (range, 3–30 mm). Follow-up images were available for an average period of 46.3 months (range, 24–69 months). In all eight patients, a total of 28 tumors were detected during the follow-up period. Fourteen of these had or developed cysts. Of the 14 cystic tumors, eight increased in size over the follow-up period. Of the 14 solid tumors, only one increased in size without cystic change.
Four patients had solid cerebellar tumors that progressed to enlarging cysts with the subsequent development of symptoms; surgery was required. One patient had two such tumors. Serial images in three of these patients are demonstrated in Figures 1–3.

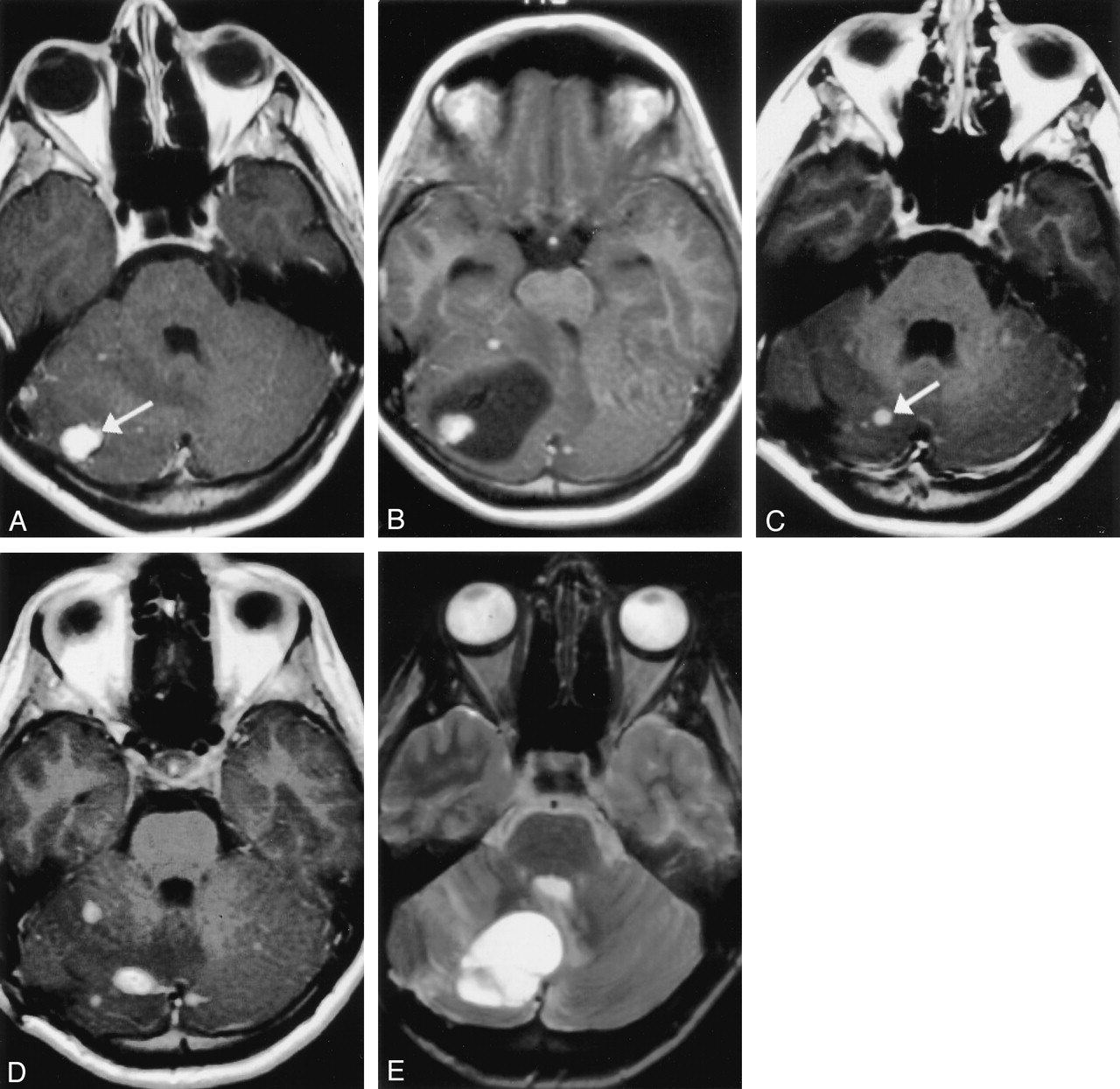
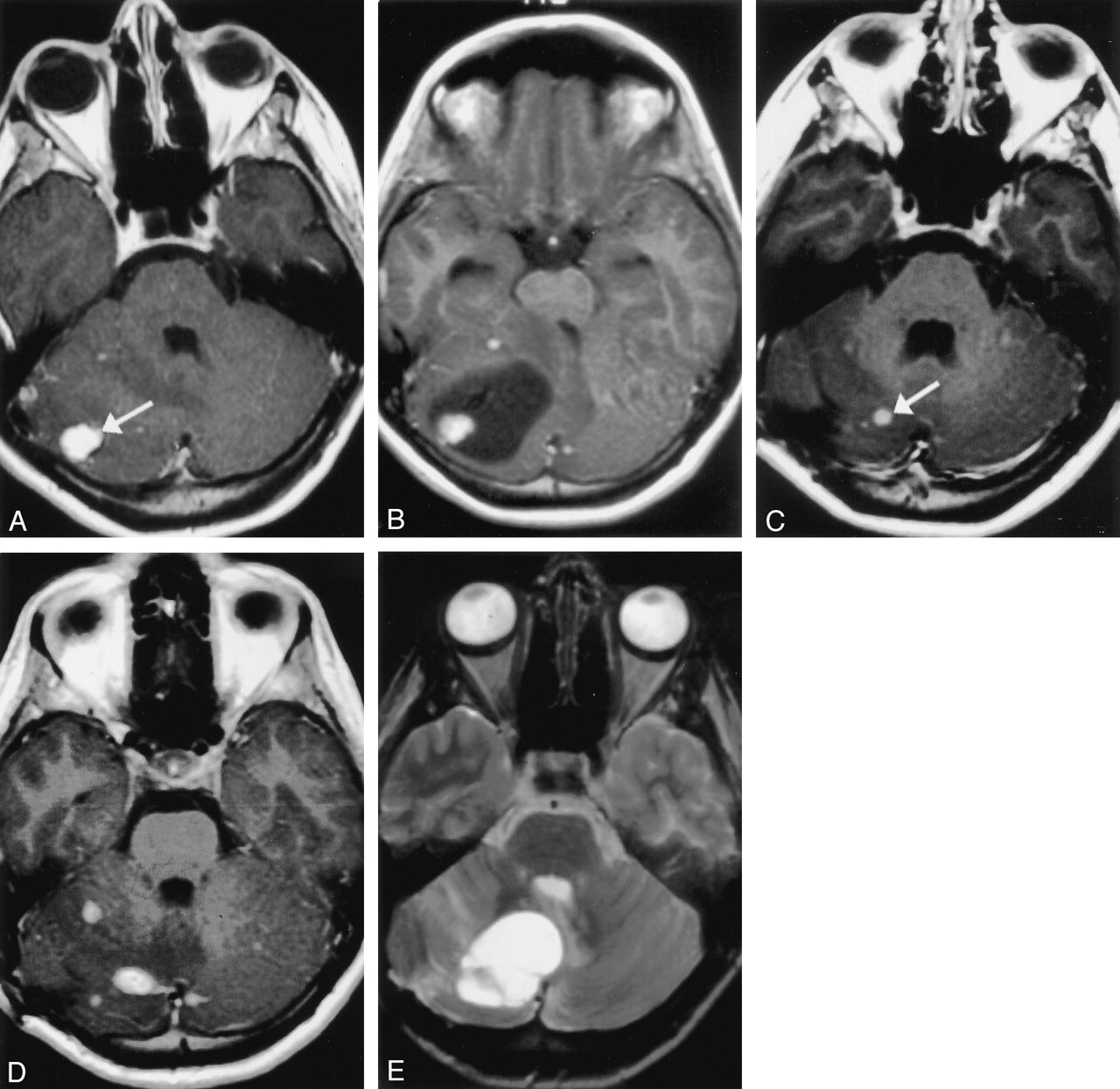
Images in a patient with a solid cerebellar tumor that progressed to enlarging cysts with the subsequent development of symptoms.
A, Contrast-enhanced T1-weighted MR image obtained at presentation demonstrates a 12-mm, enhancing, solid tumor in the right cerebellar hemisphere (arrow) (720/13 [TR/TE]).
B, Axial short-tau inversion recovery (STIR) image obtained 17 months later shows a large cyst associated with this solid tumor (arrow). An incidental left endolymphatic-sac tumor is also depicted on this image (arrowhead). (5660/29.7; TI, 150)
C, CT image shows further enlargement of the cyst 21 months after the initial study. The patient experienced posterior fossa symptoms at this time but declined surgical excision of this tumor, instead opting for craniotomy and cyst aspiration. (943/17)
D and E, MR images obtained 29 months after the initial examination. Contrast-enhanced axial T1-weighted image (D) (943/17) demonstrates enlargement of the solid part of the tumor (arrow). T2-weighted image (E) (4400/96) shows that the cyst has recurred, as had the patient’s symptoms. Surgical excision was performed shortly after this image was obtained.
Images in second patient with a solid cerebellar tumors that progressed to enlarging cysts with the subsequent development of symptoms.
A, Contrast-enhanced T1-weighted MR image shows an enhancing nodule in the right cerebellar hemisphere (arrow). (500/11 [TR/TE])
B, Image obtained 15 months later shows a large cyst associated with this nodule. Cerebellar symptoms necessitated surgical excision of this tumor. (460/13)
C, Follow-up contrast-enhanced MR image obtained 44 months after the initial study shows a new, small, enhancing nodule (arrow) and postsurgical change. (360/13)
D, Three years later, another contrast-enhanced MR image (D) shows that this nodule has increased in size. Also shown are two new, smaller nodules. (360/13)
E, Two years later, a STIR image reveals that a large cyst is now associated with this tumor. The patient experienced additional cerebellar symptoms, and further surgery was performed to remove this second tumor. (4400/96)

Images in a third patient with a solid cerebellar tumor that progressed to enlarging cyst with the subsequent development of symptoms.
A, Contrast-enhanced T1-weighted MR image obtained at presentation shows a tiny enhancing nodule in the left cerebellar hemisphere (arrow). (400/8 [TR/TE])
B, Image acquired 19 months later demonstrates a tiny cyst adjacent to this tumor. (300/9)
C, A T2-weighted image obtained 24 months after the initial study shows that the cyst has enlarged. It continued to increase in size, as demonstrated on a CT scan (not shown) obtained 3 months later. Shortly after this examination, surgical excision was performed. (3720/91.5)
The sizes of the solid tumors with enlarging cysts are shown in Table 1 and Figure 4.

Graph of cyst sizes versus time.
Sizes of Nodules and Cysts at Presentation and at Final Follow-up Imaging Before Surgery
All patients had other pathologic characterisitics related to VHL disease. All had retinal angiomas. Involvement with other tumors is listed in Table 2.
Involvement With Other Tumors of All Eight Patients
Discussion
Patients with VHL disease commonly develop cerebellar HBs, which are frequently multiple. The advent of widely available MR imaging means that many asymptomatic lesions are detected. Surgical excision is the only therapy for these tumors, but the necessity and timing of this treatment must be carefully considered. Clearly, operating on asymptomatic tumors may result in unnecessary neurologic damage. Also, it is difficult to know the optimal timing of follow-up imaging. Patients with this disease will undergo frequent abdominal imaging studies for the follow-up or surveillance of renal, adrenal, and pancreatic tumors (6).
A single previous case report (5) has shown that an HB in a patient without VHL progressed from a nodule to a nodule with an enlarging cyst requiring surgery. We have demonstrated these findings in a group of patients with VHL disease. We believe that solid and cystic HBs are the same tumor. Of the four types classically described, we did not find those of type 1 (cyst only) or type 4 (nodule with internal cyst). Several authors indicate that cysts without nodules are rare (2, 4), and in fact, purely cystic tumors likely have tiny nodules associated with them. Some tumors previously described as purely cystic may have had nodules, but these would have not been detected if contrast media were not given. We suspect that the type 4 lesion is an early form of the nodule with an adjacent cyst.
In addition, it is noteworthy that no patient required surgery for solid nodules in the cerebellum. In this group of patients, we found only one solid tumor that grew without associated cystic change, although new solid tumors were detected. Two patients in our group who did not have enough follow-up images to be included in this study underwent surgery for spinal solid tumors. Solid tumors seem to be tolerated less well in the spinal cord than in the cerebellum, presumably because of the smaller dimensions of the cord.
Decisions to perform surgery were made on the grounds of neurologic signs and symptoms attributable to the anatomic location of the tumor. If a tumor is seen to be enlarging and developing a cyst, should early surgery considered? The progressive nature of such tumors described here suggest, “Yes.” However, the number of patients included in this study was small, and a larger prospective study is required before a policy of operating on asymptomatic patients could be advocated.
One patient (Fig 1) underwent aspiration of a cerebellar cyst, but unfortunately, the cyst and symptoms rapidly recurred. Previous reports have documented that cyst aspiration is inadequate therapy (2).
Cysts seem to develop in nodules that are enlarging, as demonstrated in Table 1. The ability to determine the factors initiating cyst formation and to predict this event would be valuable.
Given the fact that no patient without symptoms underwent surgery, we suggest that, after baseline MR imaging, no further CNS imaging is required in the absence of symptoms. The only danger may arise if the nodule is a cystic astrocytoma or metastasis. A compromise policy could involve a single follow-up study at 3 months to exclude rapid tumor enlargement.
Conclusion
In this population of patients with VHL disease, we have demonstrated the enlargement of solid HB nodules and the subsequent development of cysts with these nodules. We surmise that solid cerebellar nodules are well tolerated and that the onset of symptoms heralds the development of such cysts. Repeat imaging is required at this stage to document the size of the cyst and to plan tumor excision. Simple cyst drainage appears to be insufficient for definitive management.
Acknowledgments
We would like to acknowledge the cooperation of the neurosurgical teams at the Oxford Radcliffe Infirmary that were involved in the care of the patients presented in this article.
- Received January 3, 2002.
- Accepted after revision April 24, 2003.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}