
Abstract
BACKGROUND AND PURPOSE: To reduce the door-to-puncture time, which is a prognostic factor for the clinical outcome after intra-arterial recanalization therapy, we established a prehospital telecommunication strategy between neurointerventionalists and emergency medical technicians, namely, the critical stroke call pathway. We retrospectively evaluated the clinical significance of the critical stroke call pathway by comparing the door-to-puncture time and clinical outcome of the critical stroke call pathway with those of the routine stroke pathway.
MATERIALS AND METHODS: From January 2018 to June 2020, one hundred seventy-one patients with anterior circulation occlusion who underwent arterial recanalization therapy via the emergency department were included in this study. Patients were divided into the critical stroke call pathway group (n = 75, 43.9%) and the routine stroke pathway group (n = 96, 56.1%).
RESULTS: The critical stroke call pathway group exhibited a shorter door-to-puncture time than the routine stroke pathway group (median, 87 minutes; interquartile range, 63–107 minutes; P < .001). On multivariable analysis, a good clinical outcome (3-month mRS, 0–2) was independently associated with a shorter door-to-puncture time (adjusted OR, 0.998; adjusted 95% CI, 0.996–1.000; P = .027). In patients with an NIHSS score on admission of ≤11, an excellent clinical outcome (3-month mRS, 0–1) was more frequently achieved in the critical stroke call pathway group than in the routine stroke pathway group (22/33, 66.7%, versus 21/48, 43.8%; P = .042).
CONCLUSIONS: In our study, compared with the routine stroke pathway, the critical stroke call pathway remarkably reduced the door-to-puncture time for arterial recanalization therapy, with better clinical outcomes, especially in patients with a relatively good clinical status.
ABBREVIATIONS:
- CSCP
- critical stroke call pathway
- EMT
- emergency medical technician
- IAT
- intra-arterial recanalization therapy
- IQR
- interquartile range
- RSP
- routine stroke pathway
Intra-arterial recanalization therapy (IAT) has been considered the standard treatment option for acute ischemic stroke caused by large cerebral artery occlusion.1⇓⇓⇓-5 The time from symptom onset to reperfusion is known to be the strongest predictor of clinical outcomes in patients with acute ischemic stroke. The door-to-puncture time is a modifiable factor that can be shortened in the steps from symptom onset to reperfusion.6⇓-8 Recently, the acute ischemic stroke pathway has focused on the communication of a patient’s neurologic status between emergency medical technicians (EMTs) and physicians before arrival at the hospital to reduce the door-to-puncture time.9,10
Communication between EMTs and emergency physicians can help deliver patients with suspected stroke to IAT-capable hospitals by sharing real-time information about emergency department status and IAT availability. However, several steps remain after a patient with suspected stroke arrives at an IAT-capable hospital, and these steps require time for a patient with suspected stroke to receive reperfusion therapy.
In our hospital, the routine stroke pathway (RSP) proceeds as follows: 1) the emergency physician first calls a resident of the neurology department after brain CT of the patient with suspected stroke shows no intracranial hemorrhage; 2) the resident of the neurology department examines the neurologic status of the patient with suspected stroke, performs further imaging studies, and calls a neurologist on duty; 3) the neurologist decides whether to perform IAT and calls a neurointerventionalist; and 4) the neurointerventionalist calls a neurointervention team, including the radiologic technicians and nurses on duty, and prepares the IAT.
To reduce the time these steps take, we established a telecommunication hotline defined as the critical stroke call pathway (CSCP) between EMTs and neurointerventionalists (Fig 1). EMTs responding to calls from patients or patients’ guardians examine the neurologic status of the patients, and communicate with the interventional neurosurgeons via telephone before the ambulance arrives at the hospital. The interventionalist on call, emergency medical doctors, and neurosurgical residents on duty are on standby for the arrival of the patient and EMTs. After a patient with suspected stroke arrives at the hospital, the neurointerventionalist on call examines the patient’s neurologic status and prepares for the possibility of performing IAT with the neurointervention team.

Flow diagrams of the RSP and the CSCP.
If the plain brain CT of the patient with suspected large cerebral artery occlusion shows a high density related to parenchymal hemorrhage, the attending neurointerventionalist calls the on-duty neurosurgeons who decide the treatment technique according to the patient’s neurologic status and brain images. If the image work-up of the patient shows acute cerebral infarction without large-vessel occlusion, antiplatelet medication loading, including aspirin or clopidogrel (Plavix), is administered to the patient. If the image work-up of the patient reveals no lesion, the neurointerventionalist calls the emergency doctors and medical doctors on duty who then manage the patient who presented with a medical condition that mimicked large-vessel occlusion.
This protocol used in our hospital shortened the door-to-puncture time using CT-based decision-making by neurointerventionalists and arrival of the neurointervention team before completion of the image work-up. We hypothesized that the CSCP would reduce the door-to-puncture time for IAT. We also hypothesized that the CSCP would improve clinical outcomes after IAT for patients with acute ischemic stroke.
In this study, we compared the door-to-puncture time and the clinical outcome between the CSCP group and RSP group. We also evaluated factors associated with the clinical outcome in patients who underwent IAT for acute ischemic stroke.
MATERIALS AND METHODS
Study Cohort
From January 2018 to June 2020, two hundred twenty-four patients with large cerebral artery occlusion were treated with IAT via the emergency department in our hospital. Of the 224 patients, 44 patients with posterior circulation occlusions were excluded to ensure study population homogeneity. Nine patients were additionally excluded owing to previous disability (n = 2) and loss to follow-up (n = 7). Therefore, 171 consecutive patients were included in this study.
Because the CSCP is a voluntary system without legal obligation, we could not intentionally select the patients who required IAT and did not know who was included in the CSCP and RSP groups. Patients were divided into 2 groups based on their route to the emergency department. The CSCP group was defined as patients delivered to the emergency department with prehospital telecommunication, and the RSP group was defined as patients delivered to the emergency department without prehospital telecommunication.
Imaging Work-up and Endovascular Treatment
It is not possible to selectively report patients with large-vessel occlusion before vascular imaging. Thus, we evaluated plain brain CT images of the patients with suspected large-vessel occlusion. If there was an absence of high density in these images, we directly called the neurointervention team on call during the evaluation of additional CT neck angiography and CT perfusion in the CSCP group to reduce the door-to-puncture time.
In both the CSCP and RSP groups, patients with suspected stroke were evaluated using CT-based imaging studies, including CT perfusion and CT angiography. If it was difficult to decide whether to perform IAT on the basis of these imaging studies, diffusion-weighted imaging was additionally considered. IAT was generally performed using a hybrid method of combined stent retrieval and catheter aspiration, which we have reported previously.11 When in situ stenosis was observed during IAT, rescue treatments, such as balloon angioplasty or stent placement, were performed.
Data
Patient data were collected from medical records as baseline characteristics, the times of treatment stage, and clinical and radiologic outcomes. The medical records and imaging data were reviewed with the approval of the institutional review board (2020–12-016). Baseline characteristics included age, sex, and medical history, such as diabetes mellitus, hypertension, dyslipidemia, atrial fibrillation, coronary artery occlusive disease, occlusion location, and the NIHSS score on admission. The patient’s NIHSS score on admission was assessed by experienced neurointerventionists (the authors). The times of the treatment were divided into 3 stages: 1) the time from symptom onset to hospital arrival, 2) the door-to-puncture time, and 3) the procedure time. The door-to-puncture time was defined as the time from hospital arrival to groin puncture. The procedure time was defined as the time from groin puncture to recanalization.
The radiologic outcome was assessed by the TICI grade immediately following cerebral angiography. Successful recanalization was defined as a TICI grade of 2b or 3.
The clinical outcome was assessed by the mRS score at 3 months after IAT. The mRS score was estimated by a neurointerventionalist or stroke neurologist during a routinely scheduled clinical visit. A good clinical outcome was defined as a 3-month mRS score of ≤2, and an excellent clinical outcome was defined as a 3-month mRS score of 0 or 1. A 3-month mRS score of ≥3 was defined as a poor clinical outcome.
Statistical Analysis
Baseline characteristics and time of treatment stage were compared between the CSCP and RSP groups and between patients with good clinical outcomes and those with poor clinical outcomes. Univariate analysis was performed using the Mann-Whitney U test for continuous variables and the Pearson χ2 test for categoric variables. Radiologic and clinical outcomes were compared between the CSCP and RSP groups and between the good and poor clinical outcome groups using the Pearson χ2 test. Furthermore, we investigated the variables that were independently associated with good clinical outcomes through a multivariable logistic regression model. Clinically important variables (age, sex, and time of treatment stage) as well as variables with P < .20 in the univariate analysis, suggesting their association with good clinical outcomes, were entered into the model. A stepwise method was used for backward elimination.
The area under the receiver operating characteristic curve was calculated to estimate the optimal threshold of the initial NIHSS score for a good clinical outcome.
Statistical analysis and creation of figures were performed using SPSS, Version 25 (IBM) and Excel (Microsoft). All reported P values < .05 were considered statistically significant.
RESULTS
Of the 171 patients, 86 (50.3%) were men, and the median patient age was 75 years (interquartile range [IQR], 64–80 years). The occlusion locations were as follows: internal carotid artery (n = 47), M1 (n = 86), M2 (n = 32), and anterior cerebral artery (n = 6).
Successful recanalization was achieved in 143 patients (83.6%), and good clinical outcomes were achieved in 103 patients (60.2%). The mortality rate was 5.8% (n = 10). Nine patients had other medical problems such as stomach cancer (n = 1), septic shock (n = 3), and heart failure (n = 5). One patient died from progression of a cerebral infarction with unsuccessful recanalization.
Table 1 shows the comparison between the CSCP and RSP groups. Baseline characteristics except the NIHSS score on admission did not differ significantly between the 2 groups. The NIHSS score on admission was significantly higher in the CSCP group than in the RSP group (median, 14; IQR, 8–18, versus median, 12; IQR, 8–15; P = .049). The CSCP group had a longer time from symptom onset to hospital arrival than the RSP group (median, 171 minutes; IQR, 55–544 minutes, versus median, 92 minutes; IQR, 42–258 minutes); however, the difference was not statistically significant (P = .082). Notably, the door-to-puncture time was significantly shorter in the CSCP group than in the RSP group (median, 87 minutes; IQR, 63–107 minutes, versus median, 142 minutes; IQR, 106–177 minutes; P < .001). The radiologic and clinical outcomes were not significantly different between the 2 groups.
Comparison of baseline characteristics, time of treatment stage, and clinical and radiologic outcomes between CSCP and RSP
A comparison of patients with good clinical outcomes and patients with poor clinical outcomes is shown in Table 2. Patients with poor clinical outcomes were significantly older than those with good clinical outcomes (median, 78 years; IQR, 66–83 years, versus median, 73 years; IQR, 62–78 years; P = .007). The initial NIHSS score was significantly higher in patients with poor clinical outcomes than in patients with good clinical outcomes (median, 14; IQR, 12–18, versus median, 10; IQR, 7–14; P < .001). Successful recanalization was more frequently achieved in patients with good clinical outcomes than in patients with poor clinical outcomes (91/103, 88.3%, versus 52/68, 76.5%), P = .040).
Comparison of baseline characteristics, time of treatment stage, and clinical and radiologic outcomes between the good clinical outcome group and the poor clinical outcome group
Multivariable logistic regression analysis, which included age, sex, atrial fibrillation, coronary artery occlusive disease, initial NIHSS score, occlusion location (right), time of treatment stage, and successful recanalization, showed that good clinical outcome was independently associated with the door-to-puncture time, initial NIHSS score, successful recanalization, occlusion location (right), and atrial fibrillation (Table 3). Additionally, in the patients with an initial NIHSS score of ≤11, multivariable logistic regression analysis showed that a good clinical outcome was independently associated with successful recanalization (adjusted OR, 2.74; 95% CI, 0.087–0.555; P = .008) and the initial NIHSS score (adjusted OR, −2.072; 95% CI, −0.077 to −0.001; P = .042).
Multivariable logistic regression analysis of good clinical outcome
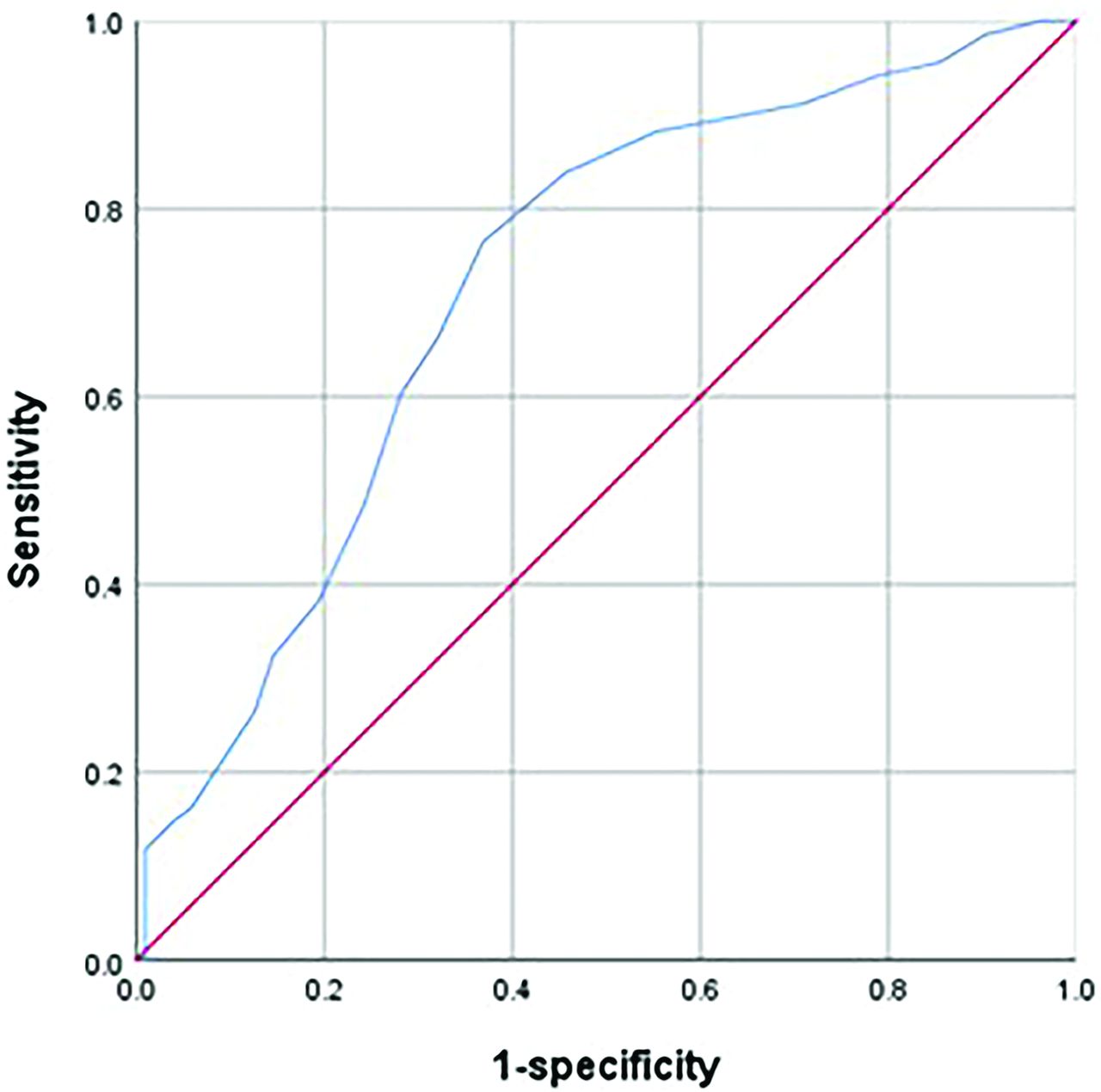
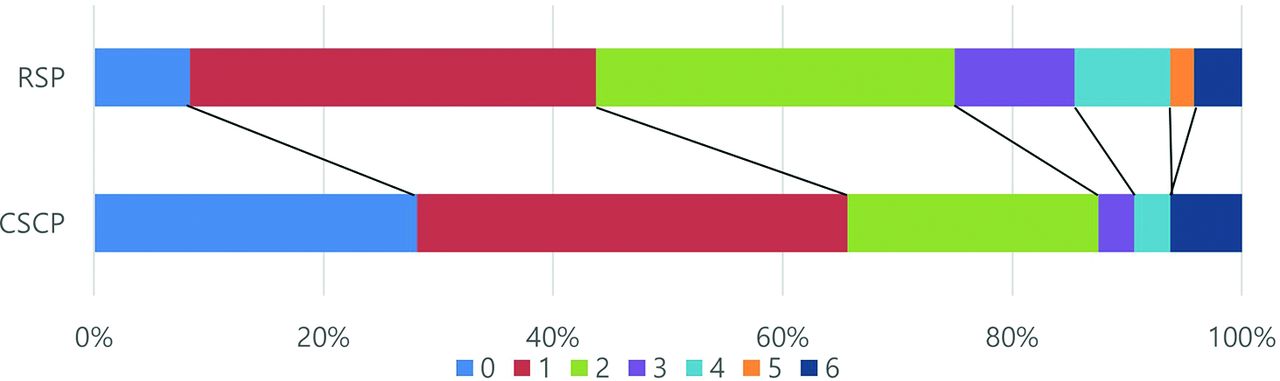
A receiver operating characteristic curve model was constructed between the NIHSS score and good clinical outcome. The area under the receiver operating characteristic curve was 0.719 (95% CI, 0.641–0.796; P <.001). The maximal Youden index J was 0.40 with 76.5% sensitivity and 63.1% specificity (Fig 2), and the optimal threshold of the NIHSS score was 11.5. In the patients with an initial NIHSS score of ≤11, if recanalization was successful, the patient may have a good clinical outcome. However, in patients with an initial NIHSS score of >12, if recanalization was successful, the patient was not expected to have a good clinical outcome based on the analysis of our data. Accordingly, we investigated the patients with an initial NIHSS score of ≤11 to evaluate the difference in good or excellent clinical outcomes between the CSCP and RSP groups. In the patients with an initial NIHSS score of ≤11 who underwent IAT (n = 81), the good clinical outcome of the CSCP group (n = 29/33, (87.9%) was not significantly different from that of the RSP group (n = 36/48, 75.0%) (P = .153). However, the excellent clinical outcome of the CSCP group (n = 22/33, 66.7%) was significantly different from that of the RSP group (n = 21/48, 43.8%) (P = .042) (Fig 3).

Receiver operating characteristic curve of the initial NIHSS score for prediction of a good clinical outcome (mRS = 0–2) at 90 days. The area under the curve of the NIHSS score was 0.714.
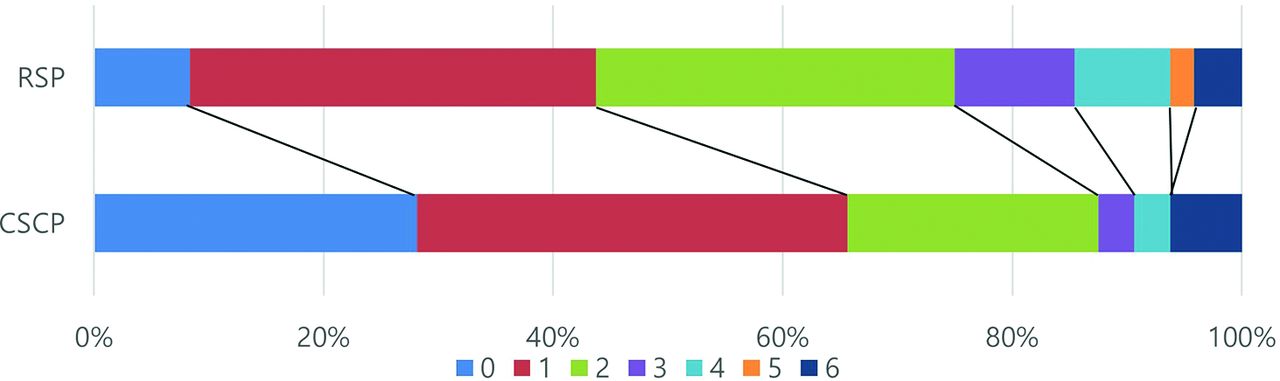
Graph comparing the 90-day mRS scores of the CSCP group and RSP group in the low NIHSS score (≤11 points) group.
DISCUSSION
Recently, the successful recanalization rate has been reported to reach 90% after IAT for patients with acute ischemic stroke using aspiration alone, stent retriever alone, or a combination of these 2 methods.1,2,4,12⇓-14 It seems difficult to develop a new game changer for IAT devices to improve successful recanalization. Therefore, we focused on reducing the door-to-puncture time for IAT to improve clinical outcomes.
A door-to-puncture time within 90 minutes was recently considered an ideal time goal, and many doctors and stroke centers are trying to reach this goal. Our results showed that the median door-to-puncture time of the CSCP group was 87 minutes, which is in line with this time goal. The reduction in the door-to-puncture time in the CSCP group can be explained by reductions in the time required for each step from patient arrival and triage to notification between doctors and preparation for the procedure by the neurointervention team.
In our study, in contrast to our expectations, the CSCP group did not achieve significantly better clinical outcomes than the RSP group (58.7% versus 61.5%, P = .711), despite the difference in the door-to-puncture time. This finding can be partially explained by the difference in the initial NIHSS scores between the CSCP and RSP groups (median, 14; IQR, 8–18, versus median, 12; IQR, 8–15; P = .049). The CSCP group had more severe ischemic injuries than the RSP group at admission, which might have affected the clinical outcomes. Because the patients with a poor neurologic status were not permitted to be delivered to adjacent hospitals for thrombectomy, the EMTs who delivered the patients unavoidably called the neurointerventionalists on call at our hospital, and more patients with an initially poor neurologic status were probably included in the CSCP group. Our multivariable logistic regression analysis also showed that the NIHSS score on admission had a lower OR than the door-to-puncture time (0.790 versus 0.998). This can also explain the clinical outcomes, which were not significantly different between the CSCP and RSP groups, despite the difference in the door-to-puncture times between the 2 groups.
In the patients with an NIHSS score of ≤11 (n = 81), the good clinical outcome of the CSCP group (n = 29/33, 87.9%) was not significantly different from that of the RSP group (n = 36/48, 75.0%) (P = .153). However, the excellent clinical outcome of the CSCP group (n = 22/33, 66.7%) was different from that of the RSP group (n= 21/48, 43.8%) (P = .042). This result suggested that the CSCP group will have a greater possibility of an excellent clinical outcome, especially for patients with NIHSS scores of ≤11.
Our results also showed that the CSCP group had a significantly shorter door-to-puncture time than the RSP group, and a shorter door-to-puncture time was an independent prognostic factor for a good clinical outcome despite the low adjusted OR (0.998). However, the door-to-puncture time based on our results is not a statistically significant cardinal factor for a good clinical outcome. This is probably because the CSCP group had a longer time from symptom onset to hospital arrival than the RSP group (median 171 minutes; IQR, 55–544 minutes, versus median, 92 minutes; IQR, 42–258 minutes). Conclusively, there was no significant difference between the CSCP group (median, 254.5 minutes; IQR, 184.5–485.0 minutes) and the RSP group (median, 254.5 minutes; IQR, 184.5–485.5 minutes) from symptom onset to femoral puncture time (P = .913). Accordingly, the clinical significance of the door-to-puncture time is probably low, unlike our expectation. Nevertheless, our study suggests that prehospital telecommunication between EMTs and neurointerventionalists has clinical significance for good clinical outcomes in patients with acute ischemic stroke.
The limitation of our study is the retrospective design without randomization between the CSCP and RSP groups. However, the selection bias may be low because all patients who underwent IAT during the study period were included. In addition, we tried to treat patients with acute ischemic stroke as quickly as possible, regardless of their route to the emergency department and whether they were in the CSCP or RSP group, reducing the likelihood of selection bias. Additionally, we have not used IV tPA in the patients with large-vessel occlusion within 4.5 hours of symptom onset. Because, there was no beneficial gain of IV tPA administration in patients with large-vessel occlusion treated with thrombectomy, on the basis of our results. Therefore, there was no direct clinical comparison of bridge therapy with IV tPA between the 2 groups. Another limitation of our study is that it was a single-center study with a small sample size. Further studies with large sample sizes are necessary to confirm these preliminary results. Nevertheless, our study could be meaningful because it suggests the clinical significance of prehospital telecommunication between EMTs and neurointerventionalists in improving clinical outcomes as well as reducing the door-to-puncture time.
CONCLUSIONS
Compared with the RSP, the CSCP significantly reduced the door-to-puncture time for IAT, with better clinical outcomes, especially in patients with a relatively good neurologic status. Our study suggests the clinical significance of prehospital telecommunication in the treatment of patients with acute ischemic stroke. Further studies with large sample sizes are necessary to confirm these preliminary results.
Acknowledgment
The authors wish to thank Busan Metropolitan Fire Headquarters, Gijang 119 Safety Center, and Haeundae 119 Safety Center. In particular, they wish to acknowledge the help of Kim JeongHwan and Lee Minho with the Haeundae 119 Safety Center in establishing and fine-tuning the CSCP.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received December 15, 2021.
- Accepted after revision March 21, 2022.
- © 2022 by American Journal of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.