
Abstract
BACKGROUND AND PURPOSE: Current stroke care recommendations for patient selection for mechanical thrombectomy in the extended time window demand advanced imaging to determine the stroke core volume and hypoperfusion mismatch, which may not be available at every center. We aimed to determine outcomes in patients selected for mechanical thrombectomy solely on the basis of noncontrast CT and CTA in the early (<6-hour) and extended (≥6-hour) time windows.
MATERIALS AND METHODS: Consecutive mechanical thrombectomies performed for acute large-vessel occlusion ischemic (ICA, M1, M2) stroke between February 2016 and August 2020 were retrospectively reviewed. Eligibility was based solely on demographics and noncontrast CT (ASPECTS) and CTA, due to the limited availability of perfusion imaging during the study period. Propensity score matching was performed to compare outcomes between time windows.
RESULTS: Of 417 mechanical thrombectomies performed, 337 met the inclusion criteria, resulting in 205 (60.8%) and 132 (39.2%) patients in the 0- to 6- and 6- to 24-hour time windows, respectively. The ASPECTS was higher in the early time window (9; interquartile range = 8–10) than the extended time window (9; interquartile range = 7–10; P = .005). Propensity score matching yielded 112 well-matched pairs. Equal rates of TICI 2b/3 revascularization and symptomatic intracranial hemorrhage were observed. A favorable functional outcome (mRS 0–2) at 90 days was numerically more frequent in the early window (45.5% versus 33.9%, P = .091). Mortality was numerically more frequent in the early window (25.9% versus 17.0%, P = .096).
CONCLUSIONS: Patients selected for mechanical thrombectomy in the extended time window solely on the basis of noncontrast CT and CTA still achieved decent rates of favorable 90-day functional outcomes, not statistically different from patients in the early time window.
ABBREVIATION:
- IQR
- interquartile range
Randomized controlled trials demonstrated that mechanical thrombectomy for anterior circulation large-vessel occlusion strokes provides beneficial outcomes when performed within the early 6-hour time window.1 Among these randomized controlled trials, the Solitaire with the Intention for Thrombectomy as Primary Endovascular Treatment (SWIFT PRIME) and Extending the Time for Thrombolysis in Emergency Neurological Deficits–Intra-Arterial (EXTEND-IA) trials enrolled patients on the basis of ischemic core imaging, whereas the Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands (MR CLEAN) and Mechanical Thrombectomy After Intravenous Alteplase Versus Alteplase Alone After Stroke (THRACE) trials did not. The selection of patients with advanced imaging provided a more favorable absolute treatment benefit.2⇓⇓⇓-6 Nevertheless, due to the safety and efficacy demonstrated in MR CLEAN and THRACE, current guidelines do not recommend advanced imaging as long as the patient presents within the 6-hour time window with a CT-ASPECTS of ≥6 (class I).7 The Endovascular Therapy Following Imaging Evaluation for Ischemic Stroke 3 (DEFUSE-3)8 trial and Diffusion Weighted Imaging (DWI) or Computerized Tomography Perfusion (CTP) Assessment With Clinical Mismatch in the Triage of Wake Up and Late Presenting Strokes Undergoing Neurointervention with Trevo (DAWN)9 trial generated class I evidence for mechanical thrombectomy in the extended 6- to 16-hour time window, while DAWN also expanded to the 16- to 24-hour time window (class IIa). Most important, enrollment in DEFUSE-3 and DAWN was also based on core imaging.8,9 Therefore, to date, patient selection in the extended time window (6–24 hours) demands advanced imaging to determine the stroke core volume and hypoperfusion mismatch (CT perfusion or diffusion-weighted brain MR imaging).
Recently, Nogueira et al10 compared outcomes between patients selected with noncontrast CT and CTA and patients who underwent CT perfusion in the early and extended time windows. They found that the CT perfusion acquisition was associated with better outcomes neither in the early nor extended time window. There is a lack of real-world data on patients selected solely on the basis of noncontrast CT and CTA for the extended time window. Here, we present mechanical thrombectomy outcomes in the early and extended time windows in patients evaluated solely on the basis of noncontrast CT and CTA.
MATERIALS AND METHODS
Consecutive mechanical thrombectomies performed for acute large-vessel occlusion ischemic stroke between February 2016 and August 2020 at comprehensive stroke centers Geisinger Medical Center and Geisinger Wyoming Valley Medical Center were retrospectively reviewed. Local institutional review board approval was obtained before the study initiation.
Patient Selection, Treatment, and Outcome Assessment
Patients were treated according to current American Heart Association/American Stroke Association guidelines except for the limited availability of perfusion imaging during the study period.7,11 Each patient underwent a noncontrast CT scan followed by determination of the ASPECTS. Eligibility for mechanical thrombectomy was based on patient demographics, baseline NIHSS scores, time since symptom onset, and noncontrast CT, including CT-ASPECTS. Scores were obtained by the on-call stroke neurologist and treating neuroendovascular surgeon. None of the patients included underwent advanced imaging beyond noncontrast CT or CTA. Patients transferred from outside hospitals or affiliated primary stroke centers did not undergo additional noncontrast CT or CTA on presentation to the comprehensive stroke center, unless the neurologic status significantly declined during transport or outside imaging was insufficient to facilitate decision-making. Transferred patients were promptly directed to the angiography suite on the basis of imaging provided through the telestroke system. Eligibility for treatment was ultimately determined by the treating neuroendovascular surgeon and adjudicated by the stroke center quality framework. Successful revascularization (TICI 2b/3) was evaluated by the neuroendovascular surgeon. Symptomatic intracranial hemorrhage was assessed according to the Heidelberg Bleeding Classification.12 Functional outcome at 90 days was determined using the mRS, with mRS 0–2 indicating a favorable functional outcome and mRS 6 indicating death.
Statistical Analysis
Categoric variables are given as frequency and percentage. Continuous variables are stated as the median and interquartile range (IQR). Baseline characteristics were compared by means of the χ2, Fisher exact, and Mann-Whitney U tests, as appropriate. Propensity score matching of 0- to 6- versus 6- to 24-hour time windows was performed using age, sex, baseline NIHSS, site of occlusion, and CT-ASPECTS as parameters. Matching was performed using the nearest neighbor method, without replacement and a caliper of 0.1. Subsequent outcome analyses were performed comparing pairs using the McNemar and Wilcoxon signed-rank test. P values of <.05 were considered statistically significant. SPSS, Version 25 (IBM) and R statistical and computing software, Version 4.03 (http://www.r-project.org/) were used to perform statistical analysis.
RESULTS
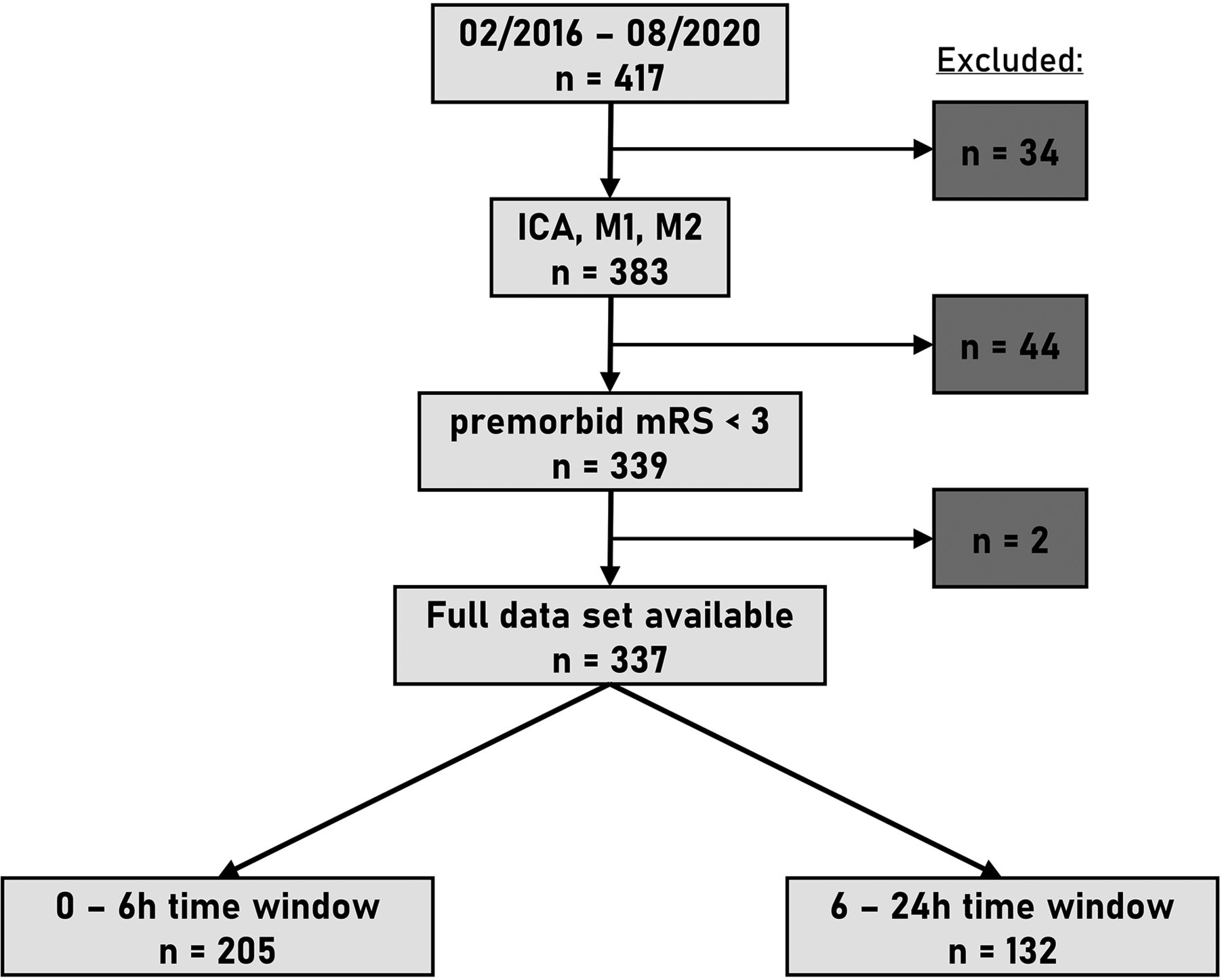
During the study period, February 2016 to August 2020, two hundred thirty-seven/417 (56.8%) mechanical thrombectomies were performed in transferred patients. In the early time window, transferred patients constituted 52.0% of all cases, whereas transferred patients even constituted 63.9% of all cases in the extended time window, thereby demonstrating the challenges of timely stroke management in a health care system that serves a large rural area. Of 417 mechanical thrombectomies performed during the study period, 383 had ICA or MCA (M1 or M2) segment large-vessel occlusions. Forty-four patients with premorbid mRS > 2 and another 2 patients with missing data were excluded. The final dataset comprised 337 cases. Two hundred five (60.8%) were treated within the early 0- to 6-hour time window, and 132 (39.2%), in the extended 6- to 24-hour time window (Fig 1).

Flow sheet patient selection.
Prematch Comparison of Early-versus-Extended Time Windows
Baseline demographics between patients who underwent mechanical thrombectomy in the early (n = 205) and extended (n = 132) time windows in the pre-propensity score–matched comparison were similar except for a higher baseline NIHSS score in the 0- to 6-hour time window (P = .045) (Table 1). CT-ASPECTS was lower in the 6- to 24-hour time window group (P = .005) (Fig 2). Rates of successful revascularization and symptomatic intracranial hemorrhage were similar. A favorable functional outcome was more frequently observed in the early time window (P = .038) (Fig 2). A trend toward more deaths was found in the group with the early time window (P = .052).
Baseline characteristics
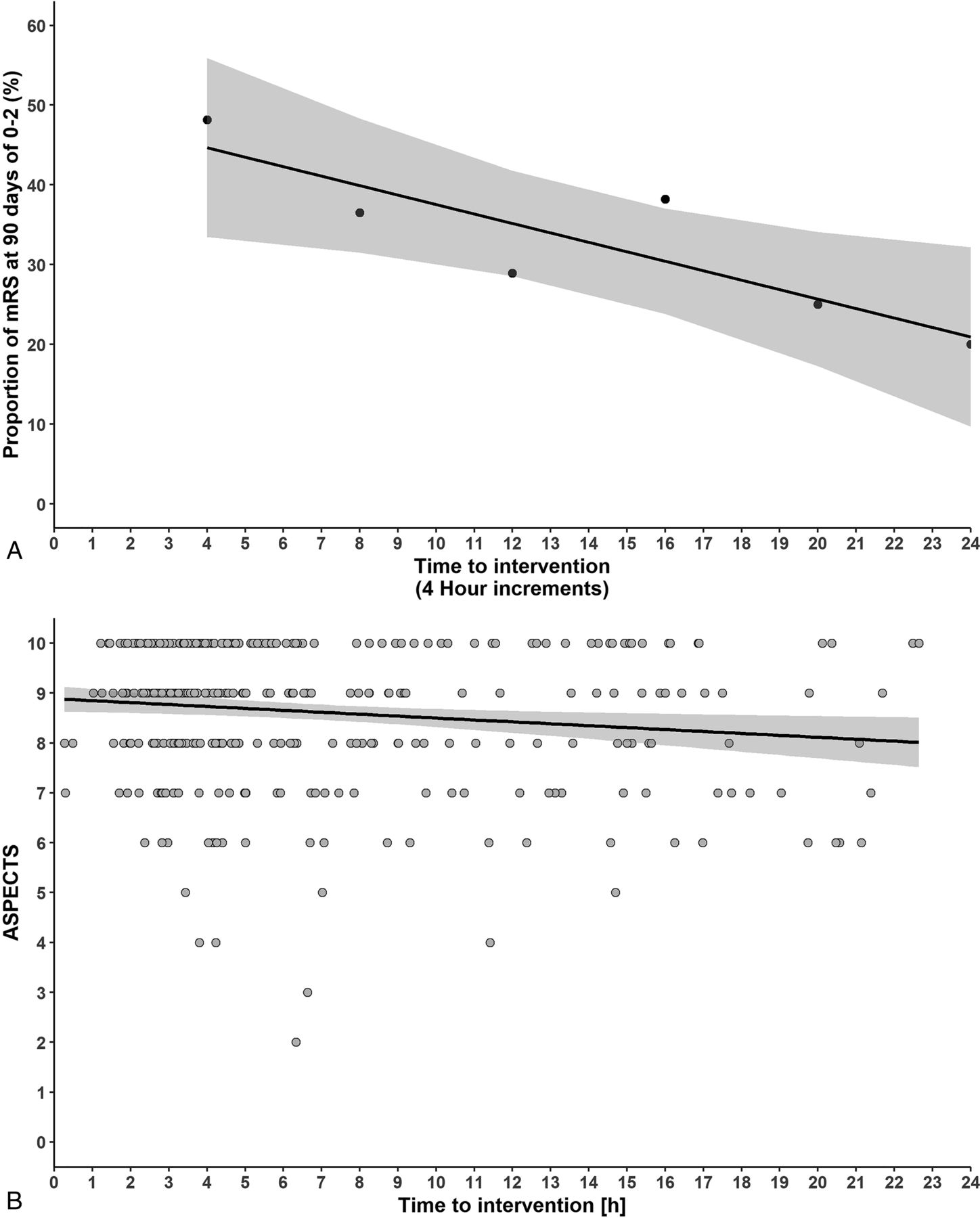
A, Mean proportion of favorable functional outcomes (mRS 0–2) per 4-hour interval of time since symptom onset to intervention, including a trendline. The trendline declines with time. B, CT-ASPECTS of all cases plotted across time from symptom onset to intervention. The trendline remains almost stable with time, representing patient selection based on favorable CT-ASPECTS.
Propensity Matched Comparison of Early-versus-Extended Time Windows
Propensity score matching yielded 112 matched pairs. Standardized mean differences were <0.1. Additional balance measures are provided in Figs 3 and 4. Comparison of the 0- to 6-hour versus 6- to 24-hour groups demonstrated equal distribution of age, sex, baseline NIHSS score, occlusion site, and CT-ASPECTS (Table 2). Outcome analysis showed equal rates of TICI 2b/3 revascularization and symptomatic intracranial hemorrhage. A favorable functional outcome was numerically more frequent in the 0- to 6-hour group than the 6- to 24-hour group (45.5% versus 33.9%), but it was not statistically significant (P = .091). Likewise, death rates were numerically larger in the 0- to 6-hour group than in the 6- to 24-hour group (25.9% versus 17.0%) though they were not statistically significant (P = .096).

Standardized mean differences for covariates integrated into propensity score matching. Prematching (unadjusted) standardized mean differences and postmatching (adjusted) standardized mean differences are shown. Standardized mean difference < 0.1 indicates well-matched samples.

Unadjusted (unmatched) and adjusted (matched) group comparison for the early 0- to 6-hour time window (indicated by 0) and the extended 6- to 24-hour time window (indicated by 1). Density overlay for age, baseline NIHSS, and ASPECTS and equality of height of proportions for female sex and location demonstrate good comparability after propensity score matching.
Propensity score–matched cohort
DISCUSSION
This retrospective cohort provides additional evidence from a real-world setting that clinical evaluation and noncontrast CT-ASPECTS in the extended time window are sufficient to achieve favorable outcome rates. Safety end points for symptomatic intracranial hemorrhage and death at 90 days were similar for both time windows. Likewise, successful revascularization was achieved in >90% regardless of the time windows. A favorable functional outcome was more frequently achieved in the early time window. This observation remained evident even after matching CT-ASPECTS variables, reflecting the predominant role of time in revascularization. However, still, 1 of 3 patients in the extended time window achieved a favorable functional outcome. These observations align with Santos et al,13 who also analyzed a cohort selected solely by noncontrast CT and CTA. They compared 186 patients from the 0- to 6-hour window with 63 patients in the time window beyond 6 hours. While applying strict inclusion criteria (NIHSS > 11, CT-ASPECTS > 6, and premorbid mRS < 2 for the extended time window), the authors observed a favorable functional outcome in 57% and 65.1% in the 0- to 6-hour and beyond the 6-hour time windows, respectively. Mortality and symptomatic intracranial hemorrhage rates were equal across time windows.13
Advanced imaging such as CT perfusion or diffusion-weighted MR imaging allows the preselection of those patients with small cores with a higher likelihood of a beneficial outcome from mechanical thrombectomy. This effect becomes particularly apparent in the extended time window. Patients beyond 6 hours of symptom onset have comparatively small cores, but without intervention, they are not likely to withstand hypoperfusion resulting in cerebral infarction and neurologic decline. Albers14 appropriately illustrated the role of timing and imaging on patient selection together with inherent absolute treatment effects when discussing the late window paradox. Albers postulated that patients who withstand the first 6 hours without significant infarctions (core volumes) have likely a favorable status due to good collateral supply. On the other hand, patients with poor collaterals are very likely to have significant infarctions even in the early time window. Early deteriorators are patients who do not benefit from mechanical thrombectomy despite timely treatment. Patients with poor collateral status and early infarctions are very unlikely to be candidates for mechanical thrombectomy in the extended time window. In contrast, patient selection in the early time window is likely to be more liberal. Therefore, patients selected in the extended time window have an a priori more favorable basis, translating into a relatively benign functional outcome of this particular subgroup.14
CT perfusion imaging performed within 6 hours of symptom onset may overestimate the infarct core.15 Thus, CT perfusion imaging in the early time window requires careful interpretation. For the extended time window, to date, only DEFUSE-3 and DAWN provide class I recommendations. In both trials, patients underwent advanced imaging to screen for core infarct volumes, and patient selection was based on predefined cutoffs.8,9 Despite the awareness of stroke care inequities between urban and rural areas,16 the current literature lacks a discussion on strategies for patients eligible for mechanical thrombectomy requiring long-distance transfers. During the study period, February 2016 to August 2020, two hundred thirty-seven/417 (56.8%) mechanical thrombectomies were performed in transferred patients. Among the early time window, transferred patients constituted 52.0% of all cases, whereas transferred patients even constituted 63.9% of all cases among the extended time window. In our health care system, transfer times regularly exceed 1 hour due to the long distance despite an internal flight air ambulance system. To date, it is unknown whether transferred patients should undergo repeat imaging to update CT-ASPECTS and rule out hemorrhage or even undergo advanced imaging to estimate the infarct core and guide patient selection.
Furthermore, only a subset of affiliated rural hospitals are certified primary stroke centers capable of providing timely advanced imaging. Contrasting the ideal stroke care system incorporating timely transportation and timely availability of advanced imaging with a stroke care system, in large part, also covering rural areas highlights 2 aspects that require reiterated adjudication by stroke quality frameworks. First, suspending advanced imaging should guide patient selection in both the early and extended time windows. Second, delaying mechanical thrombectomy by repeat imaging unless there is severe neurologic decline may result in fatality due to herniation or hemorrhage.
Recently, Nogueira et al10 found CT perfusion–based patient selection not superior to standardized noncontrast CT and CTA in terms of functional-outcome prediction. These observations, together with real-world data such as presented in the current study, challenge the demand for advanced imaging to guide patient selection and justify patient selection based purely on favorable CT-ASPECTS, even in the extended time window. The selection of patients with favorable CT-ASPECTS is shown in Fig 2. Notably, the selection of patients with large-vessel occlusion for mechanical thrombectomy using advanced imaging may increase the relative proportion of patients achieving functional independence but might compromise the absolute number of patients potentially benefitting from this treatment by excluding patients who might have benefitted.
Lowering the threshold for performing mechanical thrombectomy has also been debated for patients presenting with poor CT-ASPECTS such as CT-ASPECTS < 6. In this context, older age and large-core infarcts do not uniformly present a contraindication for mechanical thrombectomy. Instead, a subset of patients with large-core infarcts undergoing mechanical thrombectomy still achieve a favorable functional outcome.17⇓⇓⇓–21 Whether sparing of either the deep or superficial MCA territories provides a better outcome is still controversial.22,23 Partial reperfusion of distinct areas such as the motor-eloquent cortical area appears to outweigh the degree of partial reperfusion.24 It remains uncertain whether advanced imaging would identify these patients better or exclude patients who could benefit.
Mechanical thrombectomy beyond the 6-hour time window with patient selection based on advanced imaging appears cost-effective.25,26 Providing timely interpretation of perfusion-based advanced imaging modalities has been challenging for every stroke center. It has led to the development of outsourced solutions and automated interpretation platforms. However, standardized cloud-based services to assess core and penumbra on CT or MR perfusion are associated with a substantial financial burden. This study shows that selection of patients with large-vessel occlusion strokes for thrombectomy with favorable CT-ASPECTS even in the extended time window is feasible, without using advanced imaging modalities.
In summary, absolute treatment effects become lower with less stringent preselection criteria. However, withholding mechanical thrombectomy due to lack of advanced imaging does not appear justifiable for those patients with favorable CT-ASPECTS irrespective of the time window. Additional investigation is required to determine the value of advanced imaging in patients in extended time windows and those with large-core infarcts on presentation.
Limitations
Its sample size and retrospective design limit this study. There is no randomization or comparative control group for the time-window groups. The study does not provide the number of patients that ultimately did not undergo mechanical thrombectomy, which, specifically for the late window, needs to be considered. Here, patient selection is based on the decision of the stroke care team. Finally, the study does not provide specific demographic, neurologic, or radiologic criteria (such as collateral scores), finally leading to a decision for or against mechanical thrombectomy in the late time window.
CONCLUSIONS
Patients selected for mechanical thrombectomy in the extended time window solely on the basis of noncontrast CT and CTA still achieved decent rates of favorable 90-day functional outcomes not statistically different from those in patients in the early time window. However, additional investigation is required to determine the value of advanced imaging in the extended time window, specifically if advanced imaging is associated with further delay when serving patients from rural areas with long-distance transfers.
Footnotes
P. Hendrix received salary support from Geisinger and Medtronic.
Previously presented as an abstract at: Annual Meeting of the Society of Neurointerventional Surgery, July 26–30, 2021; Colorado Springs, Colorado.
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received May 22, 2021.
- Accepted after revision June 29, 2021.
- © 2021 by American Journal of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Tenecteplase versus alteplase before mechanical thrombectomy: experience from a US healthcare system undergoing a system-wide transition of primary thrombolytic
- Stroke imaging modality for endovascular therapy in the extended window: systematic review and meta-analysis
- Association between time to treatment and clinical outcomes in endovascular thrombectomy beyond 6 hours without advanced imaging selection