
Abstract
BACKGROUND: Research on the presence of sex-based differences in the outcomes of patients undergoing endovascular thrombectomy for acute ischemic stroke has reached differing conclusions.
PURPOSE: This review aimed to determine whether sex influences the outcome of patients with large-vessel occlusion stroke undergoing endovascular thrombectomy.
STUDY SELECTION: We performed a systematic review and meta-analysis of endovascular thrombectomy studies with either stratified cohort outcomes according to sex (females versus males) or effect size reported for the consequence of sex versus outcomes. We included 33 articles with 7335 patients.
DATA ANALYSIS: We pooled ORs for the 90-day mRS score, 90-day mortality, symptomatic intracranial hemorrhage, and recanalization.
DATA SYNTHESIS: Pooled 90-day good outcomes (mRS ≤ 2) were better for men than women (OR = 1.29; 95% CI, 1.09–1.53; P = <.001, I2 = 56.95%). The odds of the other outcomes, recanalization (OR = 0.94; 95% CI, 0.77–1.15; P = .38, I2 = 0%), 90-day mortality (OR = 1.11; 95% CI, 0.89–1.38; P = .093, I2 = 0%), and symptomatic intracranial hemorrhage (OR = 1.40; 95% CI, 0.99–1.99; P = .069, I2 = 0%) were comparable between men and women.
LIMITATIONS: Moderate heterogeneity was found. Most studies included were retrospective in nature. In addition, the randomized trials included were not specifically designed to compare outcomes between sexes.
CONCLUSIONS: Women undergoing endovascular thrombectomy for large-vessel occlusion have inferior 90-day clinical outcomes. Sex-specific outcomes should be investigated further in future trials as well as pathophysiologic studies.
ABBREVIATIONS:
- EVT
- endovascular thrombectomy
- HRT
- hormone replacement therapy
- RCT
- randomized controlled trial
- rtPA
- recombinant tissue plasminogen activator
- sICH
- symptomatic intracranial hemorrhage
Differences in the treatment and outcomes between women and men with cardiovascular disease are well-documented in the literature. Women undergoing percutaneous coronary interventions have higher hospital mortality rates and complications compared with men.1 For stroke, men had a higher incidence, but female patients with stroke were more severely ill.2 A large series spanning 10 years found that women were less likely to receive IV recombinant tissue plasminogen activator (rtPA) and were also less likely to be enrolled in a clinical trial.3 More recently, however, a review suggested that the disparity between women and men in the rate of IV rtPA administration was no longer apparent in more modern cohorts.4
The advent of endovascular thrombectomy (EVT) ushered in a new era in the treatment of large-vessel ischemic stroke. Sex-specific outcome analysis of the Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands (MR CLEAN), a randomized controlled trial (RCT) that demonstrated the superiority of endovascular thrombectomy over best medical management, showed that there were no statistically significant treatment effects of EVT for women in terms of 90-day functional outcomes.5 On the other hand, a meta-analysis of all the landmark trials for EVT did not show any differences between women and men in terms of outcomes.6 However, the latest evidence on the subject comes from the largest real-world cohort of 2399 patients, which shows that women were less likely to receive EVT and be functionally independent at 90 days.7 Our systematic review primarily aimed to determine whether sex influences the 90-day clinical outcomes of patients with large-vessel ischemic stroke undergoing EVT. We also examined symptomatic intracranial hemorrhage (sICH), 90-day mortality, and recanalization rate.
MATERIALS AND METHODS
A systematic review with a meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA).8
Search Strategy, Information Sources, and Study Selection
Electronic searches were performed using Ovid MEDLINE, PubMed, the Cochrane Central Register of Controlled Trials, the Cochrane Database of Systematic Reviews, the American College of Physicians Journal Club, and the Database of Abstracts of Reviews of Effectiveness from their dates of inception to March 21, 2020 (Online Supplemental Data). To achieve maximum sensitivity of the search strategy, we combined the following terms: “stroke,” “thrombectomy,” “endovascular,” “ADAPT,” “sex,” as either keywords or Medical Subject Headings terms. The reference lists of all retrieved articles were reviewed for further identification of potentially relevant studies. Authors of studies with incomplete data were also contacted by e-mail. All identified articles were systematically assessed using the inclusion and exclusion criteria.
Study Eligibility
Eligible studies for the present systematic review and meta-analysis included cohorts of patients with acute ischemic stroke who were treated with an endovascular approach, including stent-retrieval maneuvers or aspiration thrombectomy. Specifically, the studies included in this review must have included either stratified cohort outcomes according to sex (females versus males) or reported an effect size for the consequence of sex versus outcomes reported. If the proportion data were not available, then effect size either in the form of odds ratio, relative risk, or hazard ratio with 95% confidence intervals was collected. Studies must have included data on our desired outcomes: 90-day clinical outcomes according to the mRS score, recanalization rate according to the modified TICI, 90-day mortality, and sICH.
To capture modern thrombectomy results, we excluded studies published before January 1, 2015. When institutions published duplicate studies with accumulating numbers of patients or increased lengths of follow-up, only the most complete reports were included for quantitative assessment at each time interval. All publications were limited to those involving human subjects in the English language. Studies with <10 patients, abstracts, case reports, conference presentations, editorials, reviews, and expert opinions were excluded.
Risk of Bias
We included 31 observational studies (3 prospective, 28 retrospective), 1 RCT, and 1 meta-analysis6 of individual patient data from the landmark RCTs (MR CLEAN, ESCAPE, REVASCAT, EXTEND IA, SWIFT PRIME, THRACE, and PISTE) on EVT. None of the RCTs were randomized according to sex. We used the Newcastle-Ottawa Assessment Scale for Cohort Studies for the observational studies.9 The RCTs and the meta-analysis of individual patient data of RCTs were assessed using the Cochrane Collaboration tool for assessing the risk of bias in randomized trials.10 The 7 RCTs included in the meta-analysis were also assessed individually. All studies had a low-to-moderate degree of bias (Online Supplemental Data).
Data Collection Process
Two physicians (J.C.K. and J.D.B.D.) independently searched and reviewed the selected studies. Data were extracted and documented on a predesigned spreadsheet (Excel for Mac, Version 16.28; Microsoft) with the following variables of interest: first author, title, year of publication, study location, study design, sample size, age, number of women, NIHSS score, use of IV rtPA, TICI 2b–3, recanalization, 90-day mRS, and sICH. Any disagreements with data extraction and article appraisal were settled by a third independent reviewer (A.A.D.). The severity of stroke was classified according to the NIHSS score based on the most common classification system used in the literature: A score of <8 was classified as mild; 8–16, as moderate; and >16, as severe stroke.11
Statistical Analysis
The statistical analysis was performed by 2 of the authors (A.A.D., N.H.). All analyses were conducted in OpenMeta [Analyst] (http://www.cebm.brown.edu/openmeta/download.html) and R statistical and computing software, Version 3.5.0 (metafor package 2.0–0; https://metafor-project.org/doku.php). Statistical significance was considered with a 2-tailed P value ≤ .05. Unadjusted OR risk and 95% confidence intervals were reported to pool the effect of sex on thrombectomy outcomes. Interstudy heterogeneity was estimated using the Higgins I2; ≤25% denoted low, 25% to 50% denoted moderate, and >50% denoted high heterogeneity.12 In cases of high heterogeneity, random-effects models were used. Otherwise, fixed-effect models were used. In light of the high residual heterogeneity, univariate and multivariate meta-regression analyses were performed to identify potential confounders contributing to the heterogeneity. All the variables included in the meta-regression analyses were demographics, study characteristics, or preoperative variables. Specifically, for multivariate meta-regression analyses, only variables with ≥8 included studies were included in the model.10 To examine potential publication bias, we constructed funnel plots, and Egger and Begg and Mazumdar rank correlation tests were used for each primary outcome.
RESULTS
After removing duplicates, we identified 2885 studies for screening. Of these, 55 full-text articles were assessed. A total of 33 articles that met our inclusion and exclusion criteria were included in the final analysis (Online Supplemental Data). The PRISMA diagram of the study selection process is presented in the Online Supplemental Data. All the studies had a low-to-moderate degree of risk of bias (Online Supplemental Data).
Among the 7335 included subjects, the average age was 69.3 years (range, 61.5–84.8 years), and 47.4% of the subjects were women (range, 33.6%–67.0%). On the basis of the NIHSS score, 12 studies had moderate-severity stroke at baseline (range, 13–16), while 12 studies had severe stroke (range, 17–21); 50.1% of the subjects had received IV rtPA before thrombectomy (range, 11%–100% of subjects); and 74.8% had a TICI 2b–3 (range, 50%–100% of subjects) post-EVT radiologic outcome.
Primary Outcomes
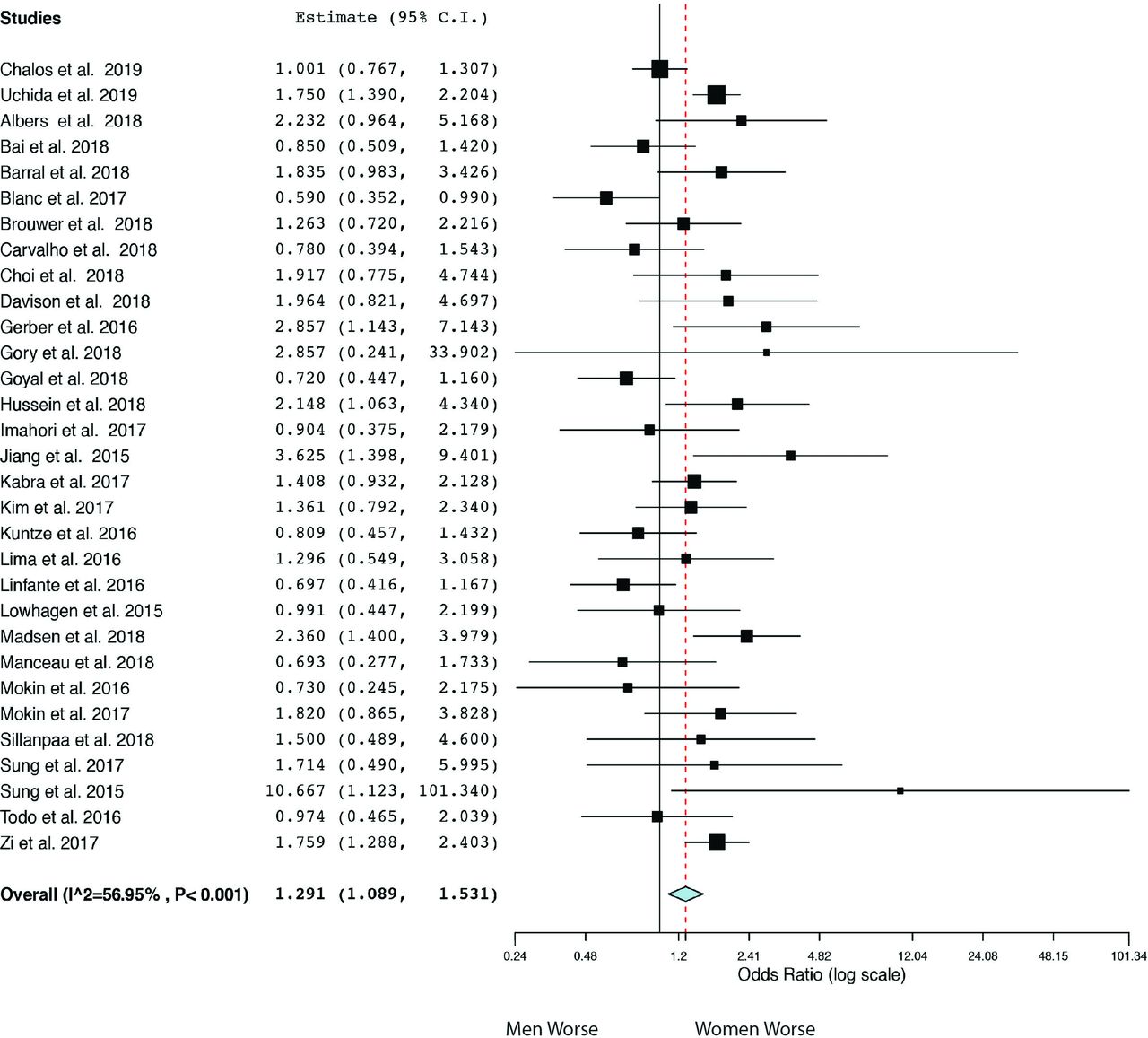
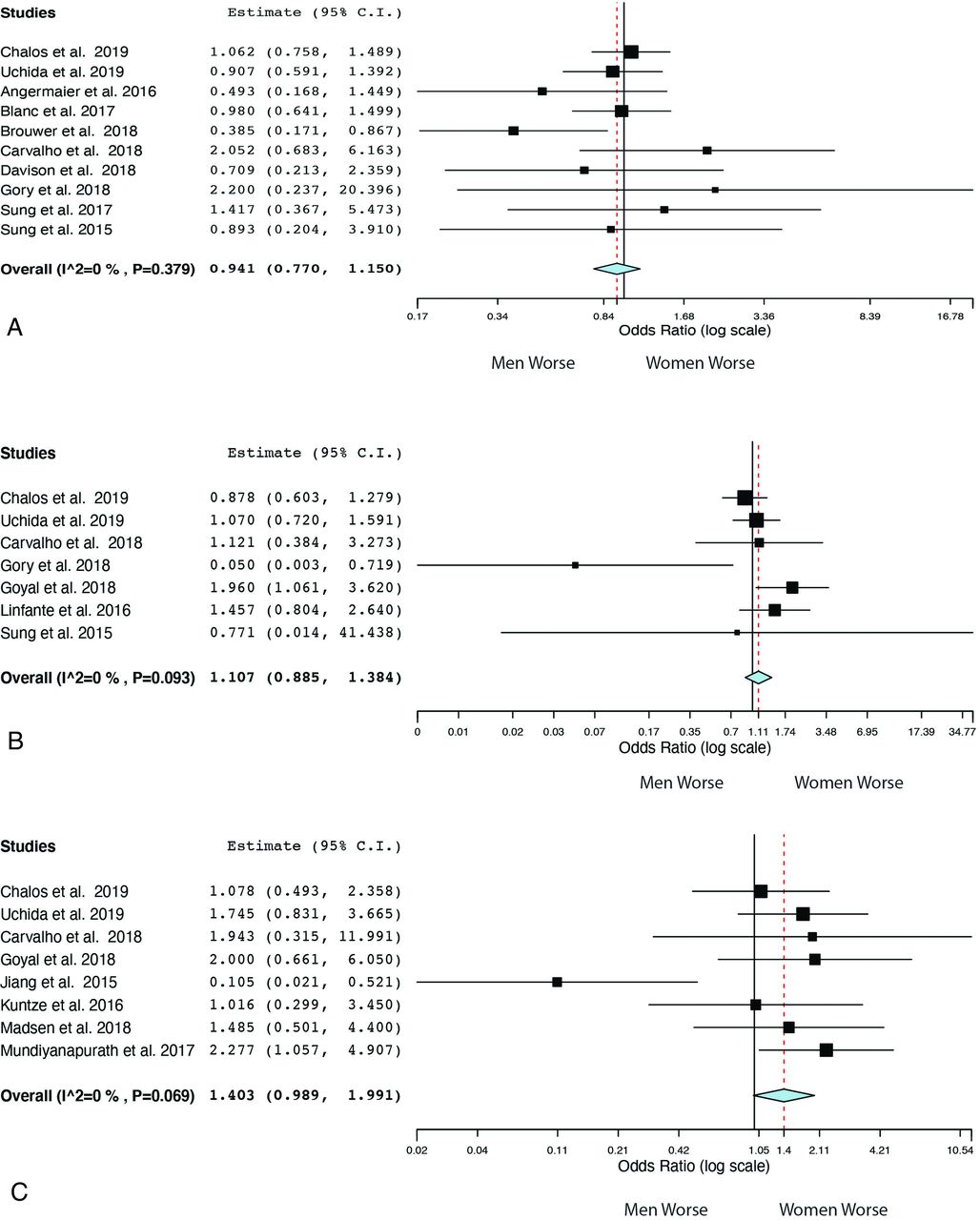
Pooled 90-day good outcomes were better for men than women (n = 31, OR = 1.29; 95% CI, 1.09–1.53; P = <.001, I2 = 56.95%) (Fig 1). By contrast, the odds of the other outcomes, recanalization (n = 10, OR = 0.94; 95% CI, 0.77–1.15; P = .38, I2 = 0%), 90-day mortality (n = 7, OR = 1.11; 95% CI, 0.89–1.38; P = .093, I2 = 0%), and sICH (n = 8, OR = 1.40; 95% CI, 0.99–1.99; P = .069, I2 = 0%), were comparable between men and women (Fig 2). Because the heterogeneity tests showed that 90-day mortality (df = 6, I2 = 44.73%, P = .093), sICH (df = 7, I2 = 46.71%, P = .069), and recanalization (df = 9, I2 = 6.83%, P = .379) had low-to-moderate heterogeneity, the fixed-effect model was used in keeping with the Cochrane recommendations for meta-analysis.

Forest plot of meta-analysis results for good functional outcome (mRS ≤ 2) at 90 days

Forest plot for secondary outcomes. A, Recanalization (TICI ≥ 2b). B, Mortality at 90 days. C, sICH.
Meta-Regression Analysis
In univariate meta-regression analysis, IV rtPA (n = 5, P = .028) was positively associated with sICH, whereas the NIHSS score (n = 5, P = .040) was inversely associated with sICH. Although no variables had a significant association with good outcome in univariate analysis, age (P = .003) and male sex (P < .001) were positively associated with good outcome, after adjusting for IV rtPA and year of publication. When the variable IV rtPA was replaced by TICI 2b–3, age (P = .045) and male sex (P = .0084) were still positively associated with good outcome.
Publication Bias
Publication bias was assessed by visually inspecting funnel plots. For good outcome, sICH, and recanalization, the plots were symmetric and with minimal extreme values. Publication bias in these outcomes was interrogated by Egger and Begg as well as Mazumdar rank correlation tests, and found to be insignificant. For 90-day mortality, although the funnel plot was asymmetric, both Egger and Begg and Mazumdar rank correlation tests did not suggest potential publication bias (Online Supplemental Data).
DISCUSSION
Our meta-analysis demonstrates that women are less likely to attain good 90-day functional outcomes (mRS 0–2) compared with men. The 2 groups did not vary in terms of sICH and 90-day mortality and recanalization rates.
Women have an overall lower lifetime incidence of stroke compared with men. This has been attributed principally to the cardiovascular protective effects of estrogen and progesterone in younger women.13 However, starting at about 45 years of age, the pattern is reversed.14 Experimental rat models mimicking middle cerebral artery stroke have found consistent results. Aged female rats with lower levels of estrogen had significantly larger infarcts compared with the other groups (aged male rats, young male and female rats).15 The identification of pathomechanisms underlying this phenomenon may help identify molecular targets for sex-based neuroprotection in the future.
In a pooled, sex-based matched analysis among patients receiving IV rtPA for stroke in randomized controlled trials, no overall difference was seen in the outcome of patients between women and men.16 However, when inspecting the probability of obtaining a good outcome across age groups in the same cohort, women fared better than men before the age of 45 but had poorer outcomes after that. This finding provides further evidence for the effect of age on sex differences in stroke. A meta-analysis of 60,159 patients on this topic found that women had worse clinical outcomes compared with men after thrombolysis.17 Higher levels of plasminogen activator inhibitor 1, a known predictor of thrombolysis resistance, in female patients with stroke was theorized to underlie these outcomes.18
However, differences in baseline characteristics between sexes may also account for inferior functional outcomes in women. The largest cohort included in the analysis also showed poorer outcomes in women. However, women in the study were also older and presented with worse strokes (higher NIHSS scores and lower ASPECTS). Nevertheless, the inferior functional outcomes remained after adjusting for the aforementioned factors.7 The use of hormone replacement therapy (HRT) was a risk factor not routinely collected in the studies included in our meta-analysis. The use of HRT has been found to decrease the levels of plasminogen activator 1.19 Intuitively, HRT should be protective for stroke. However, large randomized trials on the use of HRT for both primary and secondary prevention of cardiovascular disease have revealed that its use likely increases the risk of stroke and stroke-related death.20,21 How HRT affects the response of the female brain to recanalization and reperfusion after EVT remains to be elucidated. Thus, HRT use may ultimately be another important factor worth noting in future studies focused on sex-based differences in EVT for stroke.
This meta-analysis has several limitations. First, moderate heterogeneity was found. Next, there is also bias inherent in the retrospective nature of most studies included. None of the studies including the randomized trials were specifically designed to compare outcomes between sexes. Thus, differences in the baseline characteristics of both groups may have led to poorer functional outcomes in women undergoing EVT. Last, the definition of sICH was not uniform throughout all the studies included.
CONCLUSIONS
This sex-based meta-analysis of patients with stroke undergoing EVT suggests that women have inferior clinical outcomes at 90 days compared with men. Large-scale prospective cohorts with attention to sex and reporting of these outcome data would be instrumental in interrogating this disparity. Studies on the pathophysiology and/or systems-based cause of this phenomenon would also help to create alleviation strategies.
Footnotes
Disclosures: Thomas R. Marotta—UNRELATED: Consultancy: Medtronic, proctor for the Pipeline Endovascular Device; Patents (Planned, Pending or Issued): EVASC, for eCLIPS; principal medical advisor; Stock/Stock Options: EVASC.
References
- Received October 8, 2020.
- Accepted after revision November 25, 2020.
- © 2021 by American Journal of Neuroradiology




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Sex differences in outcomes after endovascular treatment in posterior circulation stroke: results from the MR CLEAN Registry
- Sex differences in onset to hospital arrival time, prestroke disability, and clinical symptoms in patients with a large vessel occlusion: a MR CLEAN Registry substudy
- Sex differences in outcomes after mechanical thrombectomy for acute ischemic stroke in the 'real world: protocol for a systematic review and meta-analysis study