
Abstract
BACKGROUND: Severe carotid stenosis carries a high risk of stroke. However, the risk of stroke with nonstenotic carotid plaques (<50%) is increasingly recognized.
PURPOSE: We aimed to summarize the risk of TIA or stroke in patients with nonstenotic carotid plaques.
DATA SOURCES: We performed a comprehensive systematic review and meta-analysis in patients with acute ischemic stroke in whom carotid imaging was performed using MEDLINE and the Cochrane Database, including studies published up to December 2019.
STUDY SELECTION: Included studies had >10 patients with <50% carotid plaques on any imaging technique and reported the incidence or recurrence of ischemic stroke/TIA. High-risk plaque features and the risk of progression to stenosis >50% were extracted if reported.
DATA SYNTHESIS: We identified 31 studies reporting on the risk of ipsilateral stroke/TIA in patients with nonstenotic carotid plaques. Twenty-five studies (n = 13,428 participants) reported on first-ever stroke/TIA and 6 studies (n = 122 participants) reported on the recurrence of stroke/TIA.
DATA ANALYSIS: The incidence of first-ever ipsilateral stroke/TIA was 0.5/100 person-years. The risk of recurrent stroke/TIA was 2.6/100 person-years and increased to 4.9/100 person-years if intraplaque hemorrhage was present. The risk of progression to severe stenosis (>50%) was 2.9/100 person-years (8 studies, n = 448 participants).
LIMITATIONS: Included studies showed heterogeneity in reporting stroke etiology, the extent of stroke work-up, imaging modalities, and classification systems used for characterizing carotid stenosis.
CONCLUSIONS: The risk of recurrent stroke/TIA in nonstenotic carotid plaques is not negligible, especially in the presence of high-risk plaque features. Further research is needed to better define the significance of nonstenotic carotid plaques for stroke etiology.
ABBREVIATIONS:
- ASyNC
- asymptomatic nonstenotic carotid plaques
- ESUS
- embolic stroke of undetermined source
- PICOS
- Population, Intervention; Control or comparator; Outcomes
- SyNC
- symptomatic nonstenotic carotid plaques
- ECST
- European Carotid Surgery Trial
The etiology of acute ischemic stroke is crucial to guide further management and for the prevention of recurrent events. Carotid stenosis as the underlying etiology is found in up to 20% of cerebrovascular ischemic events.1,2 Current American Heart Association/American Stroke Association guidelines recommend carotid revascularization only in patients with symptomatic carotid stenosis of >50%.3 This recommendation is supported by data from the European Carotid Surgery Trial (ECST) and North America Symptomatic Carotid Endarterectomy Trial (NASCET), which showed a significant reduction of future strokes after revascularization of symptomatic severe carotid stenoses but modest benefit in moderate stenoses.4,5 Thus, the management of symptomatic patients with <50% stenosis is undetermined. In addition, the risk of stroke and TIA with carotid plaques of <50% is not well-defined, though recent evidence suggests their potential role in stroke,6⇓⇓-9 especially in those classified as cryptogenic. Moreover, certain morphologic features of carotid plaques are independent risk factors of stroke/TIA, irrespective of the degree of stenosis.6,10,11 In a recent meta-analysis, mild carotid stenosis with “high-risk plaque features” was significantly more common in patients with an embolic stroke of undetermined source (ESUS) ipsilateral to the side of stroke compared with the contralateral side.12 Moreover, there are studies proposing carotid revascularization as a treatment option in patients with nonstenotic carotid plaques with recurrent ipsilateral strokes despite adequate medical treatment.13,14
We conducted a meta-analysis to estimate the risk of incident ischemic stroke/TIA in asymptomatic nonstenotic carotid plaques (ASyNC) as well as the risk of recurrent stroke/TIA in patients with symptomatic nonstenotic carotid plaques (SyNC).
MATERIALS AND METHODS
Our strategy to address the primary question above was informed by the Population, Intervention; Control or comparator; Outcomes (PICOS) framework recommended by the Cochrane Collaboration Handbook for Systematic Reviews of Interventions.15 Details are provided in the On-line Appendix.
Briefly, we included studies of individuals with asymptomatic or symptomatic nonstenotic carotid plaques (<50%) measured with any imaging technique (sonography/CT angiography/MR angiography/DSA). The primary outcome was the future risk of stroke/TIA in the ASyNC group and the risk of recurrent stroke/TIA in those with symptomatic nonstenotic carotid plaques. Retinal ischemic events (such as amaurosis fugax) were infrequently mentioned in the included studies and, if mentioned, were included in the subgroup of TIAs.
Search Strategy
We performed and reported this review according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.16 We registered our protocol a priori in the PROSPERO international prospective register of systematic reviews (https://www.crd.york.ac.uk/PROSPERO; No. 162497). Data were collected from published studies; hence, ethics approval and consent were not required.
Our primary question was to describe the natural history of ASyNC and the risk of recurrent stroke/TIA in patients with symptomatic nonstenotic carotid plaques (SyNC). Natural history incorporates both the risk of ischemic stroke/TIA on follow-up and the risk of progression to severe stenosis in patients with asymptomatic, nonstenotic carotid plaques. We defined nonstenotic carotid plaques as carotid plaques with <50% stenosis. SyNC was defined as a carotid plaque with <50% luminal stenosis and an ipsilateral stroke/TIA. In studies that grouped patients into <30%, 30%–70%, and >70% stenosis, only the group of patients with <30% stenosis was included in the analysis to avoid overestimation of the predefined outcome by including a subgroup of patients with 50%–70% carotid stenosis.
Secondary questions included the effects of plaque features on the risk of stroke/TIA. Plaque features include intraplaque hemorrhage, lipid-rich necrotic core, ulceration, fibrous cap, calcification, and thrombus. Additionally, we aimed to assess whether treatment affects the risk of future or recurrent ischemic stroke/TIA. Treatments included medical (antiplatelets, statins) and interventional (endarterectomy or stent placement) management. Details of the framework, search strategy, study selection with inclusion and exclusion criteria, and bias assessment, including publication bias, are mentioned in the On-line Appendix (On-line Figs 1–7).
Statistical Analysis
Analyses were performed using STATA/IC, Version 14.0 (StataCorp). The meta-analyses were performed using a random-effects model of variance. Heterogeneity was calculated using the Higgins I2 statistic (with associated P values). We also evaluated the primary outcomes through subgroup analyses using a stratified random-effects meta-analysis. Publication bias was assessed using the Egger test.
RESULTS
Summary findings of key data-extraction elements are presented in On-line Tables 1 and 2.
Risk of First-Ever Stroke/TIA in Asymptomatic Nonstenotic Carotid Plaques
Of the total 25 studies involving 24,847 participants (18 prospective, 2 randomized trials, 6 retrospective), the mean age was 67.5 years (range, 58.1–78.7 years), and men represented 50.4%. The classification of stroke etiology using the Trial of Org 10172 in Acute Stroke Treatment criteria was mentioned in only 3 studies.17-19 Grading of the degree of stenosis was predominantly based on the NASCET criteria5 and other United States–based classification systems. The average follow-up, reported in 20 studies, was 4.8 years.
Of 24,847 participants, 13,428 (54%) had ASyNC at baseline; the remaining 11,419 (45.9%) were not included in the analysis because they either had no stenosis or were classified into a 30%–70% stenosis group in the study. During a mean follow-up of 4.4 years, 730 subjects (5.4%) with ASyNC developed ischemic stroke/TIA. The incidence rate of stroke/TIA in ASyNC was 0.5/100 person-years (Fig 1).

Incidence rate (per 100 person-years) of stroke in patients with ASyNC. ES indicates effect size.
Risk of Recurrent Stroke/TIA in Symptomatic Nonstenotic Carotid Plaques
Of a total of 680 participants with SyNC in 14 studies, the mean age was 70.2 years, and most were men (n = 454, 66.7%). Classification per the Trial of Org 10172 in Acute Stroke Treatment criteria was mentioned in 8 studies.6,20⇓⇓⇓⇓⇓-26 Most studies (n = 9) used the NASCET criteria5 to define the degree of stenosis.
Six studies8,13,14,20,27,28 (n = 122) reported recurrence of ischemic stroke/TIA (n = 20, 16.4%) during a mean follow-up of 3.1 years. The incidence rate of recurrent stroke in this population was 2.6/100 person-years (Fig 2).

Incidence rate (per 100 person-years) of recurrent stroke in patients with SyNC. ES indicates effect size.
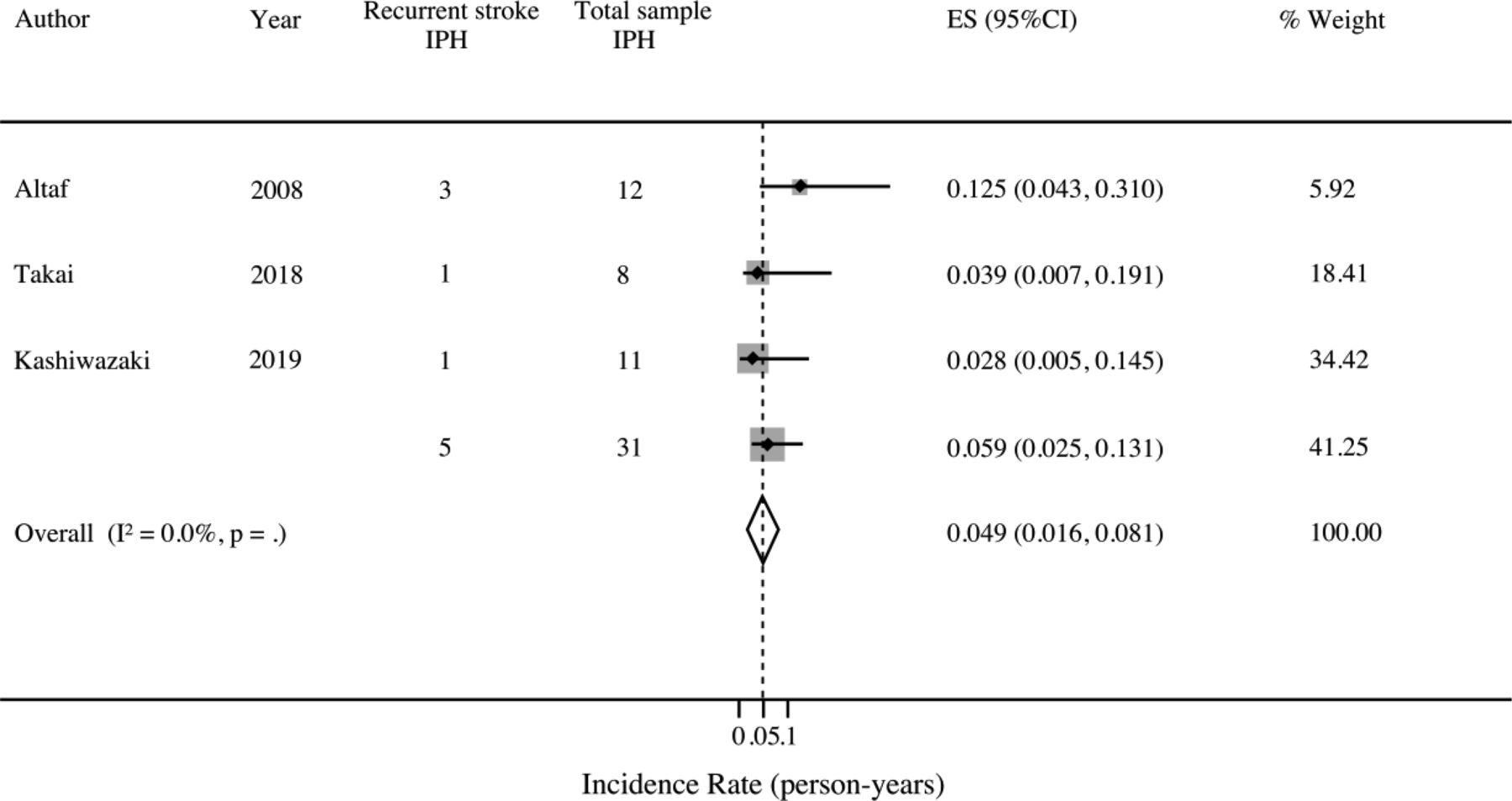
All except 4 studies13,14,20,27 reported plaque features that were associated with a higher risk of recurrent stroke/TIA. These were intraplaque hemorrhage,29 ulceration,25,29 echolucent plaques,10 hyperintense plaque,19 irregular plaque,30 and fibrous cap with a lipid-rich core.31 Three studies13,14,27 found intraplaque hemorrhage associated with a high rate of recurrent ischemic events: 4.9/100 person-years (95% CI, 1.6–8.1 person-years; Fig 3). For the remaining plaque features, the data were insufficient for a meta-analysis.

Incidence rate (per 100 person-years) of recurrent stroke in patients with SyNC, with intraplaque hemorrhage (IPH). ES indicates effect size.
Ten studies reported treatment strategies for patients with SyNC. Of those, 5 used medical treatment (antiplatelets, statins) alone,6,21,23,26,27 3 reported a combination of medical treatment and carotid revascularization,8,20,28 1 study reported both surgical and endovascular management,14 and 1 study reported only surgical outcomes.13 The low numbers in these arms were insufficient to perform a meta-analysis.
Risk of Progression to >50% Stenosis in ASyNC
Eight studies (n = 2223 participants) assessed stenosis progression from <50% to >50%. Overall, 448 of 2223 (20.2%) patients with ASyNC had stenosis progression. The pooled risk of progression was 11% (95% CI, 10%–12%; I2 = 0, P < .01) during a mean follow-up of 6.0 years (Fig 4).
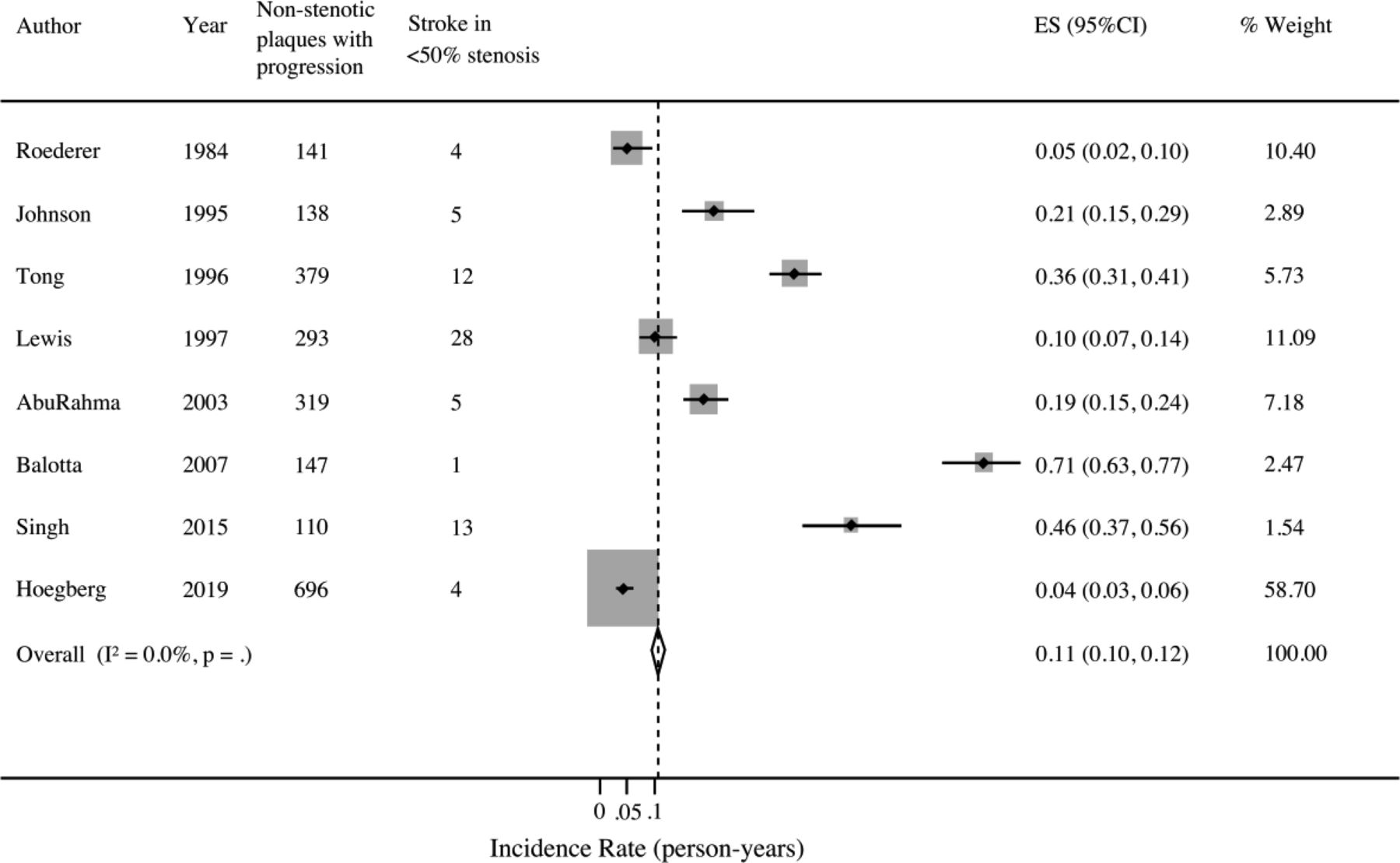
Risk of progression of <50% stenosis to >50% stenosis in ASyNC. ES indicates effect size.
Sensitivity Analyses
Detailed analyses as per study design and imaging technique for both ASyNC and SyNC are provided in the On-line Appendix (On-line Figs 8–11).
DISCUSSION
Carotid stenosis with >50% luminal narrowing accounts for 10%–20% of all strokes.32,33 The long-term risk of ipsilateral stroke in patients with >70% stenosis was 28.3% at 3 years in NASCET5 and 19% at 5 years in the ECST.4 These risks were significantly reduced after carotid revascularization. The long-term risk of ipsilateral stroke in carotid stenosis of <50% during 5 years was 18.7% in the NASCET and 8.2% in the ECST.4,5 Recently, multiple studies have shown an association between nonstenotic (<50%) carotid plaques and ischemic stroke,7,13,19 suggesting that certain carotid plaques might be an important source of stroke irrespective of the degree of stenosis. Our reported incidence of recurrent ipsilateral stroke/TIA in symptomatic, nonstenotic (<50%) carotid plaques, which substantially increases in the presence of high-risk plaque features, is comparable with the risk of recurrent strokes in stenotic (>50%) carotid plaques per NASCET and the ECST (around 9% and 4% per year, respectively).4,5 In contrast, the incidence of first-ever TIA or stroke in asymptomatic nonstenotic carotid plaques is lower compared with a 3%–4% annual incidence of stroke with severe (>70%) carotid stenosis per the Asymptomatic Carotid Atherosclerosis Study in the United States and the Asymptomatic Carotid Surgery Trial in Europe.34,35
In this meta-analysis, the relatively high rate of recurrent strokes in SyNC can be explained by the high-risk patients who already had at least 1 stroke with associated risk factors. In addition, because most studies included strokes of different etiologies, nonstenotic plaques might be an incidental finding in many cases, and these recurrent strokes are due to other unidentified etiologies (eg, cardioembolic). Also, the stroke etiology work-up was not uniform, and none of the studies that reported stroke recurrence outlined the investigations performed to rule out a cardioembolic source. On the other hand, with the increasing use of CTA to investigate stroke etiology, symptomatic nonstenotic carotid lesions are now recognized more frequently, and the risk of recurrent events might indeed be high. However, given the small sample size, selection bias and biases in reporting results cannot be ruled out.
Eight of the 14 studies with SyNC reported stroke etiology, and in all of these, ESUS was the predominant etiology. As of today, data supporting nonstenotic carotid lesions as a possible etiology of stroke are not robust, and most of these patients are currently classified as having ESUS if other sources of stroke are ruled out.9,28 The incidence of recurrent strokes was 2.6/100 person-years in patients with nonstenotic carotid lesions and otherwise unknown etiology, which may suggest that SyNC is potentially the etiology of these cryptogenic strokes.
Apart from the measurement of the degree of stenosis, growing literature uses high-definition vessel wall imaging of high-risk plaque features to identify patients at increased risk of recurrent stroke, despite low-grade stenosis.11,36 In this metanalysis, studies in both populations (especially SyNC) reported specific plaque features that predict a high recurrence rate, the most common being intraplaque hemorrhage. We found that the incidence rate of recurrent strokes is the same as that in symptomatic severe carotid stenosis, which should raise awareness of this high-risk subgroup. However, these studies are relatively small (total n = 31) and few in number (n = 3). Also, our search strategy did not include specific terms like “intraplaque hemorrhage” and so forth because this was not our primary outcome, which may have led to under-reporting of these specific features. Even though the representation of the subgroup of patients with SyNC and high-risk plaque features in the currently existing literature is limited, these findings are thought-provoking and support the need for larger studies and further validation.
Another important aspect is the treatment of patients with symptomatic nonstenotic carotid plaques. Current guidelines rely on the measurement of the degree of stenosis to recommend carotid revascularization.3 However, there is increasing evidence to suggest that unstable, inflamed, carotid plaques could rupture, causing stroke irrespective of the degree of stenosis.37 Furthermore, studies have also demonstrated that certain subgroups of patients with nonstenotic carotid stenosis tend to have recurrent strokes despite the best medical management.28,37,38 These observations suggest a limited efficacy of medical therapy in a subgroup of patients with SyNC with high-risk plaque features. Recent studies using high-resolution imaging to detect high-risk patients with SyNC have shown a benefit of carotid revascularization with almost no recurrence on follow-up.8,13 These studies indicate that the degree of stenosis alone may not be sufficient to determine treatment strategies, and plaque features and vulnerability may become important considerations in the treatment decision-making.
Limitations
This meta-analysis has several limitations: First, many of the included studies for assessing the risk of first-ever stroke/TIA in nonstenotic carotid plaques were relatively old: Ten of 25 were published before 2000, and the oldest study was published in 1984. Also, many of these studies traditionally classified the degree of stenosis as <30%, 30%–70%, and >70% before the NASCET definition. Because this classification system incorporates 50%–70% stenosis along with nonstenotic plaques, we excluded them to avoid the overestimation of results. Furthermore, there is heterogeneity both in the imaging technique and the underlying classification system used for characterizing carotid stenosis in the included studies. We addressed this issue using sensitivity analyses, stratifying by imaging technique. Last, only a few publications reported stroke etiology, and overall, the number of patients with ESUS and nonstenotic carotid plaques was provided infrequently. Even though our results are overall comparable with numbers reported in prior studies7 of patients with ESUS and nonstenotic carotid plaques, overestimation of recurrent events might have occurred because other etiologies of stroke (eg, cardioembolic) could not be excluded.
CONCLUSIONS
The risk of first-ever stroke/TIA with ASyNC in our meta-analysis was low, but once the patient was symptomatic, the risk of recurrent stroke/TIA in SyNC increased substantially, particularly when high-risk features such as intraplaque hemorrhage were present. Given the emerging evidence for an association between nonstenotic carotid plaques and stroke, one must consider it an etiology and investigate further to assess high-risk features. Presently, there is insufficient evidence to support a treatment strategy for this high-risk subgroup of patients with SyNC. Further research is needed to better investigate the natural history, progression from <50% to >50% stenosis, and potential treatment options such as more aggressive medical management or carotid revascularization of patients with nonstenotic carotid plaques.
Footnotes
N. Singh and M. Marko contributed equally to this publication.
Disclosures: Mayank Goyal—UNRELATED: Consultancy: Medtronic, Stryker, Mentice, MicroVention; Grants/Grants Pending: Medtronic, Stryker, Cerenovus*; Patents (Planned, Pending or Issued): GE Healthcare, Comments: systems of acute stroke diagnosis; Royalties: GE Healthcare. *Money paid to the institution.
References
- Received March 7, 2020.
- Accepted after revision April 29, 2020.
- © 2020 by American Journal of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
{kind=link}