
Abstract
SUMMARY: The frontal process of the maxilla occasionally shows a localized FD-like appearance. The purpose of this study was to determine its prevalence and findings on CT. A retrospective study of 1000 consecutive paranasal sinus CT scans was preformed on outpatients without a history of trauma or previous surgery in our hospital during 6 months. CT images were interpreted independently by 2 experienced head and neck radiologists on a PACS system in a bone window setting. Of the 1000 patients (546 males; 454 females), 51 (5.1%,41 males and 10 females) had an FD-like appearance in the frontal process of the maxilla. There was a statistically significant difference between sexes (P < .001). Twenty-nine (56.9%) entities arose from the right frontal process and 22 (43.1%) from the left frontal process. These entities, with well-defined margins, were located at the base of the frontal process of the maxilla, appearing as an ovoid or triangular configuration on axial-plane CT and as a spindle or elliptic shape on the coronal plane. The mean maximal diameter was 9.8 mm (range, 3.6–16.1 mm). These entities exhibited a pagetoid appearance (type I) in 37 (72.5%), a ground-glass appearance (type II) in 8 (15.7%), and a cyst-like appearance (type III) in 6 (11.8%) patients on CT. The FD-like appearance of the frontal process of the maxilla is not rare and can be readily detected by CT.
Abbreviations
- FD
- fibrous dysplasia
During the past 10 years, we have incidentally encountered a few people with an FD-like appearance of the frontal process of the maxilla by paranasal sinus CT in our daily practice. These individuals usually presented to the ear, nose, and throat clinic with rhinosinusitis symptoms and underwent paranasal sinus CT scans. On the basis of outpatient medical records, they had no facial deformities on physical examination. To the best of our knowledge, no relevant studies on the subject have been reported in the literature to date.1–6 Knowledge of the osseous appearance in this region could help radiologists and clinicians increase their awareness of the variant or asymptomatic FD, avoiding confusion with tumor or infection. For us, there has been some recent interest in the appearance of the frontal process of the maxilla. This prompted our study to determine the prevalence and features of it on paranasal sinus CT scans of outpatients in North China.
Materials and Methods
Patients
This study was approved by the institutional review board. A retrospective review of paranasal sinus CT scans of 1000 consecutive outpatients who were consecutively selected by a PACS system in our hospital between August 1, 2008, and January 31, 2009, was performed. All these patients were referred for CT due to clinical symptoms, presumably rhinosinusitis. Their clinical medical records were reviewed, and they had no history of trauma or prior surgery.
CT Technique
CT images were acquired in both the axial and coronal planes by using a Brilliance 64-section CT scanner (Philips Healthcare, Best, the Netherlands). The imaging parameters were as follows: voltage, 120 kV; current, 200 mA; matrix, 512 × 512; and section thickness, 2 mm. These images were reconstructed by using a bone algorithm. Reformations were performed from the superior wall of the frontal sinus to the inferior wall of the maxillary sinus on the axial plane and from the anterior wall of the frontal sinus to the posterior wall of the sphenoid sinus on the coronal plane.
Data Analysis
All CT images were reviewed on a PACS system in a bone window setting (window width of 4000 HU at a window level of 700 HU) by the same 2 experienced head and neck radiologists, and the findings were reached by consensus. The paranasal sinuses and craniofacial bones on CT images were carefully evaluated. If the frontal process showed the FD-like appearance, we analyzed the following imaging features: size, margin, shape, and attenuation.
On the basis of the classification of FD proposed by Fries,7 the CT findings were then classified into 3 types: Type I (pagetoid pattern) appears as a bony expansion and primarily consists of a mixture of ground glass and sclerotic attenuation; type II (ground-glass pattern) is characterized by bony expansion with homogeneous ground-glass attenuation; and type III (cyst-like pattern) has a spheric or oval shape and appears as a well-defined lucent area with a ground-glass or a sclerotic margin.
Statistical Analysis
We analyzed the data by using the Statistical Package for the Social Sciences, Version 11.0 software (SPSS, Chicago, Illinois). The χ2 test and Monte Carlo exact test were used to calculate the measure of association. A P value < .05 indicated a statistically significant difference.
Results
The study population consisted of 546 (54.6%) males and 454 (45.4%) females with a median age of 41.2 years (range, 8–89 years). Among 1000 patients, 736 (73.6%) had paranasal sinusitis.
Of the 1000 patients, 51 (5.1%) were identified with an FD-like appearance in the frontal process of the maxilla, including 41 men and 10 women, with a median age of 47.3 years (range, 22–83 years). There was a statistically significant difference between sexes (P < .001). The primary clinical manifestations were as follows: nasal obstruction in 43 (84.3%) patients, rhinorrhea in 38 (74.5%), headache in 24 (47.1%), and dysosmia in 8 (15.6%). Of the 51 entities, 29 (56.9%) arose from the right frontal process and 22 (43.1%) from the left frontal process. Of the 10 women, 7 (70%) showed an FD-like appearance in the left frontal process, and 3 (30%) in the right frontal process. Of the 41 men, 26 (63.4%) showed an FD-like appearance in the right frontal process, and 15 (36.6%) in the left frontal process. There was no statistically significant difference between right and left frontal processes of the maxilla in these 51 patients (P = .483).
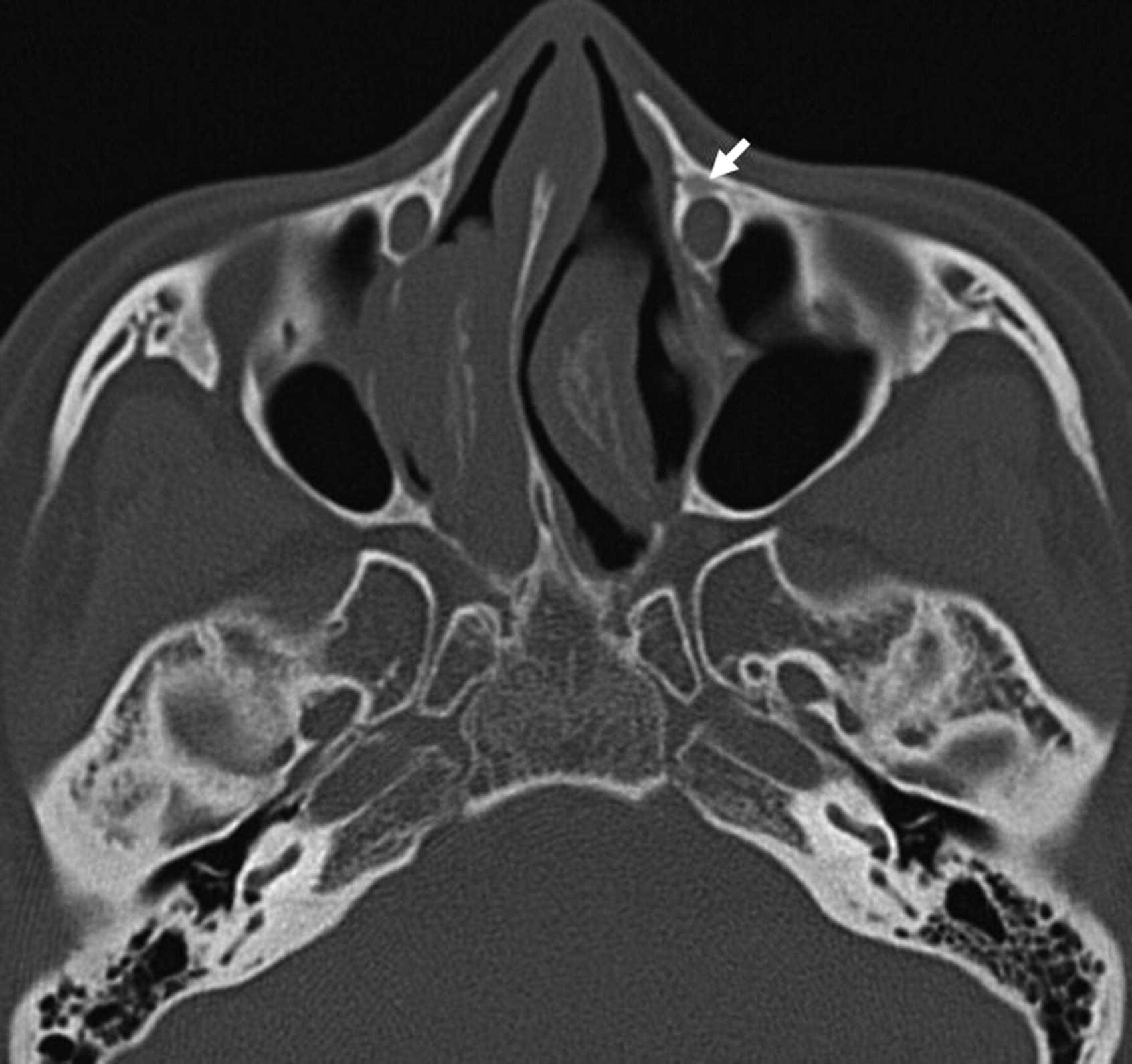
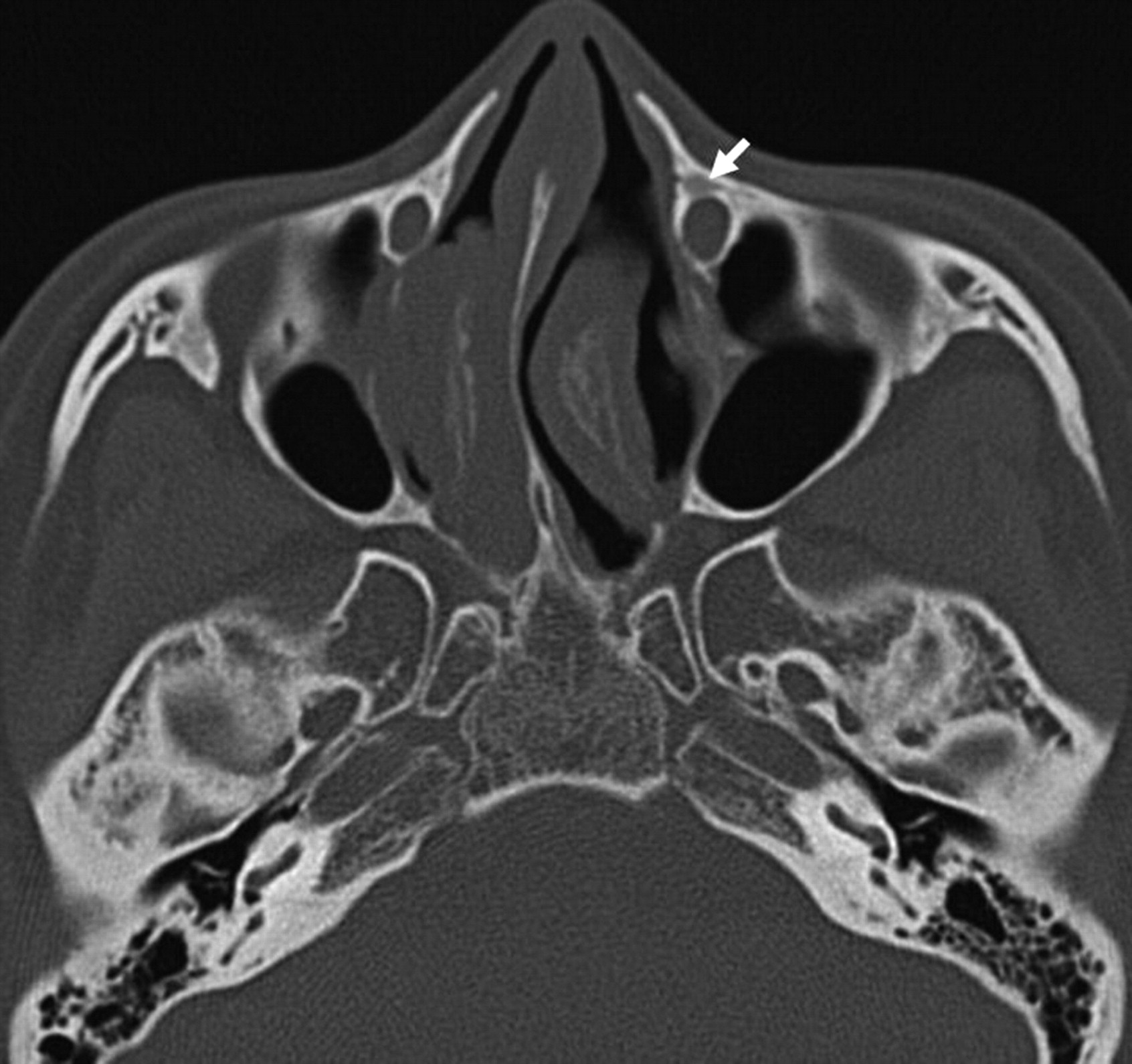
These entities were located at the base of the frontal process of the maxilla, adjoining the lacrimal sac. All entities showed relatively well-defined margins and appeared as an ovoid or triangular configuration on axial CT planes and as a spindle or elliptic shape on coronal planes. Their mean maximal diameter was 9.8 mm (range, 3.6–16.1 mm). These entities showed type I in 37 (72.5%) (Fig 1), type II in 8 (15.7%) (Fig 2), and type III in 6 (11.8%) patients (Fig 3) on CT. There were no statistically significant differences as to sex (P = .146) or side (P = .389) among the 3 patterns. In addition, these entities caused localized thinning of the bony cortex, without crossing the bony suture. The contour of the affected region of the frontal process usually showed slight expansion; however, these entities did not significantly compress and obstruct the surrounding structures.

Axial CT image shows the typical pagetoid appearance (type I) (arrow) in the left frontal process of the maxilla.
Axial CT image shows a ground-glass appearance (type II) (arrow) in the left frontal process of maxilla.

Axial CT image shows the cyst-like appearance (type III) (arrow) in the right frontal process of the maxilla.
No similar manifestation was detected in other craniofacial bones on CT images. Of the 51 patients, 35 (68.6%) had paranasal sinusitis.
Discussion
The frontal process of the maxilla has an irregular shape, attached to the frontal, nasal, and lacrimal bones. It forms the anterior lacrimal crest of the lacrimal fossa and also contributes to the osseous part of the nasolacrimal duct. It occasionally produces an FD-like appearance, which can be easily demonstrated on CT. The etiology of this finding is unknown at present; however, we speculate that it may be related to the development of the frontal process, the apposition of the frontal process, and lacrimal bone trapping some of these embryonic cells, eventually leading to unchecked fibro-osseous proliferation.1,4 This speculation could explain the FD-like appearance of the frontal process that develops near the bony suture and also arises from rests of fibrotic or cartilage stem cells present in bone rather than the bony suture, which may contribute to these occurrences that are far from the bony suture. Because most entities were incidentally found on paranasal sinus CT in patients who had no clinical manifestations related to this finding and the CT findings were very similar to those of FD as well, we postulate that the appearance of the frontal process may be either a nonsymptomatic FD or a benign osseous variant.
This FD is usually seen during childhood and adolescence; in most cases, it arises before 20 years of age, and it is more common in females than in males. In our case series, men (41/546) were more frequently affected than women (10/454), and the median age was 47.3 years. Craniofacial FD is usually unilateral, and the maxilla is the most commonly involved site in this region.8–10 The frontal process of the maxilla was unilaterally affected in our series. This may also provide further evidence for our above-mentioned hypothesis.
In this series, this entity was located at the base of the frontal process of the maxilla, adjoining but not compressing the lacrimal fossa. The CT features of these entities were characteristic. Similar to those on FD, their radiographic findings ranged from lucent zones to diffuse areas of sclerosis. The radiographic appearances may depend on the phase of development and amount of fibrous tissue and woven bone within the entity.8–10 On the basis of the features of the craniofacial bones on radiographs, Fries7 classified FD into 3 patterns: pagetoid, sclerotic, and cyst-like. In the present study, we adopted this classification scheme to analyze our cases. Poorly mineralized bone predominates early, producing an osteolytic-appearing entity (cyst-like pattern) with peripherally lamellar onion peel–like ground-glass or sclerosis, often referred to as an “egg shell lesion” on CT. As the woven bone mineralizes, the entity exhibits the classic expanded “ground-glass” appearance (ground-glass pattern) on CT. In later phases, due to the increase of attenuated osseous tissue, the entity may take on a more attenuated heterogeneous appearance (pagetoid pattern).2,11 The pagetoid (72.5%) pattern was the most common in this series, followed by ground-glass (15.7%) and cyst-like (11.8%) patterns, which may indicate that this entity often is detected in later phases. The affected frontal process of the maxilla may be slightly expanded, along with a typically intact thin cortex. According to our comparison analysis with different windows on the PACS system, this appearance of the frontal process of the maxilla is more clearly demonstrated by using wide windows such as width/level, 4000/700 HU on CT images.
The FD-like prevalence was 5.1% in our study, thus it is important to recognize this as a common finding in healthy populations. In the past, due to low resolution of the paranasal sinus or nasal bone radiographs, most entities were not demonstrated by this conventional imaging technique. However, with the development of CT and wide clinical application of paranasal sinus CT in recent years, we have observed more and more cases; the true incidence may be even higher in the future due to further recognition.
Treatment for this entity is not necessary unless there is significant deformity or loss of function.1,6,12 Accurate identification of the FD-like appearance of the frontal process of the maxilla on CT may be a great help in the differential diagnosis for diseases in this region.
A limitation of our study was that the analysis of imaging data was performed retrospectively and these entities were not proved by histopathology. In addition, the dynamic changes of these entities with time were not studied. Thus, further study is required to comprehensively elucidate the entity, including its etiology, histopathology, clinical significance, and so forth.
Conclusions
The detection of FD-like foci in the frontal process of the maxilla is not rare and can be clearly shown by CT. Similar to FD, this entity appears with typical features on CT. Although the clinical significance of this entity may be minimal, knowledge of its CT appearance may help in the differential diagnosis for diseases in this region.
References
- Received June 6, 2010.
- Accepted after revision August 4, 2010.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.