
Abstract
BACKGROUND AND PURPOSE: Our aim was to describe the immediate or early complications and technical failures occurring during balloon kyphoplasty (BKP) procedures and attributable to balloon inflation.
MATERIALS AND METHODS: We performed a retrospective review of all consecutive kyphoplasty procedures performed in our institution from May 2005 to October 2006. Fifty-one patients were treated by BKP at 75 spinal levels, and 137 vertebroplasties were performed as well.
RESULTS: Several recurrent complications or procedural failures were observed during BKP: cortical or endplate fracture by balloon expansion (4 vertebrae), partial vertebral re-collapse after deflation (4 vertebrae), balloon rupture during inflation (5 vertebrae), and transient hyperalgia after the procedure (11 patients, 27.5%).
CONCLUSIONS: Several symptomatic or asymptomatic complications and technical failures can occur during BKP. Some modifications of the usual kyphoplasty technique may decrease the frequency of these complications.
Percutaneous balloon kyphoplasty (BKP)1 is an interventional radiologic technique that has been used in the treatment of vertebral compression fractures due to various causes such as osteoporosis, metastases, or trauma.2,3 In BKP, inflated balloon tamps are used to restore the height of the vertebral body and correct kyphosis before injecting bone cement for stabilization of the fracture. The cavity created in the vertebral body is filled with cement after removal of the deflated balloons. Although fewer cement leakages are described with this technique than with vertebroplasty,2–4 some specific intraoperative complications can occur, especially during balloon inflation. The purpose of this article was to review the possible technical failures and complications in BKP that are related to balloon expansion inside the vertebral body and to discuss possible modifications of the usual kyphoplasty technique that can be applied to decrease the incidence of these events.
Materials and Methods
All consecutive patients who were referred to our radiology department for treatment of vertebral compression fractures between May 2005 and October 2006 were included. In this period, 51 patients (mean age, 69 years; range, 51–85 years; 16 men and 35 women) were treated by percutaneous kyphoplasty at 75 spinal levels. In addition, these patients underwent percutaneous vertebroplasty at 137 spinal levels. All patients underwent preprocedural conventional vertebral radiography, CT, and MR imaging of the spine before treatment, and radiography and CT after treatment. The etiology of the vertebral compression fractures was examined through histologic analysis of biopsies made before or during the intervention. The etiology was benign in 27 patients: osteoporosis (25 patients) and trauma (2 patients). A malignant etiology was found in 24 patients: multiple myeloma (17 patients), lymphoma (1 patient), and metastasis (6 patients). For all patients, the clinical indication for percutaneous treatment was spinal pain due to vertebral fracture. Vertebroplasty alone was performed if no fracture reduction was necessary. The indication for kyphoplasty was significant (ie, ≥20%) height loss of the vertebral body. Height loss was assessed before the treatment by analysis of the CT scans. Normal theoretic height of fractured vertebrae was assessed by calculating the mean height of the normal vertebrae below and above the fractured vertebra.
The mean time period between fracture and intervention was 69 ± 51 days (range, 5–180 days). An average of 1.5 vertebrae per patient was treated by percutaneous kyphoplasty, and an average of 2.7 vertebrae, by percutaneous vertebroplasty. The average number of vertebral levels treated for each session was 3.3 levels (average number of treatment sessions, 1.25 per patient). The treated vertebral levels were T4 (1 vertebra, 1.3% of treated vertebrae), T5 (2, 2.6%), T6 (2, 2.6%), T7 (2, 2.6%), T8 (6, 8%), T9 (4, 5.3%), T10 (1, 1.3%), T11 (4, 5.3%), T12 (17, 22.6%), L1 (12, 16%), L2 (10, 13.3%), L3 (5, 6.6%), L4 (5, 6.6%), and L5 (4, 5.3%).
Kyphoplasty Procedure
All BKPs were performed by an experienced interventional neuroradiologist.
Procedures were performed in an angiography room with biplane control (C-arm angiographic unit, AdvantX; GE Healthcare, Milwaukee, Wisconsin), associated with a mobile angiographic unit (Siremobile 2000; Siemens, Erlangen, Germany) under aseptic conditions. The treatment was applied with the patient under general anesthesia. BKP was performed according to the usual percutaneous kyphoplasty technique.1 Thirteen-gauge needles were used to puncture the vertebra and to introduce the 7-gauge KyphX Osteo-Introducer (Kyphon, Sunnyvale, California) inside the posterior part of the vertebral body. Balloons were 15 mm long at superior thoracic levels (above T8) (K09A, Kyphon) and 20 mm long from T8 to L5 (K09A, Kyphon). Balloons were positioned inside the vertebral body via a bilateral transpedicular (thoracic level) or lateropedicular (lumbar level) approach by using an introducer system. The 2 balloons were then inflated with contrast medium under barometric control. The maximum balloon inflation pressure was 400 psi. The maximum inflated volume was 4 mL for a 15-mm-long peanut-shaped balloon and 6 mL for a 20-mm-long peanut-shaped balloon. After deflation and removal of the balloons, polymethylmethacrylate (PMMA) cement was injected at low pressure into the cavity created, to stabilize the vertebral fracture. Intravertebral injection was performed under lateral and anteroposterior fluoroscopy. All kyphoplasty procedures were performed with PMMA (KyphX HV-R, Kyphon).
In case of re-collapse of the vertebra after balloon deflation, the BKP technique was modified to avoid loss of fracture reduction after balloon deflation. The BKP technique was begun as usual, and the balloons were inflated to reduce the vertebral fracture. When a loss of fracture reduction was observed after deflating the balloons, as opposed to the conventional technique earlier described in “Materials and Methods,” the 2 balloons were re-inflated to the same volume and pressure. Only 1 balloon was then deflated and removed instead of the 2 balloons. The balloon that was not deflated was designed to maintain the maximum fracture reduction initially obtained with the 2 balloons. Cement was injected at low pressure into the hemivertebra that did not contain the inflated balloon. After polymerization of the cement in this hemivertebra, the second balloon was deflated and removed and cement was injected into the ipsilateral hemivertebra. We called this technique “maximum fracture reduction.”
The efficacy of the treatment was assessed by scoring the level of pain before and after treatment on a visual analog pain scale ranging from 0 to 10 (no distress to unbearable distress).
Statistics
Complications and technical failures evaluated included the following: cortical or endplate fracture by balloon expansion, transient hyperalgesia, balloon rupture during inflation, and partial vertebral re-collapse after balloon deflation. The incidence of these complications and technical failures is reported as numbers and/or percentages.
Results
Two days after BKP, 92% of patients had a reduction of at least 3 levels on the visual analog pain scale. The incidence of cement leakage in kyphoplasty (assessed by control CT after the treatment) was 33% for the total number of treated vertebrae. We did not observe any complication due to cement leakage. Among vertebrae treated by BKP, several complications and technical failures due to balloon expansion were observed in 13 vertebrae (17.3%) (Table).
Vertebrae data and complication rates
First, we observed cortical or endplate fracture by balloon expansion in 4 vertebrae of 4 patients (mean age, 72 years; range, 62–78 years): 3 with osteoporosis and 1 with a myeloma (Fig 1). In 1 female patient (78 years of age with a myeloma), endplate fracture by balloon expansion led to a procedural fracture of an adjacent vertebral body (Fig 2). Second, we found vertebral re-collapse after deflation in 4 vertebrae of 4 patients (2 men and 2 women; mean age, 67 years; range, 50–82 years; mean re-collapse angle, 5°; Fig 3). Re-collapse was not related to a low clinical success; 100% of patients with re-collapse showed improvement of pain after treatment. The technique of maximum fracture reduction, as described in “Materials and Methods,” was used successfully in 2 of the 4 patients with vertebral fracture re-collapse after balloon deflation. Loss of local kyphosis reduction after balloon deflation was 4° and 9° for these 2 patients. The maximum fracture reduction technique restored the angle initially obtained. An analgesic effect was observed in both patients with no mortality or morbidity. Third, we observed balloon rupture during inflation in 5 vertebrae of 5 patients (2 men and 3 women; mean age, 62 years; range, 51–80 years): 2 with osteoporosis, 1 with trauma, 1 with lymphoma, and 1 with multiple myelomas (Fig 4).

Thoracic balloon kyphoplasty (BKP) for vertebral fracture due to multiple myelomas. Note anterolateral cement leakage due to a focal cortical fracture caused by balloon inflation (arrows).

A, Patient with multiple vertebral fractures due to multiple myelomas. Lateral view of T4, T5, and T6 before treatment. B and C, Superior endplate fracture of T5 during balloon inflation responsible for inferior endplate fracture of T4 (arrow) during the kyphoplasty procedure at T5, lateral (B) and anteroposterior views (C). D, Final lateral view after cement injection. T4 and T6 vertebroplasty was performed at the same time.

A, Maximal fracture reduction technique for a patient with L1 vertebral fracture due to osteoporosis. A−D, and I: Lateral view. E−G, and H, Frontal view. B, Initial balloon inflation leads to partial kyphosis correction (local kyphosis angle = 9°). C, Fracture reduction loss after balloon deflation (local kyphosis angle = 18°). D, Re-inflation of the 2 balloons to restore maximum fracture reduction. E and F, Deflation of only 1 balloon (E) and cement injection in the same side (F). G and H, After polymethylmethacrylate polymerization, deflation of the second balloon (G) and cement injection on the same side (H). I, Final view showing maintenance of the initial fracture reduction (local kyphosis angle = 9°).
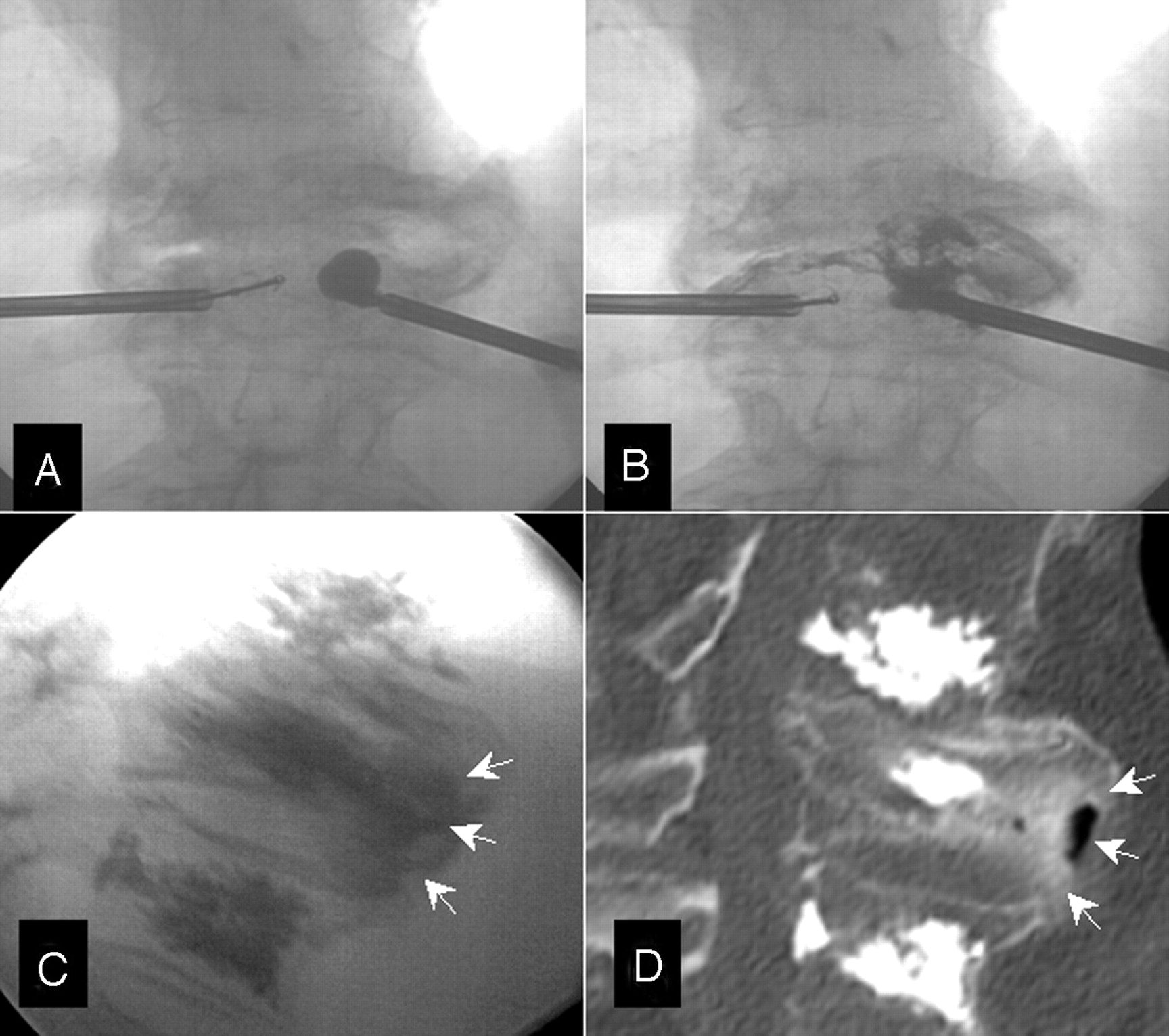
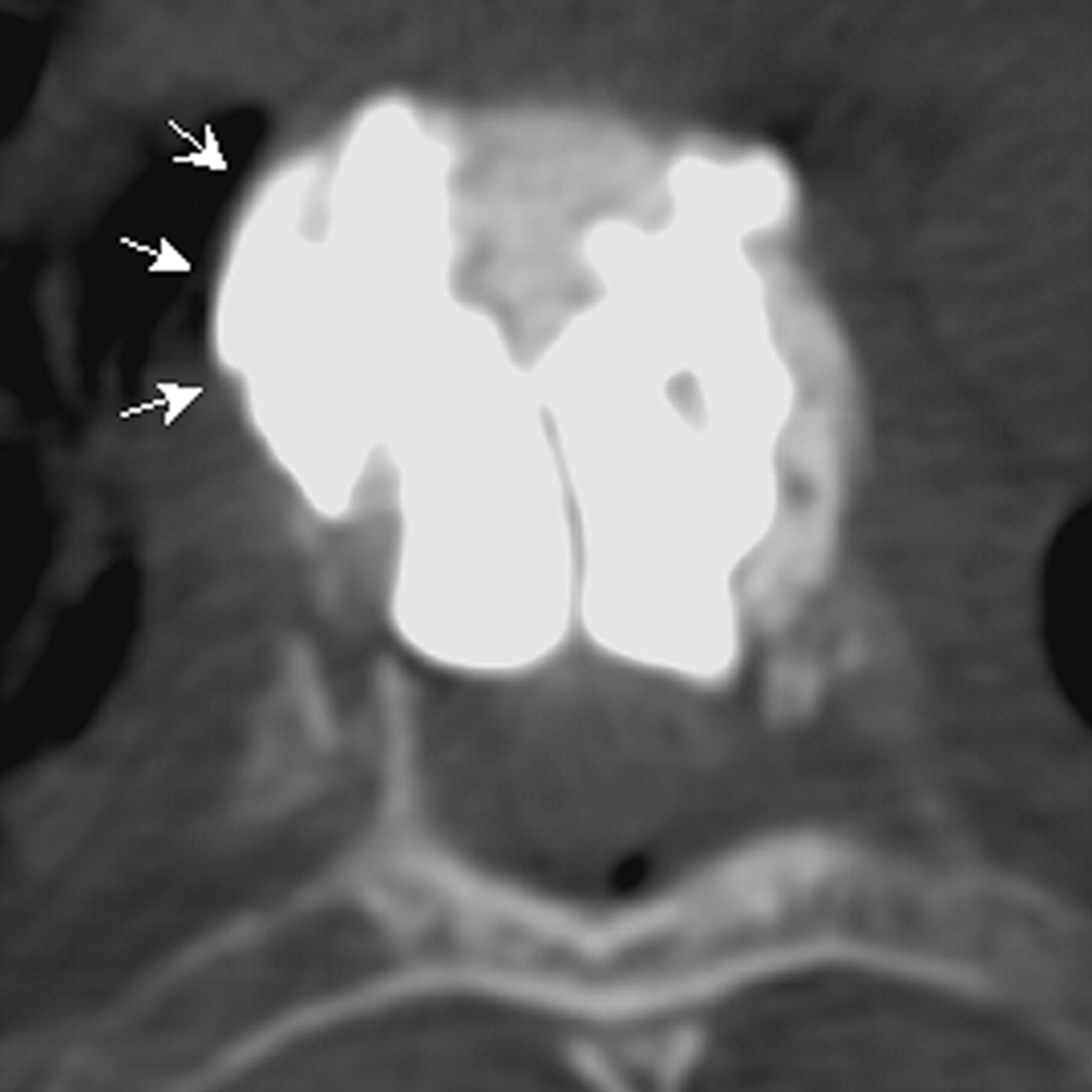
A, T12 BKP for vertebral fracture due to osteoporosis (frontal view). B and C, Balloon rupture responsible for anterior and lateral contrast leakage into the soft tissues (arrows). No arteriovenous leakage is seen. D, CT scan, final sagittal view showing anterior soft-tissue contrast leakage (arrows).
When balloon rupture occurred, we observed that contrast agent did not leak into veins or arteries in any of the patients in this series but predominantly remained inside the vertebral body with minor contrast agent leakage through the fracture line into the paravertebral space. Finally, we found that 11 patients (21.5%) had transient hyperalgesia after the procedure (3 men; 8 women; mean age, 72 years; range, 52–82 years): 4 with myelomas, 4 with osteoporosis, 1 with trauma, 2 with metastases. In 9 of these patients, kyphoplasty alone was performed (9 vertebrae). In this selective subgroup, 3 patients (33%) experienced transient hyperalgesia.
Discussion
We observed 4 types of complications and technical failures during BKP: cortical fracture during inflation, vertebral fracture re-collapse after balloon deflation, balloon rupture during inflation, and transient hyperalgesia.
Cortical Fracture during Inflation
If a cortical fracture occurs in the vertebral endplates, the inflated balloon can reach an adjacent vertebra when the intervertebral disk is thin and damage this adjacent vertebra. Four focal cortical fractures due to balloon expansion were observed in our study, and an adjacent vertebral fracture occurred procedurally due to expansion of the balloon through the vertebral endplate and the adjacent intervertebral disk. A predisposing factor for cortical fracture may be the presence of heterogeneous bone structure in a vertebra. This can lead to nonuniform balloon expansion during BKP and subsequent cortical fracture. Previously, we described a technique called “controlled segmental balloon kyphoplasty,” which allows controlled reduction of fractures in vertebrae with heterogeneous bone structure.5 In case of nonuniform expansion of balloons during inflation, we use that technique to decrease the risk of cortical fracture during inflation.
Vertebral Fracture Re-Collapse after Balloon Deflation
Some vertebral fractures can be spontaneously mobile, such as fractures with osteonecrosis.6 In our experience, these fractures are usually easily reduced by the inflatable balloon tamp because of their mobility. However, after deflation of the balloon, loss of fracture reduction can be observed7 with loss of kyphosis angle reduction. This forms a weakness of the kyphoplasty technique. Cement injection into the vertebral body is performed under low pressure and is unable to restore the loss of fracture reduction. The risk of cement leakage is increased when cement is injected at high pressure or when more cement is injected than the capacity of the cavity created in the vertebral body.
Four patients in the present study developed visible loss of fracture reduction after balloon deflation. Two patients were successfully treated by the maximum fracture reduction technique. Although based on a small population, this adaptation of the kyphoplasty technique avoided loss of fracture reduction during the procedure. In this limited series, no case of anterior cement leakage or complication was observed with this technique. Kissing balloons, which can occur during inflation when the balloons are located too medially, must be avoided. Excessive contact between cement and balloon, when the cement is injected into 1 side of the vertebra while maintaining an inflated balloon in the other side, can result in damage to the balloon because PMMA polymerizes via an exothermic reaction,8–10 releasing heat.
Balloon Rupture during Inflation
Although in itself not necessarily a technical failure or complication, balloon rupture is an unwanted event during the procedure because it may lead, for example, to contrast leakage or procedural delay. Contrast agent did not leak into veins or arteries in any of the patients with balloon rupture in our study but, predominantly, remained inside or close to the vertebral body. This can probably be explained by the fact that in the case of balloon rupture, the pressure in the vertebra rapidly decreases and contrast agent is not pushed into paravertebral vessels. The cavity created before balloon rupture also probably provides a reservoir for contrast agent.
No symptomatic complication due to balloon rupture (ie, gas embolism) was observed in this series. In the technique of BKP, balloons must be purged of any trapped air before insertion to prevent gas embolism in the event of balloon rupture. Balloon rupture appears to be facilitated by sharp solid bone fragments. In our experience, the risk of balloon rupture can be decreased by very slowly increasing balloon inflation pressures, which appears to allow the shape of the balloon to adapt to the solid and sharp bony environment. An alternative or additional way to limit balloon rupture consists of using a curette to break bone bridges and contusive bone fragments before inflating the balloon.
Transient Hyperalgesia
Transient hyperalgesia has been described after acrylic cement injection into the acetabulum11 or after vertebroplasty procedures in <3% of cases.12,13 Few publications have reported transient hyperalgesia after kyphoplasty.14 Transient hyperalgesia consists of accentuation or recurrence of pain early after the procedure. The polymerization of the cement that is injected during the BKP procedure leads to an exothermic reaction. The reported cause of pain was a local inflammatory response due to that exothermic reaction.14,15 Transient hyperalgesia has been treated by steroids and nonsteroidal anti-inflammatory drugs. An increased incidence of hyperalgesia (21.5%) was observed after kyphoplasty in our study group. In 9 patients, kyphoplasty alone was performed (9 vertebrae) without additional vertebroplasty. In this selective subgroup, 3 patients (33%) experienced transient hyperalgesia after the procedure. All patients were treated by nonsteroidal anti-inflammatory drugs (ketoprofen, 200 mg/day for 5 days), allowing resolution of pain after several days. The incidence of hyperalgesia in this subgroup of 9 kyphoplasty patients appears to be higher than that in vertebroplasty, according to the reported values for vertebroplasty in the literature.12,13
We hypothesize that hyperalgesia in kyphoplasty is related to balloon inflation that can cause paravertebral soft-tissue distraction. The trocars used for kyphoplasty (7 gauge) are also larger than those used for vertebroplasty (usually ≤10 gauge). These trocars can cause more soft-tissue or bone damage in the access route than in the vertebroplasty procedure. Moreover, the access used for the kyphoplasty procedures in our patients was a lateropedicular route, whereas the access for vertebroplasty was transpedicular. At thoracic levels, the lateropedicular route goes through the costovertebral joint. Possibly, this is associated with more frequent hyperalgesia. In our study group, among the 11 patients who had a transient hyperalgesia, 9 underwent kyphoplasty at a thoracic level and only 2 patients, at a lumbar level. We have the impression that that access results in more frequent transient hyperalgesia when it is at thoracic levels through the costovertebral joint.
Conclusions
Although several complications due to systemic disease, anesthesia, or access route have been described during kyphoplasty procedures, only a few complications or technical failures due to balloon inflation have been reported. The present series illustrates complications and technical failures in kyphoplasty that may be related to balloon inflation. Some modifications of the usual kyphoplasty technique may decrease the incidence of these complications.
References
- Received April 2, 2009.
- Accepted after revision June 16, 2009.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}