
Abstract
BACKGROUND AND PURPOSE: Analysis of the prevertebral soft tissue (PVST) is helpful in detecting osseous and ligamentous injuries of the cervical spine. Because the standard of care has shifted from radiographs to multidetector CT (MDCT), a re-examination of the PVST on MDCT images is needed to establish normal values for thickness appropriate for this imaging technique.
MATERIALS AND METHODS: Thickness of the PVST was measured in 192 patients undergoing screening cervical spine MDCT with multiplanar reconstructions as part of a trauma protocol. Patients included in the study were not intubated, had an immobilized cervical spine, had normal findings on cervical spine CT, and did not have a diagnosis of osseous or soft-tissue cervical injury. Exclusion criteria included patients with a congenital or acquired (nondegenerative) abnormality of the cervical spine or PVST.
RESULTS: The upper limits of normal for the thickness of the PVST were 8.5 mm at C1, 6 mm at C2, 7 mm at C3, 18 mm at C6, and 18 mm at C7. The upper limit of normal was not determined for C4 and C5 levels due to variable position of the esophagus and larynx. The smallest variability and calculated SDs were found at C2 and C3.
CONCLUSIONS: The thickness of the PVST is important in the detection of underlying injuries to the cervical spine. We propose the obtained values as the upper limits of normal for PVST thickness on MDCT images in the adult population.
The thickness of the prevertebral soft tissue (PVST) has long been considered a valuable radiographic measurement in evaluating possible injury to the cervical spine.1–6 Analysis of the PVST is helpful in detecting subtle osseous or ligamentous injuries that might go unrecognized. In our experience, the normal values based on radiographic studies are commonly used in multidetector CT (MDCT) images, despite the fact that differences in the acquisition of these images could account for significant differences in their normal values. With the widespread replacement of standard radiographic evaluation of the cervical spine by MDCT,4,7–10 it is necessary to establish normal values for the thickness of the PVST on MDCT images.
To our knowledge, an up-to-date evaluation of the PVST thickness on MDCT images has not been published. In the past, many authors have measured the PVST thickness on lateral cervical spine radiographs and obtained results that have a large overlap between normal and abnormal findings in patients.11 Others, such as Harris,1 found the contour of the PVST at the craniocervical junction to be a more reliable method of detecting underlying injury in this region. Hay et al proposed a ratio method in which they compared the thickness of the PVST with the width of the C5 vertebral body, therefore taking into consideration differences in radiographic technique and a patient's body habitus.11 All of these methods have their own limitations. Furthermore, the lack of abnormal PVST thickness does not exclude an underlying injury.3,12
The purpose of this study was to determine the normal thickness of the PVST on neutral position MDCT images in the adult population.
Materials and Methods
The patient population consisted of 192 trauma patients (119 men and 73 women) who presented to the hospital emergency department between January 2007 and April 2007 and underwent MDCT of the cervical spine with multiplanar reconstructions as part of a trauma protocol. The subjects selected for this study were 20 years of age and older (average age, 42 years; range, 20–98 years) and had no known prior cervical spine injury, congenital or acquired anomaly of the PVST such as retropharyngeal internal carotid artery, retropharyngeal lymphadenopathy, mass, abscess, or fluid collection. Degenerative disk disease was not an exclusion criterion.
Patients were evaluated for cervical spine injury and were included in the study if no congenital or acquired (nondegenerative) osseous abnormality was detected on initial CT and if the patient was discharged from the hospital without a diagnosis of a cervical spine or soft-tissue injury. Patients who had undergone endotracheal or nasogastric tube placement were not included in the study population because intubation has been shown to have an unpredictable but significant effect on PVST width.2 Further review of the patients’ clinical and radiologic histories was performed up to 1 year after the initial scan to exclude patients with cervical injuries that were diagnosed later.
Cervical spine imaging was performed without intravenous contrast by using a 16-section MDCT scanner, with the following standard protocol: 16 × 0.75 mm collimation with 1-mm-thick sections, 0.5-mm reconstruction overlap, and a pitch of 0.942. Axial images were reconstructed at 1 mm, and 3 contiguous sections were fused for review and storage on a PACS workstation. Reformations in both sagittal and coronal planes were obtained routinely from 1-mm axial reconstructions. Multiplanar reformations were reformatted to 3-mm thickness every 3 mm through the entire spine. A 16-cm FOV, 512 × 512 matrix, 140 kV, and 250 mAs were generally used; however, these factors were sometimes altered to accommodate a patient's body habitus. Patients were scanned in a “near-neutral” position with a cervical collar in place. Examinations selected for inclusion in this study were free from motion artifacts and allowed the measurement of the PVST thickness from C1 to C7 in the FOV. The images were analyzed by using a preset bone window with a window level setting of 450 HU and a window width setting of 1700 HU.
The measurements were performed in the midline on sagittal reformatted images extending from the midanterior vertebral body to the closest point in the air column from C3 to C7 in the preset bone window. At C1 and C2, the measurements were performed from the craniocaudal midpoint of the anterior arch of C1 and at the midpoint of the vertebral body of C2 (excluding the dens) to the closest point in the air column (Fig 1). The midline was determined by direct correlation with coronal reformatted images. Patients with scoliosis or positional rotation of the spine were analyzed after we obtained oblique sagittal reformatted images or by close correlation between the sagittal images and the coronal reformations to ensure the midline measurement. Measurements were recorded to the nearest half millimeter.

Midsagittal MDCT image of the cervical spine illustrating the method used to measure the thickness of the PVST.
Mean, SD, standard error of the mean, and range were calculated for each cervical spine level. Normal maximum values were defined as the value inclusive of 97.5% of the study population.
Results
At C1, the mean width of the PVST on MDCT was 4.4 mm, with an SD slightly >1.9 mm, and the upper limit of normal was 8.5 mm. At C2, the mean width of the PVST on MDCT was 3.7 mm, with an SD of 1.2 mm, and the upper limit of normal was 6 mm. At C3, the mean width of the PVST was 4.2 mm, with an SD slightly >1.3 mm, and the upper limit of normal was 7 mm. A large variability in the thickness of the PVST was found at C4 and C5 due to the inconsistent position of the esophagus and larynx; therefore, the upper limits of normal were not calculated for these levels. The mean width of the PVST at C6 was 13 mm, with an SD of 2.6 mm and an upper limit of normal of 18 mm. At C7, the mean width of the PVST was 11.6 mm with an SD of 3.2 mm and an upper normal limit of 18 mm (Table).
Results for mean, range, and upper limits of normal PVST thickness on MDCT*
SDs calculated at C2 and C3 were smaller than those for all other levels of the cervical spine. In general, larger SDs, ranges, and upper limits of normal were found for the thickness of the PVST at C4 and below.
Discussion
Analysis of the PVST as an indirect sign of underlying cervical spine injury is usually performed in the standard radiographic examination of the cervical spine. Assessment of the PVST thickness is the most commonly used method to evaluate for PVST edema and/or hematoma, which may accompany osseous or ligamentous injury. Several authors have calculated the average and normal upper limits for thickness of the PVST on lateral cervical spine radiographs13–19 as published in Keats’ and Sistrom's Atlas of Radiographic Measurement.11 With the advent of MDCT as the initial radiologic evaluation of the cervical spine in the setting of suggested trauma, normal PVST measurements specific to that technique are essential. Due to the various differences in the images obtained with standard radiographs compared with MDCT, the use of previously accepted normal values based on radiographs cannot be applied to MDCT images. In this study, we determined the normal thickness of the PVST in healthy adults on MDCT images. Familiarity with this normal aspect of the PVST on MDCT images will allow more accurate evaluation of the cervical spine in the acutely traumatized patient.
MDCT has fast become the initial radiologic examination in the setting of suggested cervical spine injury. In urban trauma centers, helical CT as the initial screening test in the evaluation for cervical spine fractures has been shown to lower both complications and institutional costs.10 Additionally, MDCT increases both the sensitivity and the rapidity of the initial cervical spine evaluation, whereas overall imaging costs remain similar to those of patients who are initially evaluated with radiographs.20 Multiple previous studies place the sensitivity of MDCT for fractures of the cervical spine at 99%–100%, significantly better than that of conventional radiography.4,8,20 Currently, in both Europe and the United States, MDCT has been recommended as part of a primary cervical spine screening protocol for trauma patients.4,8
The Normal Thickness of the PVST on MDCT
Causes of increased PVST thickness include infection, neoplasm, hemorrhage, and fluid accumulation.21 In the setting of trauma, severe potentially incapacitating injuries to the cervical spine can present with PVST thickening as the only radiographic sign.22 At the C1-C2 level, increased width of PVST could indicate atlanto-occipital subluxation, occipital condyle fractures, C1 fractures, odontoid fractures, rupture of the transverse atlantal ligament, or hangman fractures (Fig 2).1,3 At more inferior levels of the cervical spine, widening of the PVST has been associated with hyperflexion and hyperextension sprains, wedge and teardrop fractures, and unilateral and bilateral facet dislocation.3

A 24-year-old patient after a motor vehicle crash with closed head injury; no fracture was identified in the cervical spine or craniocervical junction. A, Midsagittal MDCT image of the cervical spine demonstrates abnormal PVST thickening at C1 and C2 (asterisks). B, Correlation with midsagittal short τ inversion recovery MR image obtained the next day confirms the presence of extensive PVST edema and/or hematoma in this region (arrowheads).
Edema and/or hematoma in the PVST is more commonly detected at the higher cervical levels (C2 and C3) than at the lower levels even in the presence of a lower cervical spine injury.3 This is thought to be secondary to a relatively greater laxity of the PVST above the esophagus that allows more thickening as well as a wider range of normal values in thickness of the lower cervical levels.3 This can translate into occult low cervical spine injuries only becoming radiographically manifest when they dissect cephalad and present as thickening of the C2-C3 PVST.3
Levels C2 and C3 were found to have the smallest range and SD between different patients. When comparing the data with normal values based on radiographs (mean of 3.9 mm at C2 and mean of 4.5 mm at C3),11 we found that the values obtained on MDCT images were statistically different (P = .041 for C2 and P = .0012 for C3). Similarities were found in the sense that these levels show the least variability between patients and, therefore, are conceptually the most reliable levels to determine abnormal thickness.11 The differences in the normal values obtained with the 2 techniques are mainly thought to be secondary to intrinsic magnification of radiographic techniques and differences in the way the measurements were obtained. Although the normal values found in Keats’ and Sistrom's Atlas of Radiographic Measurement were obtained extending from the inferior portion of the vertebral body to the air column, we performed the measurements on MDCT images at the midanterior vertebral body point to avoid confusion when reproducing these measurements in patients with degenerative disk disease and prominent osteophyte formation. Although the shape of the anterior vertebral body can vary to a certain degree between patients (ranging from concave to convex), in our experience, thickening of the PVST is greater at the levels of the midanterior vertebral body than it is at the regions anterior to osteophytes. For this reason, the measurements were performed at the midvertebral level and not at the endplates.
At C4 and the cervical levels below it, we found a wide range of normal, correlating with the great variation published in the literature based on radiographic evaluation.11 The thickness increased significantly compared with the upper cervical levels due to the presence of the esophagus and posterior wall of the airway. Furthermore, the esophagus and larynx were found to be in variable locations (C4 or C5) among the patient population, probably due to a different phase of swallowing. This is thought to account for the great variability and range at these levels, and for this reason, the upper limits of normal at C4 and C5 were not determined and conceptually should not be used to evaluate for abnormal thickness.
Normal Appearance of the PVST
Higher resolution MDCT scanners and current protocols allow a more detailed visualization of the PVST anatomy than was possible in the past. To evaluate the PVST appearance, we found the sagittal reformatted images very helpful, by using a preset soft-tissue window setting with a window width setting of 500 HU and a window level setting of −10 HU. Variations of the window level and width are sometimes necessary to improve tissue contrast.
The normal appearance of the PVST as seen on midsagittal reformatted images of the cervical spine is of 3 thin stripes anterior and parallel to the spinal column (Fig 3). The most anterior stripe, adjacent to the airway, represents the pharyngeal mucosa and the pharyngeal constrictor muscles, accounting for its soft-tissue attenuation. It is consistently thin and extends from the skull base down to approximately the level of C4-C5, where it joins the esophagus.
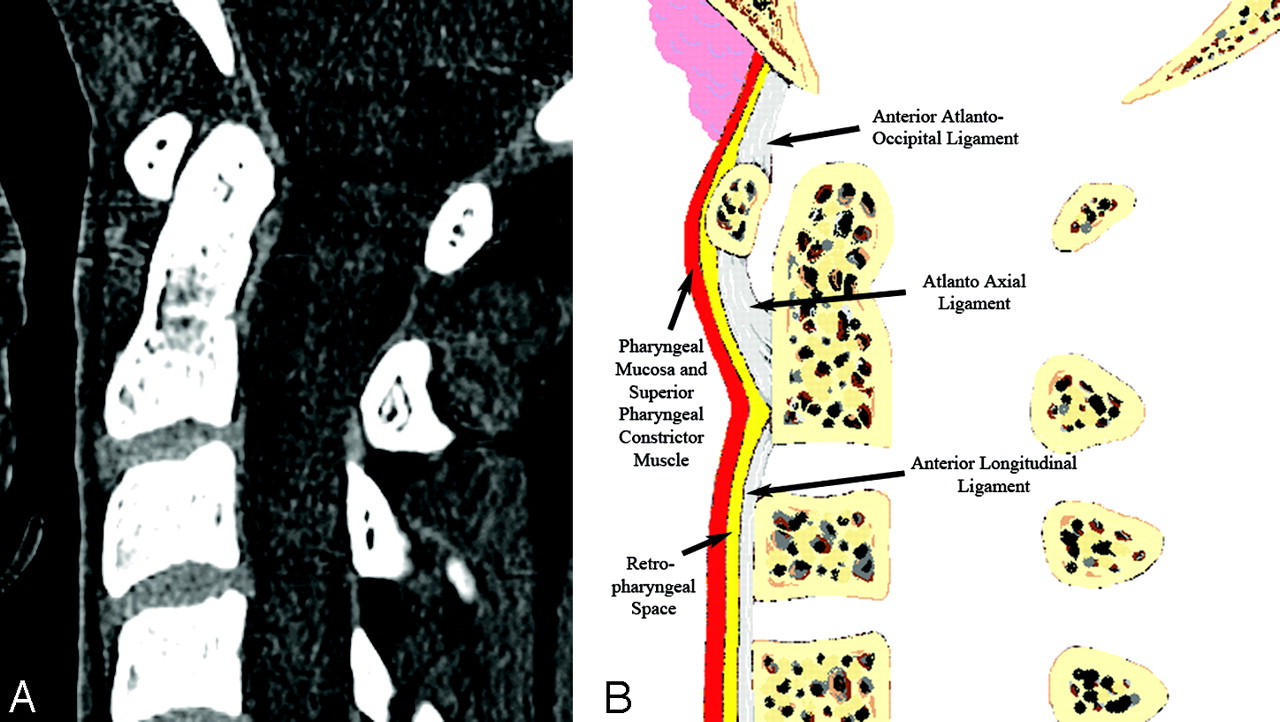
Normal appearance of the upper PVST on the midsagittal plane. A, MDCT image demonstrates 2 high-attenuation stripes separated by a central stripe of fat attenuation corresponding to the retropharyngeal/retroesophageal spaces. B, Diagram helps depict the normal anatomic planes of the PVST.
The second stripe has fat attenuation and represents the areolar and adipose connective tissues of the retropharyngeal and retroesophageal spaces.23 The retropharyngeal space is technically considered to extend from the base of the skull to the origin of the esophagus, where it continues inferiorly as the retroesophageal space. These 2 spaces are enclosed by the middle (visceral division) and deep (alar division) layers of the deep cervical fascia and contain a variable amount of lymph nodes superiorly.24 The fat stripe normally lies in close proximity to the anterior surface of the vertebral bodies and displacement can help detect and localize injuries to cervical spine.23 Variation in the thickness and conspicuity of this fat plane can be seen among individuals, but it is always present.25 This could be explained by differences in a patient's body habitus, because patient weight has been shown to relate proportionally to the thickness of the PVST on radiographs.26,27 In some patients, this fat plane can be identified more easily on parasagittal images due to relative thinning of this fat attenuation stripe in the midsagittal plane.
The third stripe is of soft-tissue attenuation and is made of ligamentous structures. Below C2, it is composed of the anterior longitudinal ligament, which inserts superiorly in the anterior and inferior portion of the vertebral body of C2. Extending from the C2 vertebral body rostrally, the third stripe is formed by the anterior atlantoaxial and anterior atlanto-occipital ligaments, which extend from the vertebral body of C2 to the anterior arch of the atlas and from the anterior arch of the atlas to the clivus, respectively.1
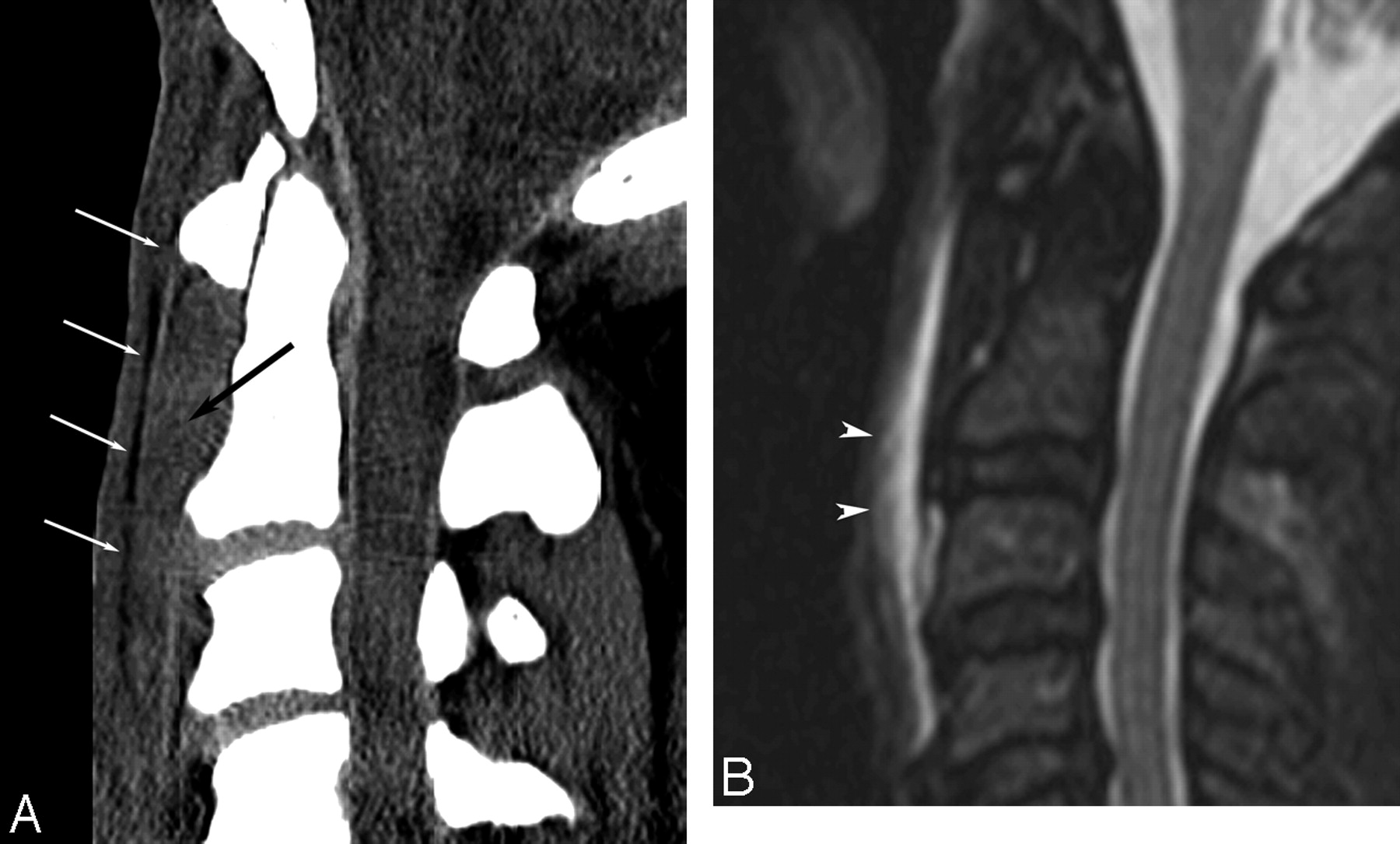
In our experience, the appearance of the PVST on sagittal reformatted images can aid greatly in the detection of PVST edema and/or hematoma. Different types of osseous or ligamentous injuries of the cervical spine can result in edema and/or hematoma of the PVST and alter the normal appearance on MDCT. This is commonly seen as anterior displacement of the fat plane by a thickened third stripe (Fig 4). The accumulation of blood in the prevertebral space contained by an intact prevertebral division of the deep cervical fascia, or ligamentous swelling, is thought to account for these findings. In some instances, there can be replacement or obliteration of the normal fat attenuation plane, thereby losing the normal striped appearance of the PVST. This is thought to be due to inflammation or hemorrhage in the retropharyngeal space. It is important not to confuse these findings with those of healthy patients who have a thin second stripe or fat plane in the presence of normal PVST thickness. Although increased thickness of the PVST can be helpful in these cases to suggest further imaging, we have seen this abnormal appearance in the setting of normal PVST thickness (by using MDCT normal upper limit values) later confirmed to be secondary to the presence of PVST edema and/or hematoma on MR imaging (Fig 5). Therefore, in our opinion, evaluation of the thickness and appearance of the PVST should be performed in patients with a history of cervical spine trauma to avoid missing occult injuries that manifest as abnormality in the PVST.

A 43- year-old patient after a motor vehicle crash with no osseous injury. A, Midsagittal MDCT image of the cervical spine demonstrates abnormal high attenuation (black arrow) anteriorly displacing the retropharyngeal fat plane (white arrows). B, Short τ inversion recovery MR image obtained the same day shows extensive PVST edema and/or hematoma in this region (arrowheads).

A 27-year-old patient after a motor vehicle crash with no osseous injury. A, Midsagittal MDCT image demonstrates normal PVST thickness by using normal values based on MDCT. B, Evaluation of the appearance of the PVST reveals subtle loss of the normal PVST fat plane above the inferior endplate of C3 (arrowhead). C, Correlation with short τ inversion recovery MR image obtained the same day confirms the presence of edema and/or hematoma of the PVST accounting for the MDCT image findings.
Ideally, the patient population would have included only healthy volunteers or patients undergoing MDCT of the cervical spine for an indication other than trauma. We did not find this to be practically feasible and included patients who sustained some form of trauma as an indication for evaluation of the cervical spine. Although this could be a limitation of the study, the presence of a cervical collar helped standardize the position of the cervical spine in a “near-neutral” position. We believe that the strict criteria for inclusion in the study patient population and the further review of the patients’ radiologic and clinical histories 1 year after trauma markedly decreased the possibility that a patient with a true cervical spine abnormality and PVST thickening was included in the study. Nonetheless, we cannot exclude the possibility that a patient included in our study presented to an outside institution later and was found to have an abnormality of the PVST.
Although it is known that changes in the position of the neck can translate into changes in the PVST thickness, the presence of a cervical collar ensured that patients were not in complete cervical flexion or extension. Penning3 studied the change in thickness of the PVST in patients under complete extension and flexion on radiographs, finding a maximal difference of <1 mm between the different positions compared with the neutral position. For this reason, the minor differences in the degree of flexion-extension allowed in the presence of a cervical collar likely did not cause significant changes in the PVST thickness.
Conclusions
We propose the obtained normal values as the upper limits of normal for PVST thickness on MDCT images in the adult population. As part of a comprehensive evaluation of the cervical spine in the setting of trauma, normal measurements of PVST thickness and familiarity with their normal appearance on MDCT sagittal reconstructed images could aid in the detection of subtle osseous or ligamentous injury.
Acknowledgments
The authors wish to acknowledge the contribution of Dr. Ed Nickoloff, Professor of Radiology (Physics), Columbia University and New York-Presbyterian Hospital.
Footnotes
Paper previously presented at: Annual Meeting of the Radiological Society of North America, November 29–December 4, 2007; Chicago, Ill.
References
- Received June 4, 2008.
- Accepted after revision July 28, 2008.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}