
Abstract
BACKGROUND AND PURPOSE: Systematic facial mutilations during mummification have never been described before. The purpose of this work was to study a wrapped mummified head using high-resolution CT scanning.
MATERIALS AND METHODS: An isolated mummified head from the Egyptian Middle Kingdom was scanned at 200 μm isotropic resolution. A prototype flat panel CT scanner was used to generate 800 nonoverlapping CT sections at 120 kV and 50 mA. This dataset was analyzed to discern various surgical alterations during mummification.
RESULTS: There were large defects in the cribriform plate and the posterior fossa. Systematic mutilations of the facial bones and mandible, involving the anterior and inferior walls of the maxillary sinuses, the floor of both orbits, and the zygomatic arches with contiguous segments of the zygomas, were demonstrated. The coronoid processes of both mandibles had been sharply excised and the articular tubercles of the temporomandibular joints fractured.
CONCLUSION: Defects in the ethmoid and the posterior skull base are consistent with previous descriptions of excerebration. Mutilations of the facial skeleton and jaw, which are unrelated to the process of excerebration, have never been described previously. It is noteworthy that the osteotomies selectively include the insertions of the muscles of mastication. These mutilations apparently were designed for mobilization of lower jaw. The “Opening of the Mouth” ceremony, described in the ancient texts, would be difficult to perform in the presence of rigor mortis; it is probable that the observed osteotomies were performed to facilitate this ceremony. Our research suggests that by the Middle Kingdom, Egyptian embalmers had developed highly sophisticated surgical techniques that have not been appreciated previously.
There are many open questions about various aspects of the mummification procedure as practiced by the ancient Egyptians. Recent technological advances in imaging and forensic science offer the possibility of gaining further insights into this process and providing definitive answers to some of these questions. A series of advanced radiologic examinations was conducted at the Massachusetts General Hospital to shed further light on the mummified head of Djehutynakht, an important Middle Kingdom artifact in the collection of the Museum of Fine Arts, Boston (MFA).
Methods and Materials
The Mummy
In 1915, the Harvard University-Boston Museum of Fine Arts expedition excavated the tomb of Djehutynakht, the local governor of a Middle Egyptian province who lived around 2000 BC.1 Although the tomb had been plundered in antiquity, the burial chamber still contained what are perhaps the finest Middle Kingdom coffins in existence. Made of cedar and painted both inside and out, they belonged to the tomb's owner and his wife, whose name was also Djehutynakht. As for the human remains, only a mummified head and a single finger have survived, though at the time of excavation there were remains including a torso scattered about the burial chamber and its entrance. The head, which is the subject of this study, is still invested in its molded linen wrappings, on which the eyebrows were drawn with black pigment (Fig 1).

Photograph of the mummified head of Djehutynakht.
Between 1984 and 1986, the MFA's collection of mummies was x-rayed and CT scanned at the Brigham and Women's Hospital in preparation for the exhibition “Mummies and Magic.”2 The head of Djehutynakht was among the remains examined. The radiographic results represented an important contribution to our understanding of the mummified head. It was appreciated that there was a defect in the ethmoid air cells and sphenoid sinus, indicating that the brain had been removed by that route. It was also noted that the maxillary sinuses had been partially destroyed. This was erroneously interpreted as being related to brain removal. The technology available at that time did not allow high enough spatial resolution and detail to deduce all of the alterations that were made during the mummification process and to appreciate the remarkable significance of these mutilations. Given the advancements in technology in the intervening 20 years, the following tests were undertaken at the Massachusetts General Hospital in 2005.
X-Ray Radiographs
Radiographs of the mummified head were taken to study the high-resolution projectional anatomy of the skull. Standard projectional x-ray views of the head were acquired to first look at the structure of the head. Morphometric measurements and the integrity (and lack of integrity) of various skull bones were established.
Multidetector CT
Detailed tomographic examination was undertaken to investigate the internal structure of the bones and to look inside the cranial vault by using a multidetector CT (MDCT, Sensation-64; Siemens Medical Solutions, Erlangen, Germany). These images were studied to determine whether and how the excerebration was done, the process of mummification, the state of dentition, and any bone pathology. The MDCT imaging was also used to reveal any trauma to the bones and to date them. Any bone trauma during life will show signs of healing, whereas trauma during the embalming procedure should have sharply defined borders without any signs of healing. Trauma to the skull, inflicted by grave robbers, would probably show up as depressed fractures. This test was also configured to reveal information about the teeth, general dental hygiene, wear pattern, nutritional status, and general aging.
MR Imaging
Although x-ray based CT is the study of choice for the evaluation of bony anatomy, the soft-tissue details are better assessed using MR imaging. The MR imaging was attempting to focus on the tissue structure of the mummy's head. It was hoped that the relative size of the muscles would shed light on the diet of that era. In addition, any piercings (eg, in the nose or ear lobe) may tell us about the customs and ornamentations prevalent in the Middle Kingdom.
Multiple different types of image sequences were attempted to assess the remains of the facial muscles after the mummification process and the intervening 4,000 years. However, despite using the shortest available TE and TR times, no signal intensity was detected by using the most sensitive coil. This was due to the extreme state of desiccation and lack of any appreciable intracellular or extracellular water in the specimen. After multiple attempts, the study was aborted.
Ultra-High-Resolution, Flat Panel Volume CT
A flat panel volume CT (fpVCT) scanner combines the advances in CT with digital flat panel detector technology.3 In simple terms, one can think of a flat panel volume CT as a conventional MDCT in which the rows of detector elements have been replaced by an area detector composed of a matrix of detector elements.4 It is, therefore, capable of producing a larger number of sections (as many as 768 for the current prototype), spanning approximately 18 cm in 1 rotation. The large z-coverage afforded by these scanners is sufficient to image a mummified head in 1 axial scan. Unlike micro-CT, fpVCT provides a much larger viewing area and is suitable for large specimens, in vivo imaging of large animals, and humans.
The current fpVCT prototype (Siemens Medical Solutions) uses a PaxScan 4030CB (Varian Medical Systems, Palo Alto, Calif) cesium iodide (CsI), amorphous silicon flat panel detector.5 With an active area of 40 × 30 cm2, this detector provides an FOV of 25 × 25 × 18 cm3 when geometric magnification is taken into account. The detector panel consists of a 2048 × 1536 matrix of elements, each with a dimension of 194 μm2. As the gantry rotates, projection images of the anatomy are acquired. The 2D projections are reconstructed into a volumetric stack of sections by using a 3D reconstruction algorithm. The mummy was scanned at 120 kV and 50 mA. Six-hundred views were acquired and reconstructed in approximately 800 sections, each with 1024 × 1024 pixels.
By virtue of their ultra-high, isotropic spatial resolution (∼200 μm), fpVCT systems bring into focus anatomy that heretofore has been in the domain of microscopy.6 For example, by using fpVCT, we are able to directly visualize the trabecular structure of the bone.7 This could help us infer any metabolic disorders (eg, osteoporosis) by observing their effect on the trabecular structure of bone. In addition, at 200-μm resolution, the sharpness and the quality of edges in any osteotomies made during the mummification process could be directly visualized in the CT images. This level of detail has the promise of revealing Djehutynakht's skull anatomy and the mummification process in unprecedented detail.
3D Processing
The data acquired from these various studies were analyzed by using the Leonardo workstation (Siemens Medical Solutions). By appropriate window and level controls, the data were separated into the soft tissue and bone structures to create images of the mummy's bust and its skull. These were then further manipulated to create cut-away views, as well as projections from an arbitrary viewpoint.
Results
All of the features visible in MDCT were also visible in fpVCT. As expected, fpVCT offered higher spatial resolution and greater anatomic detail. Therefore, in the analysis that follows, only fpVCT images are shown and analyzed. The volumetric images showed excellent bony detail and the soft tissue, including the skin surface. A photograph of the mummy head is shown in Fig 1. The wrapping covering the skin surface can be visualized clearly in this photograph.
Calvaria
Figure 2 shows surface-rendered views of the skull of the mummy from different viewpoints. As can be seen, the calvaria are intact above the level of the orbital rims. The bone is well mineralized and the cortical thickness normal, indicating that Djehutynakht was probably young and did not suffer from osteoporosis or any other metabolic bone disorder.

Multiple 3D surface-rendered views of the mummified skull showing the various surgical defects discussed in this article and detailed in subsequent illustrations.
In the posterior, occipital/suboccipital location, there is an extensive area over which the scalp is missing. This is best seen in the left-most image in Fig 3. The linen covering this area is deficient as well. The underlying skull, however, is intact without any evidence of a depressed fracture or surgical defect. These changes most probably occurred well after the mummification process, probably as a result of rough handling or deliberate mutilation of the mummy.

Posterior, anterior, and oblique views of the wrapping around the head. Notice the posterior occipital scalp defect and the near-normal appearance of the malar region despite extensive mutilations to the facial skeleton.
Skull Base
Anterior Cranial Fossa.
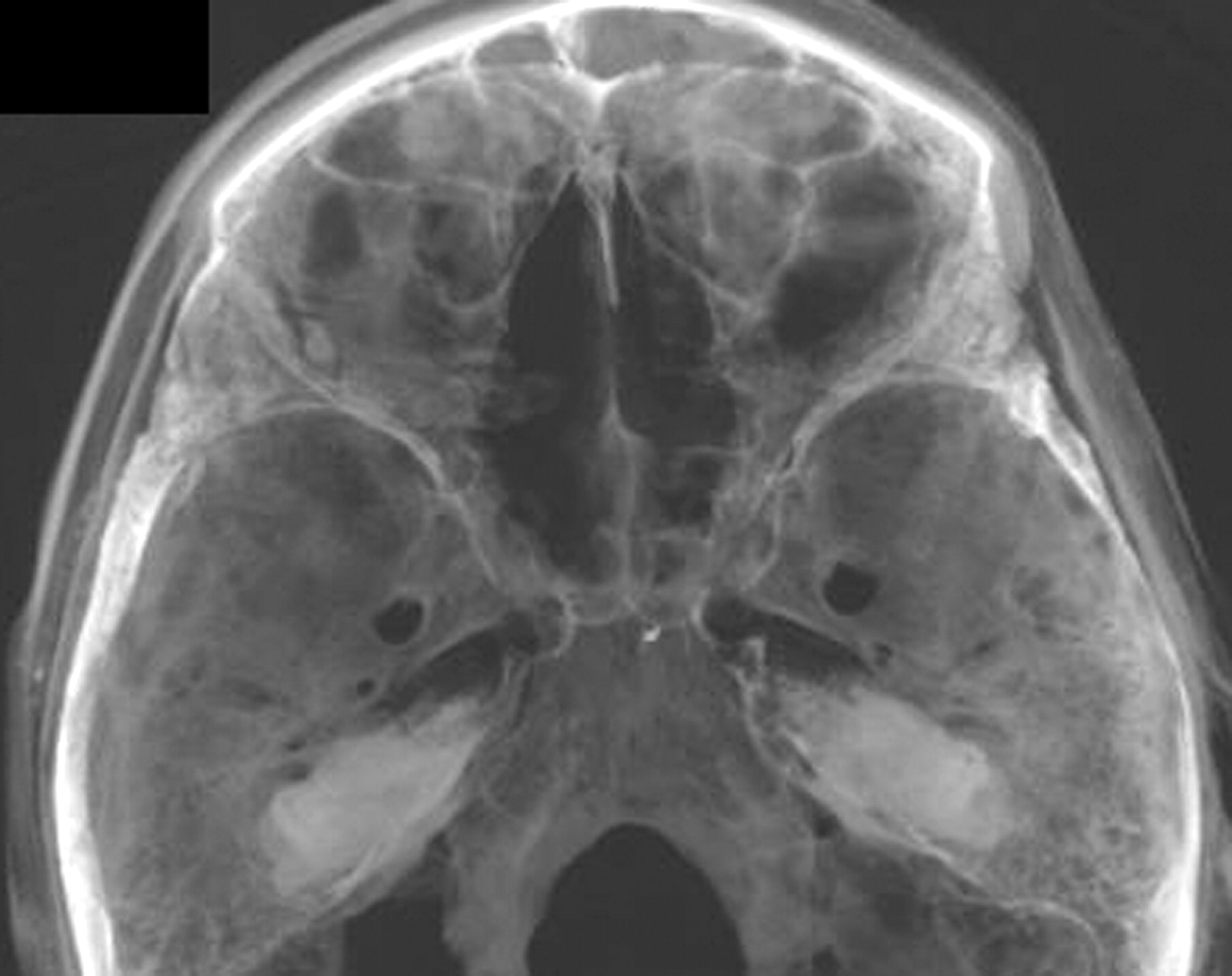
Figures 4 and 5 depict the anterior and middle cranial fossae. In the anterior skull base, the middle portion of the cribriform plate has a large defect, just posterior to the crista galli. The ethmoid air cells in this section have been removed. This defect makes the anterior cranial fossa communicate with the nasal cavity and the outside. It also makes the cranial vault communicate with the oropharynx through the portion where the soft palate would have been and through the choanae. The hard palate is intact as are the medial and superior walls of the orbits.

A slightly transparent view from the top of the cranial vault showing anterior and middle cranial fossa. The defect in the cribriform plate is apparent, and, through it, the contents of the nasal cavity can be partially visualized.

A surface-rendered, inferior view looking up (left) and a superior view looking down (right), showing the defect in the cribriform plate that establishes a communication between the nasal cavity and the intracranial space.
Middle Cranial Fossa.
The sphenoid bone is intact (Figs 4 and 5). The sella turcica can be visualized and has not been violated. The hamuli of the lateral pterygoid plates are intact bilaterally. The major foramina of the skull base can be visualized.
Posterior Cranial Fossa.
At the base of the posterior cranial fossa, adjacent and to the left of foramen magnum, there is a large defect in the occipital bone (Fig 6). It occupies the space between the foramen magnum and the petrous ridge and is confluent with the jugular foramen. The adjacent styloid process has been fractured. In the desiccated mummy, this defect in the bone makes the posterior cranial fossa communicate with the posterior oropharynx; in a cadaver or in life, there would have been intervening soft tissue. The rim of the foramen magnum itself is intact.

Inferior views looking up (top and bottom left), and a superior view looking down (bottom right) showing the defect in the posterior cranial fossa, illustrated with the help of 2 clip planes. Note the jagged nature of the margins of this defect.
The margins of the defect are somewhat irregular, suggesting that the bone had been removed piecemeal, rather than having been sharply cut away as a single piece with a bone saw. The bone defect is well removed from the area of superficial tissue loss on the posterior surface of the skull, making it extremely unprobable that the latter provided access to the skull base. Access to this area would have been most expeditiously gained from a lateral retromastoid approach.
All of the cervical vertebral bodies are missing. There is a gap where the trachea and the esophagus descended into the thoracic cavity.
Nasal Structures and Palate
The nasal bones are intact. The external appearance of the nose has been restored by the linen (Fig 7). The nasal turbinates on the left have been removed, and, as noted earlier, there is a defect in the left side of the cribriform plate. The right side of the cribriform plate has a smaller defect. The nasal septum is partially resected, because the middle and superior part of the nasal septum is missing. The anterior nasal septum and the nasal philtrum are present. There is diastasis of the suture between the frontal process of the maxilla and the nasal bones bilaterally.

A zoomed in, left superior oblique view showing the weaving pattern of the headband and the wrapping over the forehead and the nose.
Facial Structures
The head was wrapped in 7 layers of a thin, gauzelike linen that is not very attenuating to x-rays, as measured by the CT number. The weave of this material is hard to discern, though it can be distinguished from skin by its lower attenuation. The thickness of the linen molding varies and was shaped to give form to the face, especially where bone has been removed (eg, bilateral zygomas, Fig 7). In parts of the head, air has dissected between the cloth and skin surface. No facial lacerations or deliberate incisions are identifiable because of the preparation.
Zygoma and Zygomatic Arch.
There is a displaced zygoma complex or tripod fracture on the left (Fig 8). There is no evidence of healing, and these fractures are postmortem. There is diastasis of the sutures between the zygoma and its neighboring bones (ie, the left maxillary bone, the frontal bone, and the greater wing of the sphenoid). The body of the left zygoma is dislocated into the space of the left maxillary sinus. The posterior part of the left zygoma and the entire right zygoma have been removed.

Missing right zygoma (left image) and left zygoma complex fracture (arrow in right image). The attenuated bone fragment near the nasal opening in the left image probably represents a tooth fragment. The body of the left zygoma is free floating, because it has been disarticulated from the surrounding bones and pushed into the left maxillary sinus.
On both sides, the midportion of the zygomatic arch has been removed (Fig 9). There is a sharp-edged resection of the inferior medial surface. The missing fracture fragment is not identified in the specimen.

Left and right lateral views (top and bottom rows, respectively) showing resected zygomatic arches and the coronoid processes of the mandibles bilaterally. The images on the left are surface rendered to depict the sharp edges of the osteotomies.
The anterior walls of the maxillary sinuses and inferior orbital rims have been destroyed (Figs 8 and 9). The roofs and medial walls of both orbits are intact. Although the bone destruction is extensive, there is remarkable symmetry to bone removals. With the exception of the displaced fragment of the left zygoma, all of these bones have been completely excised.
The external malar contours have been reconstructed bilaterally by using linen wrapping and layers of glue-like material that, on CT, have the attenuation of soft tissue (Fig 3). By virtue of this postmortem restoration, the superficial appearance of the face belies the extensive surgical alterations that lie underneath.
Mandible and Temporomandibular Joints.
Both coronoid processes of the mandible have been surgically removed by sharply defined cuts of the anterior and superior medial surfaces of the mandibular rami (Fig 10). The zygomaticotemporal arches have been partially or completely removed, again by a sharp instrument. The mandibular condyles are seated in the glenoid fossae bilaterally. The articular tubercles of the mandibular fossae have been fractured on both sides (Fig 11). The right styloid process of the temporal bone is intact. The left has been excised.
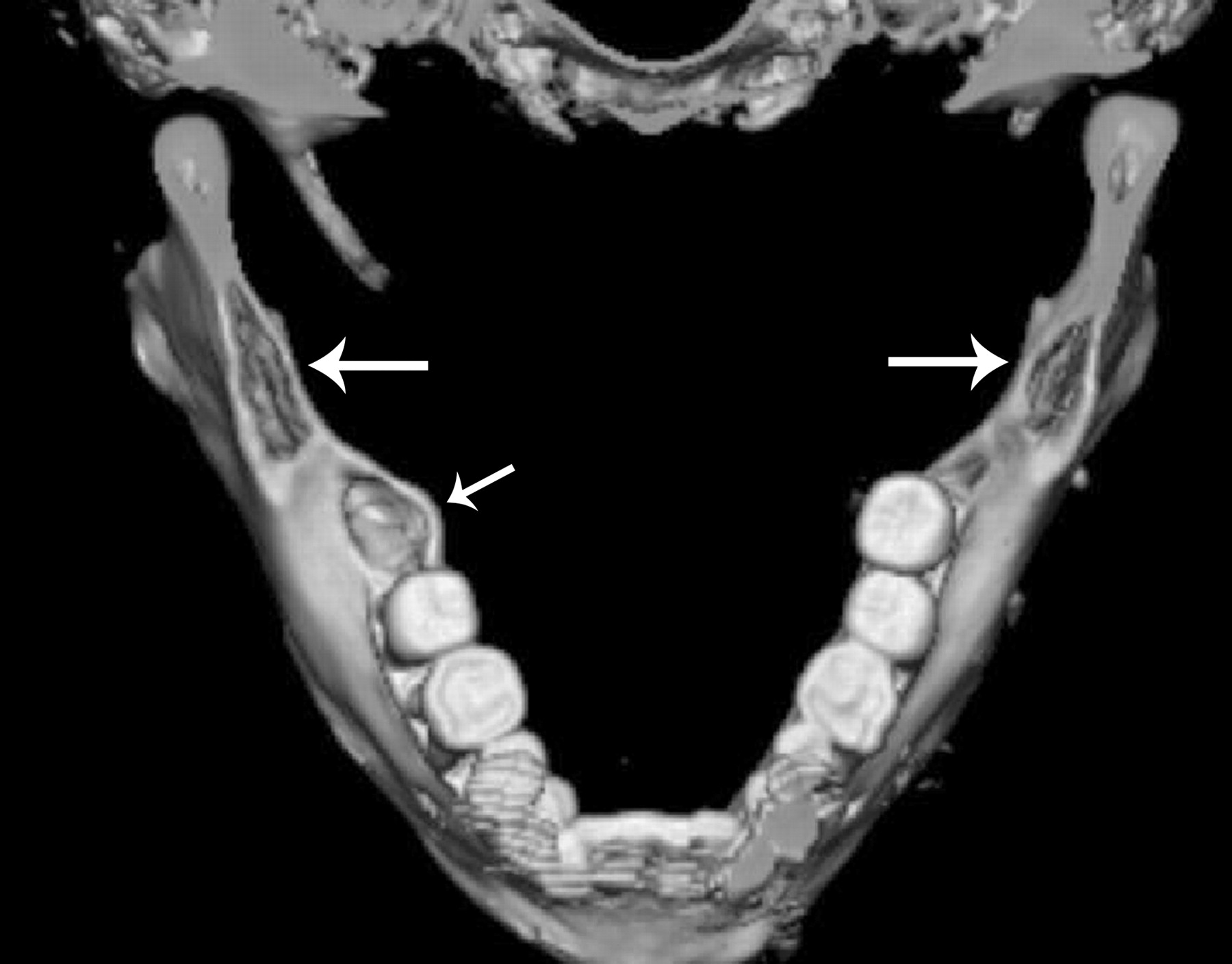
A superior view of the cut surface of the coronoid processes (thick arrows). The right styloid process is intact; that on the left has been sharply resected. Also note the socket of the third right molar (small arrow).

Detail of left temporomandibular joint showing the sharp resection margin of the coronoid process, fracture of the articular tubercle of the mandibular fossa, and sharp resection margins of the zygomatic arch.
Dentition.
There are 15 mandibular teeth (Fig 12). The last mandibular molar on the right (ADA 32) has been removed, and the socket for this molar is visible. All 3 of the molars on the left are intact.

A slightly oblique view of the dentition.
The middle 10 maxillary teeth are present. These include the middle and lateral incisors, the canines, and the 2 premolars, bilaterally. The second premolar on the left is partially fractured. A periapical lucency in the left central incisor in the maxilla may represent dental disease or may be an artifact of postmortem dental trauma during preparation.
There is a dense object just inferior to the right nasal opening and anterior to the maxillary alveolar ridge that may be a broken tooth or a bone fragment. It appears to be on the skin surface beneath the linen, rather than subcutaneous or intraoral.
Discussion
Brain Removal or Excerebration
For persons with even a casual interest in Egyptian mummies, brain removal has always had particular interest and appeal. It is generally accepted that the procedure was commonly performed beginning at the time of the New Kingdom (1550–1070 BC).8 Less certain is the frequency with which excerebration was performed before this. There are rare examples of artificial cribriform defects in skulls attributed to the Old Kingdom (2575–2100 BC). Even in skulls of that earlier period, which lack an artificial skull defect, some authors have hypothesized that brain removal might have been performed through the foramen magnum. There is, however, no firm evidence for this. Similarly, during the Middle Kingdom (2040–1640 BC), there are only occasional examples of excerebration among the human remains.9
Djehutynakht dates to the early days of the Middle Kingdom and, therefore, represents one of the few examples of brain removal during that early time. Although the defect in the cribriform plate is consistent with previous descriptions of excerebration, the occipital bone defect is of particular interest. There is only 1 other example of such a defect, and that specimen also dates to the Middle Kingdom (Fig 13).10 Given the historic evidence and the presence of an artificial defect in the cribriform plate, it is fair to deduce that at least part of Djehutynakht's brain was removed through the nasal cavity, keeping the anterior nasal septum intact. The process involved inserting a hooked probe through the cribriform defect to macerate the brain and its coverings so that they could be withdrawn piecemeal. This was probably facilitated by repeated irrigation, placing the cadaver prone to encourage drainage of the intracranial contents.11 The anterior and middle cranial fossae could be expeditiously evacuated in this manner. Any tissue remaining in the posterior cranium could then be extracted through the occipital defect. Later in Egyptian history, there are definite examples of posterior excerebration by enlargement of the foramen magnum.12

Middle Kingdom female skull from the Dashur pyramid of Amenemhet III.10
Mutilations of the Facial Skeleton
Although the skull-base defects related to brain removal are unusual, there are known precedents among documented remains from ancient Egypt. On the other hand, the facial mutilations are unique. The previous radiographic investigation of the mummy head had detected only destruction of the anterior walls of the maxillary sinuses and inferior orbital rims. It was assumed that the object of these bone removals was to facilitate excerebration. This conclusion is not tenable given the fact that the roofs and medial walls of both orbits are intact. This would have precluded the embalmers gaining access to the intracranial space through the maxillary sinuses and orbits. Given the other extensive symmetrical nature of the bone removals, one must look elsewhere for a rationale. On each side not only the anterior wall of the maxillary sinus and inferior orbital rim had been removed but also the zygoma and zygomatic arch, as well as the coronoid process of the mandible. It is of interest that, with the exception of the displaced fragment of the left zygoma, all of these bones have been completely excised. This procedure would have required considerable effort, expertise, and an understanding of functional anatomy.
In seeking a rationale for these mutilations, it is noteworthy that the zygoma, zygomatic arch, and coronoid process of the mandible are all sites of attachment for the largest muscles of mastication (temporalis and masseter). In addition, bilateral fracturing cuts have been made in and around the temporomandibular joint by using a sharp instrument. This would detach the remaining pterygoid muscles and the temporomandibular ligament (Table), completing the detachment of muscles of mastication from the mandible.
Origin and insertion of the various muscles of mastication*
The effect of all of these maneuvers taken together would be to completely mobilize the mandible. Each step in the process is specifically directed toward this end. The initial step on each side might have been to remove the anterior wall of the maxillary sinus and inferior orbital rim by a transoral, sublabial approach. In the present day, this is a standard surgical approach to the maxillary sinuses. Wide entry into the maxillary sinuses would have given the embalmer access to the zygomas and adjacent inferior rim of the orbit. If rigor mortis were present, as seems probable, it would be necessary to partially mobilize the mandible at this point to more adequately expose the body of the zygoma and the more posterior zygomatic arch to remove these structures. Partial mobilization of the mandible could be accomplished by positioning a chisel against the coronoid process in the retromolar trigone and driving it posteriorly. Transection of the coronoid process at its base would effectively detach the temporalis muscle. The chisel could now be advanced more deeply to the temporomandibular joint simply by feeling the location of the hinge point of the joint. Once the pterygoid muscles and the temporomandibular joint ligament were transected at their point of attachment to the mandible, the jaw would open sufficiently to provide access to the zygomas and zygomatic arches, particularly if the coronoid processes had been excised. It should be noted that modern surgical procedures remarkably similar to this are used to perform coronoidectomies to treat conditions associated with limited mobility of the jaw.13 In fact, the zygomatic arch may also be mobilized to allow wider surgical exposure during coronoidectomy.
It should be emphasized that, although the totality of structural mutilations is quite extensive, the only thing that they all ultimately have in common is their association with mandibular function and mobility. One might consider the removal of the maxillary sinus walls and inferior orbital rims as an exception; however, this was necessary to gain transoral access to the deeper structures. It is striking that all of the involved bony structures were not only mobilized but also removed. This remarkable technical feat was presumably performed not only to provide the widest possible anatomic exposure through a limited space but also to assure that the largest muscles of mastication were truly detached.
It has already been explained that entry into the maxillary sinuses and inferior orbits could not have had any role in excerebration. Similarly, removal of the zygomas and adjacent structures would not provide access to the anterior or middle cranial fossa for brain removal. It is relevant in this regard that the more medially situated pterygoid plates and hamulus bones are undisturbed. From this evidence it is safe to assume that the purpose of these extensive mutilations was unrelated to excerebration.
Significance of Facial Mutilations
Hypothetically, one might consider that the purpose of these mutilations was to reach the occipital skull base through the mouth to perform the observed skull defect to the left of the foramen magnum. Not only would this route for exposure of the posterior fossa skull base have been quite a task technically, it is difficult to imagine that the embalmers would have gone to this effort to arrive at an anatomic point that could be accessed very easily from the posterior direction. In addition, the only other example of a similar occipital skull defect (Fig 13) shows no evidence of the other mutilations that we have described.10
The purpose of such mutilations can only be conjectured. It is difficult to believe that it was done simply to remove tissue from the facial skeleton and oropharynx for purposes of embalming. It was very important to the ancient Egyptians to preserve the living appearance of the deceased as much as possible after death. Removing the zygomas, inferior orbital rims, and zygomatic arches would have significantly altered the facial contour. To accommodate for this, Djehutynakht's physiognomy was meticulously recreated with linen wrappings and packing. This is readily apparent from our images (Fig 3).
It is more probable that the jaw was mobilized for some other purpose that took precedence over simply preserving the mummy's appearance. Although this could have been done simply to gain deeper access to the oral cavity, it is more probable to have had some more important ritual significance. From the time of the pyramids until the last days of ancient Egyptian history, one of the most important parts of the funerary ritual was the “Opening of the Mouth” ceremony. The possibility that what we have observed in the case of Djehutynakht was somehow related to this rite deserves consideration. The “Opening of the Mouth” ceremony would be difficult to perform in the presence of rigor mortis; the facial mutilation described above would effectively overcome this problem by detaching the mandible from the muscles of mastication.
A limitation of this work is that a single mummified head was studied. This makes definitive assertion of the above deductions difficult. In addition, from the findings observed in 1 specimen, it is difficult to make the generalization for the mummification process as a whole. The hypothesis that the facial mutilations were done to facilitate the “Opening of the Mouth” ceremony can only be substantiated through radiologic study of other specimens from the same time period. In this regard, whereas other excellent radiologic surveys have been presented in the literature (eg, those Raven and Taconis8 and Hoffman and colleagues14,15), there is a paucity of research material from the Middle Kingdom.
Less conjectural is the significance of our findings with regard to the knowledge of functional anatomy of the jaw possessed by the ancient Egyptians. The skill and efficiency with which the mutilations were performed reflect a remarkable grasp of skeletal anatomy and its relation to mandibular function. The Edwin Smith Surgical Papyrus is one of our most important sources of information concerning ancient Egyptian medicine.16 Its origins postdate (∼1600 BC) the time of Djehutynakht. The 48 cases that it describes and discusses are principally of a traumatic nature with surgical implications. More than half are injuries of the head and face, 10 of which describe trauma in the region of the zygoma, maxilla, mandible, and/or temporal bone. There is 1 case of a dislocated mandible.
Among the anatomic terms used in the papyrus, there are several relating to the jaw and its function that are unique to this article. In his authoritative translation, Breasted16 was struck by the anatomic sophistication of the text with regard to the structure of the temporal bone, zygoma, and mandible and their relation to the action of the jaw. He remarked, “It has been customary to attribute the Egyptian's knowledge of human anatomy to the familiarity of the embalmer with the bodies he was eviscerating and embalming. Here, however, we find the surgeon familiar with a muscle of the head which was never touched by the embalmer. His knowledge of it could have come only from dissection and from treatment of wounds.” Based on our present findings, this statement must be qualified. In fact, it is quite possible that the anatomic and functional details contained in the papyrus derive entirely from the quite sophisticated dissections performed by the embalmers and reflected in the mutilations evident in Djehutynakht's mummy.
Acknowledgments
We thank the following individuals who made the scanning and 3D imaging of this mummified head possible: Dr Gordon Harris (director, 3D imaging laboratory), Jennifer McGowan (operations manager, 3D imaging laboratory), and Dennise Palumbo, RN, MSN (executive director, radiology).
Footnotes
This research was partially supported by a research grant (204410) from the Center for Integration of Medicine and Innovative Technology.
References
- Received September 18, 2007.
- Accepted after revision October 17, 2007.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}