
Abstract
BACKGROUND AND PURPOSE: During percutaneous polymethylmethacrylate (PMMA) vertebroplasty (PV), PMMA cement may migrate into the venous system and subsequently be transported to the pulmonary arteries. Frequency, outcome, and imaging findings of PMMA pulmonary embolism are poorly understood. We retrospectively assessed the frequency and outcome of PMMA embolism during PV in a large patient cohort and evaluated the relationship of the volume of injected PMMA to the occurrence of pulmonary PMMA embolism.
MATERIALS AND METHODS: Between 2001 and 2007, 532 osteoporotic compression fractures in 299 consecutive patients were treated with PV. PMMA embolism was defined as venous PMMA migration toward the lungs visible on biplane fluoroscopy during PV. CT was performed immediately and 1 year after PMMA migration.
RESULTS: Venous PMMA migration occurred during 11 PVs in 11 patients (2.1%, 95% confidence interval, 1.1–3.7%). CT in 8 patients demonstrated small peripheral pulmonary PMMA emboli. All 11 patients remained asymptomatic during 1-year follow-up. Repeat CT scanning after 1 year in 6 patients demonstrated unchanged pulmonary PMMA deposits without late reactive changes. Mean injected cement volume in patients with and without PMMA embolism was not different (3.6 ± 1.06 mL versus 3.3 ± 1.16 mL, P = .43). Similar comparison for thoracic and thoracolumbar vertebrae yielded P values of .07 and .9.
CONCLUSION: Pulmonary PMMA embolism during PV is an infrequent complication without permanent clinical sequelae. After 1 year, no pulmonary reaction was seen on CT. No definite relationship of PMMA emboli with injected cement volume could be established.
Percutaneous polymethylmethacrylate (PMMA) vertebroplasty (PV) is increasingly used for pain relief in patients with symptomatic vertebral compression fractures. Since the introduction of PV in 1987, its safety and effectiveness have been confirmed in several studies.1–6 Complications of PV are rare and, if they occur, are mostly related to PMMA leakage outside the treated vertebral body into adjacent anatomic structures. During PV, PMMA may migrate into the venous system and is subsequently transported to the pulmonary arteries. Frequency, outcome, and imaging findings of such PMMA pulmonary embolism are poorly understood.
In this study, we retrospectively assessed frequency and clinical and imaging outcomes of PMMA embolism during PV in a large patient cohort. In addition, we evaluated whether the volume of injected PMMA is a risk factor for the occurrence of pulmonary PMMA embolism.
Materials and Methods
This study was approved by the institutional review board and written patient informed consent was obtained.
Patients
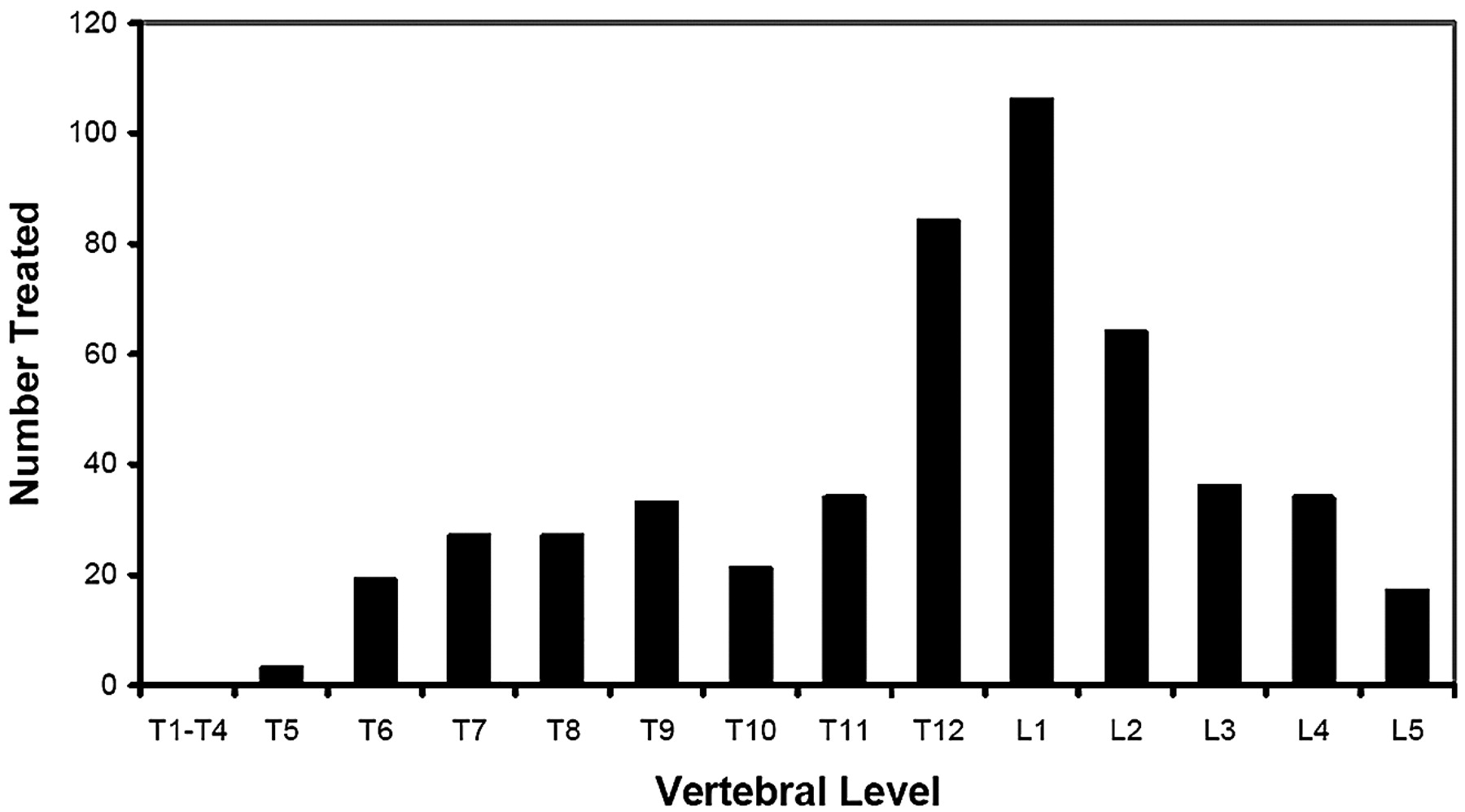
Between October 2001 and June 2007, PV was performed in 299 consecutive patients with osteoporotic vertebral compression fractures. In 197 patients, 1 vertebra was treated; in 102 patients, 2 were treated; and in 24 patients, 3 were treated. During follow-up, new fractures were treated with PV in 59 of 299 patients. Altogether, 532 osteoporotic vertebral compression fractures were treated. Of 299 patients, 60 were men and 239 were women, with a mean age of 73 years (range, 47–94 years). The location of treated vertebra is displayed in Fig 1.
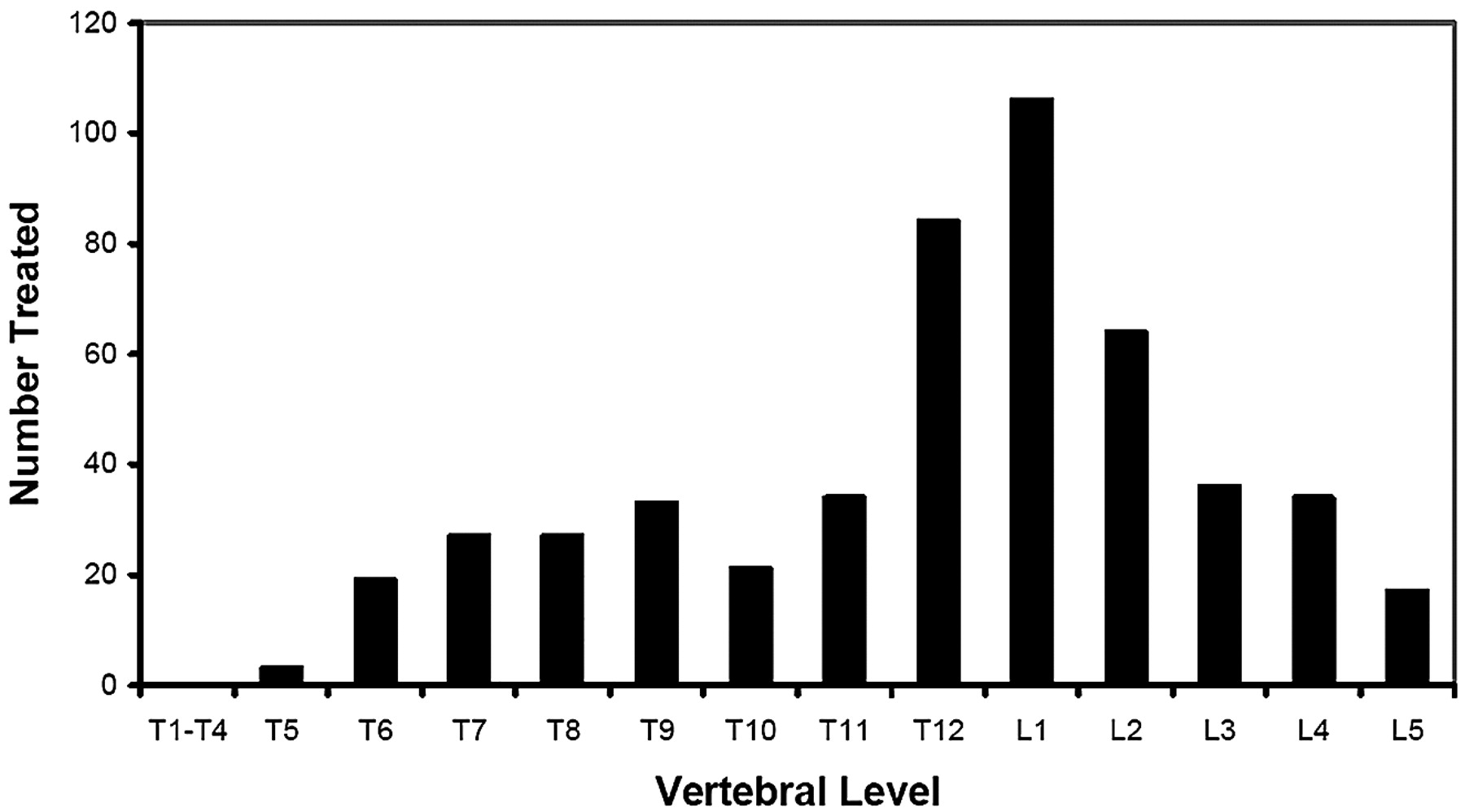
Graph shows the distribution of treated osteoporotic compression fractures.
Vertebroplasty
PV was performed on a biplane angiographic unit (Integra BN 3000 Neuro; Philips Medical Systems, Best, the Netherlands). After local anesthesia was administered, two 11- or 13-gauge needles were bilaterally transpedicularly inserted into the vertebral body. We injected PMMA under continuous biplane or lateral fluoroscopy, alternating both pedicles by using 1-mL syringes until it reached the posterior one fourth of the vertebral body. Whenever epidural or paravertebral leakage was observed, injection was stopped. When needed, the injection was resumed after a 15- to 20-second delay without changing needle position. The volume of injected cement in each treated vertebral body was recorded.
Definition of Pulmonary PMMA Embolism
“Pulmonary PMMA embolism” was defined as venous PMMA migration toward the lungs, visible on fluoroscopy. If migration occurred, any clinical changes were recorded and a native chest CT was performed immediately after the procedure to detect the location, number, and distribution of PMMA emboli and possible reactive changes of the lung parenchyma.
Follow-Up of Patients with Pulmonary PMMA Embolism
Medical records of patients with pulmonary PMMA embolism were reviewed for possible related cardiovascular symptoms. In October 2007, surviving patients were contacted and requested to fill out a short questionnaire regarding cardiovascular symptoms after PV. In addition, they were invited for repeat native chest CT for comparison with CT performed immediately after PV.
Statistical Analysis
Frequency of pulmonary PMMA embolism was assessed per treated vertebra as a proportion with 95% confidence intervals (CI). Mean volume with SD of injected PMMA per vertebra was assessed for all 462 vertebrae in which injected cement volume was recorded and separately for thoracic (T5-T10), thoracolumbar (T11-L2), and lumbar vertebrae (L3-L5), both in patients with and without pulmonary PMMA embolism. A t test was used for comparison.
Results
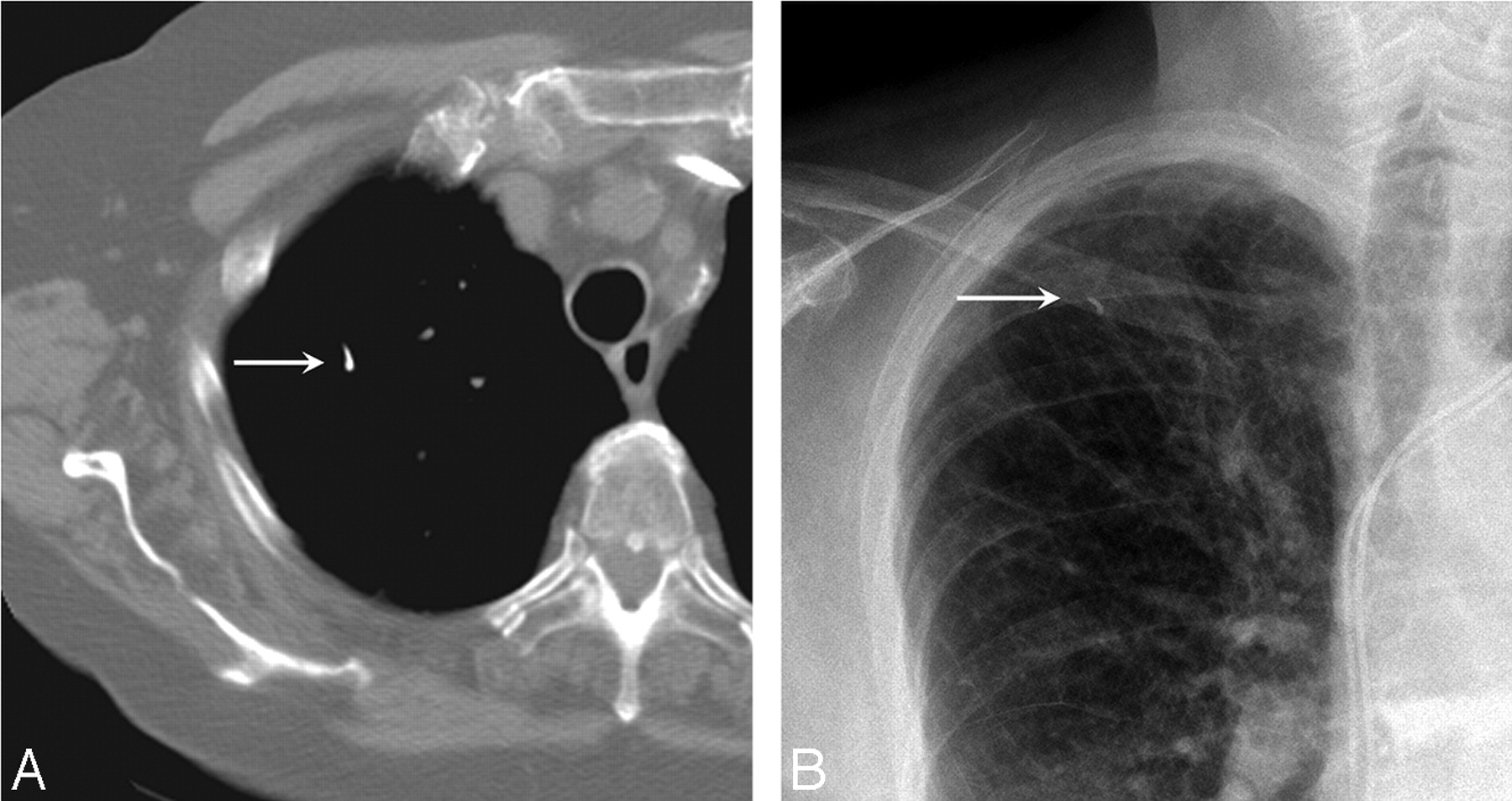
In 532 PVs in 299 patients, pulmonary PMMA embolism occurred in 11 procedures (2.1%; 95% CI, 1.1–3.7%) in 11 patients (Table and Fig 2). Native chest CT scanning in 8 patients demonstrated 1–3 small (2–6 mm) peripheral punctuate or tubular hyperattenuations randomly distributed in 1 or 2 lobes without reactive pulmonary changes. No PMMA depositions were present in the heart or central pulmonary arteries. In none of 11 patients did clinical symptoms develop during PV or afterward during hospital admission. No additional medical treatment, such as anticoagulation, was administered, and the hospital stay was not extended. After a mean follow-up of 12 months (range, 5–22 months), 2 patients died of metastatic cancer and 1 patient could not be traced. The remaining 8 patients reported no cardiopulmonary symptoms. All 8 patients agreed to native chest CT scanning, and in 6 of 8, results could be compared with previous CT (mistakenly, 3 patients had no initial CT after PV). In all 8 patients, CT scans showed findings similar to those on initial CT without reactive pulmonary changes. In 6 patients with initial and follow-up CT scans, findings were unchanged.
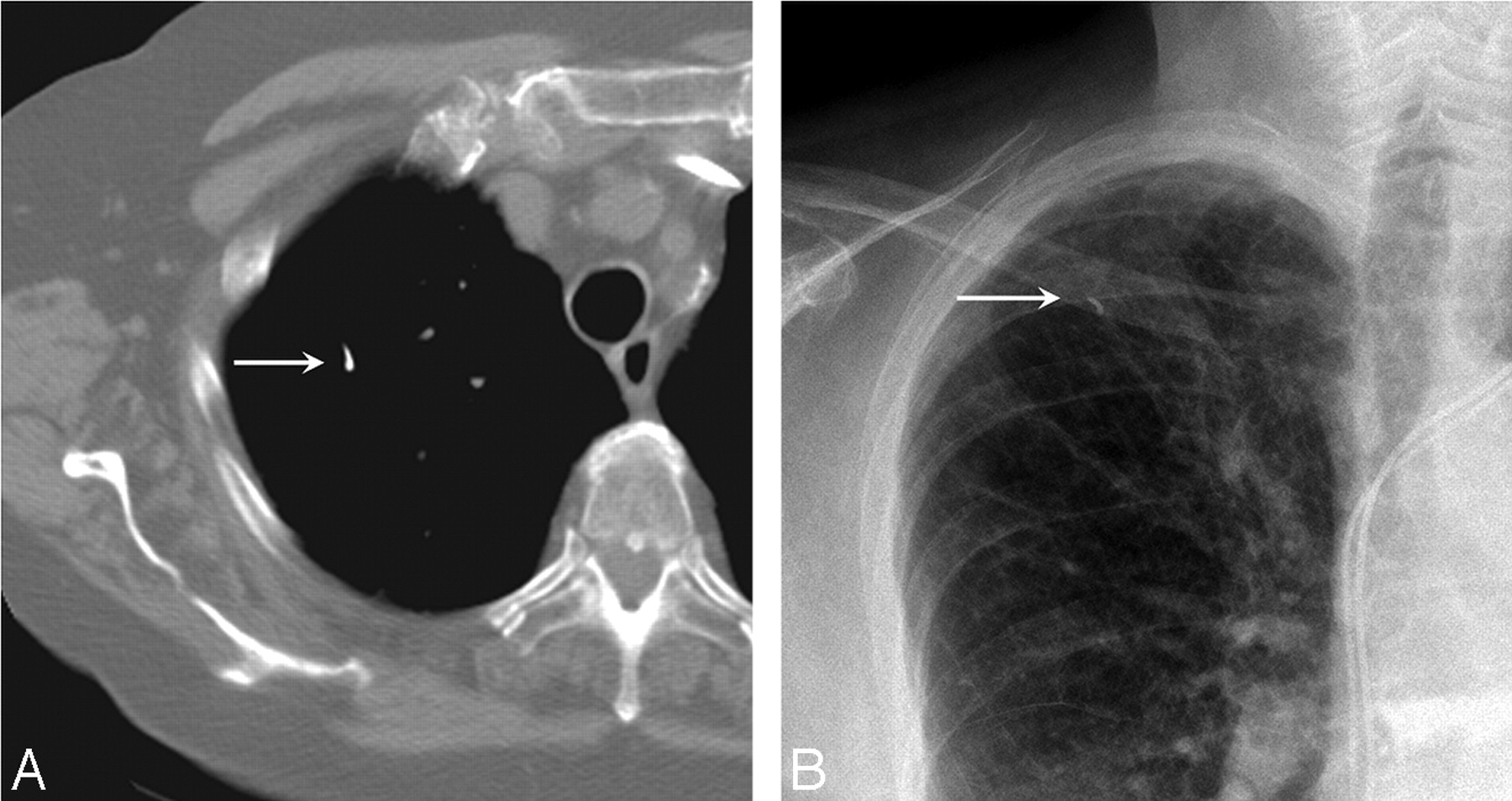
A small pulmonary PMMA embolus is seen in the right upper lobe visible on a native chest CT scan (A) and on a chest radiograph (B).
CT findings in patients with pulmonary PMMA embolism during PV
Mean cement volume in 462 vertebrae in which injected volume was recorded in patients without PMMA embolism was 3.3 ± 1.16 mL (range, 0.5–9 mL), and in 11 vertebrae in patients with PMMA embolism, this was 3.6 ± 1.06 mL (range, 2.6–5.5 mL). This difference was not significant (P = .43).
Similar comparison was done for thoracic (116 versus 5, P = .07), thoracolumbar (272 versus 5, P = .9), and lumbar (74 versus 1, P = invalid) vertebrae. Although there was a trend toward more injected cement volume in patients with pulmonary PMMA during PV of thoracic vertebrae, this was not significant.
Discussion
Pulmonary PMMA embolization during PV for compression fractures is rare, with an incidence of 2.1%. CT demonstrated small PMMA deposits in segmental or subsegmental pulmonary arteries without early or late reactive pulmonary changes. No PMMA depositions were present in the heart or central pulmonary arteries. In none of the patients did clinical symptoms develop during 1-year follow-up.
The low frequency of pulmonary PMMA embolism is confirmed in other observational studies with frequencies of 0%–4.8%.6–11 Combined data of this and other studies6–11 of 1791 VPs indicate a frequency of 1.3%, with a narrow 95% CI of 0.9–1.8%. We could not establish a definite relation of injected cement volume with the occurrence of PMMA embolism, though there was a trend toward more injected cement volume in patients with pulmonary PMMA during PV of the thoracic vertebrae. In most cited studies, patients with PMMA embolism remained asymptomatic. In a large study of 1000 PVs,6 PMMA embolism occurred in 8 patients. In 1 patient, this embolism was symptomatic, with transient pleuritic chest pain and dyspnea, despite a low volume of injected cement.
On the other hand, in several cases, severe or fatal clinical complications of PMMA embolism were reported.12–17 In all cases, there was evidence of a large injected total PMMA volume (9–15 mL) or a large amount of PMMA in the heart or central pulmonary arteries. This suggests that in these cases, venous cement migration was not fluoroscopically detected in a timely manner.
In our opinion, supported by others, with proper use of fluoroscopy and a limited volume of PMMA injected in repeated small quantities, pulmonary PMMA embolism will rarely occur. If it does occur, only very small quantities of PMMA will be transported to the pulmonary arteries, which will hardly ever cause symptoms and, in all cases, will be without permanent clinical sequelae. Therefore, standard chest radiographs or CT after PV is not warranted.
Next to PMMA embolism, intramedullary fatty bone marrow embolism may occur, a well-recognized phenomenon in orthopedic surgery.18 Injection of bone cement may force fatty bone marrow into disrupted medullary veins; this marrow will migrate to the pulmonary vessels. The migration may cause increased pulmonary resistance, hypoxemia, and thus decreased cardiac output.12,19 In an experimental study of PV in a sheep model,20 PV provoked an initial reflexive decrease in heart rate and arterial blood pressure followed by fat and bone marrow emboli passing through the heart into the pulmonary vasculature. This result indicates that fat embolism also may occur during PV in humans. Apparently, these fat emboli are well tolerated in patients without associated cardiopulmonary disease. However, especially in patients with compromised cardiopulmonary reserve, it seems sensible to limit the levels treated per session and the injected PMMA volumes per vertebra.
Conclusion
Pulmonary PMMA embolism during PV was an infrequent complication in our series and had no short or midterm clinical sequelae. After 1 year, no pulmonary reaction was seen on CT. Although there was a trend toward more injected cement volume in patients with pulmonary PMMA during PV of thoracic vertebrae, this was not significant.
References
- Received May 26, 2008.
- Accepted after revision June 30, 2008.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}