
Abstract
SUMMARY: An organized hematoma is a chronic state of fibrotic tissue surrounding a hemorrhage. A mass lesion resulting from hematoma in the maxillary sinus was first reported in 1917, and the term, “blood boil,” was clinically coined from such features as encapsulated blood and locally aggressive behavior. Subsequently, others have reported lesions with a similar appearance and clinical course, and now, in Japan, blood boil is used as a clinical term for such lesions. Factors that may predispose a patient to hematoma formation vary, and the pathogenesis of the mass is still uncertain. The lesions are mainly composed of an organized hematoma, regardless of their origin. We present 2 cases of organized maxillary sinus hematomas that have unusual radiologic findings and correlate these findings with the histopathologic findings.
Case Reports
Case 1
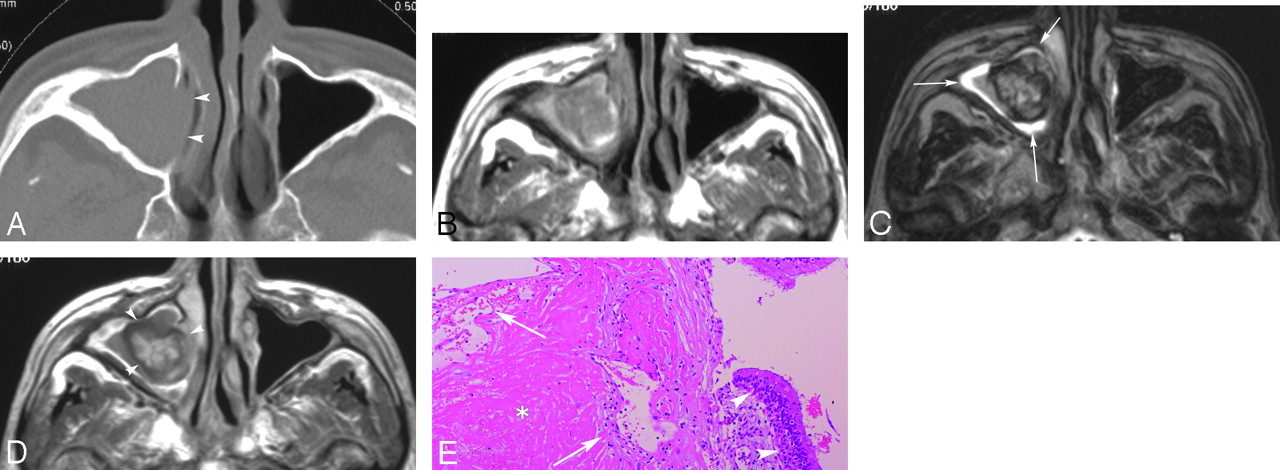
A 22-year-old man was referred to the otolaryngology department with a 6-month history of nasal congestion and swelling in his left cheek. When he was examined in our hospital, no epistaxis or neurologic deficit was noticed. There was no history of hematopoietic disorder. Endonasal examination revealed a pinkish mass in the left nasal cavity. The nasal septum was deviated to the right. A CT scan showed an 8-cm mass in the left maxillary sinus, which was primarily expansile with focal areas of bone loss (Fig 1A). On MR imaging, the mass had a slightly high T1-weighted signal intensity, heterogeneous low-to-high T2-weighted signal intensity, and scattered areas of well-demarcated enhancement on contrast-enhanced T1-weighted images (Fig 1B–D). A high signal intensity zone surrounded the mass on T2-weighted images (Fig 1C). A malignant tumor was suspected because of the size of the mass and the bony changes. Caldwell-Luc approach allowed en bloc resection of the mass. Pathology showed a fibrous encapsulated organized hematoma with surrounding inflamed mucosa without a neoplastic tissue (Fig 1E).

CT, MR imaging, and histopathologic findings in case 1.
A, The axial image of CT (bone algorithm) shows expanding mass in the left maxillary sinus. Expansile bone destruction (arrowheads) of the medial wall and bone defects (asterisks) of the anterior and posterior wall are observed.
B, T1-weighted spin-echo (TR/TE, 620 ms/15 ms) axial image depicts slightly high intensity areas on the mass. The left pterygopalatine fossa fat and the left retroantral fat are replaced by the mass (arrowheads).
C, T2-weighted fast spin-echo (TR/TE, 5000 ms/120 ms) axial image depicts curvilinear hyperintensity areas around the mass (arrows).
D, Contrast-enhanced T1-weighted spin-echo (TR/TE, 620 ms/15 ms) axial image clearly shows the antral and nasal parts of the mass (arrowheads). Markedly enhanced portions, which are clearly demarcated from nonenhanced portions, are observed in the mass.
E, Hematoxylin-eosin stains (low-power field, original magnification ×4) reveal the hematoma with organization in case 1. There is a reactive hyperplasia of endothelial cells in the hematoma (asterisks). Scattered fibroblasts are observed in the fibrous tissue margin (arrows). In the margin of the specimen, an inflamed columnar epithelium is confirmed (arrowheads). No tumoral cells are found.
Case 2
A 76-year-old man presented with a 5-month history of repeated nasal bleeding. He has been followed for cirrhosis for several years; however, no coagulopathy was present. Endonasal examination demonstrated a pinkish mass in the right nasal cavity, with medial displacement of the lateral nasal wall. On CT, a 2- × 3-cm mass displaced and thinned the medial antral wall (Fig 2A). On MR imaging, the mass was primarily isointense to muscle on T1-weighted images but contained areas of high signal intensity (Fig 2B). On T2-weighted images, there was a central region of high signal intensity surrounded by a low signal intensity zone, and a thinner rim of high signal intensity surrounded the entire mass (Fig 2C). The mass was markedly enhanced in a multinodular manner on contrast-enhanced T1-weighted images (Fig 2D). A malignant tumor was initially suspected because of a history of repeated epistaxis and the age of the patient. During surgery, the mass was totally resected by a transnasal approach. Histolopathology showed only a fibrous encapsulated organized hematoma (Fig 2E).
CT, MR imaging, and histopathologic findings in case 2.
A, The axial image of CT (bone algorithm) shows the mass in the right maxillary sinus. The pressure on the medial maxillary sinus wall has caused medial bowing of the wall (arrowheads).
B, T1-weighted spin-echo (TR/TE, 620 ms/15 ms) axial image depicts punctuate high signals on the mass.
C, T2-weighted fast spin-echo (TR/TE, 5000 ms/120 ms) axial image depicts a curvilinear hyperintensity area around the mass (arrows).
D, Contrast enhanced T1-weighted spin-echo (TR/TE, 620 ms/15 ms) axial image shows the mass (arrowheads). A central enhanced area corresponding with the area of central heterogeneous hyperintensity on T2-weighted image is observed in the mass.
E, Hematoxylin-eosin stains (low-power field, original magnification × 40) reveal the hematoma with organization in case 2. An admixture of fibrin network and hemorrhage (asterisk) is observed. There is a reactive hyperplasia of endothelial cells (arrows). An inflamed columnar epithelium is confirmed (arrowheads). No tumoral cells are found.
Discussion
An organized hematoma in the maxillary sinus is a rare lesion. Fewer than 100 cases1–8 have been reported to our knowledge. The mass usually originates in a single maxillary sinus and is generally located in the medial antral wall near the sinus ostium. Patients range in age between 20 and 76 years; no sex predominance is observed. It occurs in patients with and without a bleeding diathesis. The patient often presents with various symptoms that are caused by the mass, depending on the size and location. The most frequent symptom is nasal congestion and rhinorrhea because of the obstruction and secondary inflammatory process by the mass. Repeated epistaxis is reported in 70% of patients.2 Pain or facial swelling occurs when the mass compresses the adjacent structures. The mass gradually enlarges and causes pressure remodeling of the antral walls with some focal areas of apparent bone destruction. CT scans show an expansile maxillary sinus mass with some areas of bone resorption (Fig 1). On MR imaging, the mass usually has a variable signal intensity on T1- and T2-weighted images, ranging from low to high. After contrast administration, discrete areas of enhancement are present within the mass. The surrounding inflamed sinus mucosa, despite the bony changes, suggest a benign process on imaging.
The pathogenesis of organized hematomas has not been elucidated. However, Lee et al3 suggest a possible mechanism for the formation of an organized hematoma as follows: 1) repeated hemorrhage in the semiclosed lumen (maxillary sinus) forms a hematoma encapsulated by fibrosis; 2) the encapsulation prevents the absorption of the hematoma and induces vascularization, which causes rebleeding and increasing pressure within the hematoma; and 3) the progressive expansion of a hematoma causes the demineralization of adjacent structures. A variety of benign lesions or clinical states have been described in association with the development of an organized hematoma and they display similar conditions clinically and radiologically. Ozaki et al4 suggest that a hematoma originates from a hemangioma or an inflammatory vascular injury, and they define an organized hematoma without an underlying hemangioma as an inflammatory pseudotumor. A bleeding diathesis, an aggressive fungal infection, radiation therapy, a postoperative complication, or trauma are also potential causes of a similar condition.5–9 The photomicrograph of the histopathologic specimen in our subjects shows excessive endothelial proliferation with adjacent subacute and chronic hematoma and surrounding fibrous tissue margin. Histopathologic findings and clinical course in our subjects resemble those from other reports of hematomas of the maxillary sinus.10 We speculate that the same pathophysiologic mechanism may be responsible for the hematomas seen in conjunction with the entities described above. In our histopathologic specimens, there is no cholesterol cleft with reactive foreign-body giant cells seen in cholesterol granuloma. No mucous retention or infiltration of foamy histiocytes seen in the mucocele is observed. A hematoma is subepithelially located; thus, a hemorrhagic cyst is ruled out. We suggest that an organized maxillary sinus hematoma is different from these entities.
Conclusion
Benign hematoma of the sinus is a rare lesion of uncertain pathophysiology that may mimic a neoplasm. It is important to include this in the differential diagnosis of an expansile maxillary sinus mass containing a hemorrhagic product so that inappropriate surgery can be avoided.
Acknowledgments
We thank Dr Kenichi Wakasa for helpful comments on our article.
References
- Received July 30, 2006.
- Accepted after revision November 22, 2006.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.