
Abstract
BACKGROUND AND PURPOSE: “Gossypiboma” is a term used to describe a mass within the body that comprises a cotton matrix surrounded by a foreign-body reaction, which is extremely rare after spinal surgery. The purpose of this study was to describe the clinical and MR imaging features of gossypibomas in the paravertebral area of 7 patients.
MATERIALS AND METHODS: Between October 1999 and December 2005, 7 cases of paravertebral gossypibomas were confirmed pathologically at 2 institutions. The clinical features were reviewed retrospectively. We recorded MR imaging features and differential MR imaging–based diagnoses.
RESULTS: All patients were symptomatic; the most frequent symptom was nonspecific back or neck pain. None of the patients presented with signs of infection or required surgery urgently. In 3 of the 7 patients, gossypiboma was included in the preoperative differential imaging diagnosis. In all patients, the gossypiboma was located in the vicinity of the initial site of surgery. Typically, gossypibomas were visible in T2-weighted images as a mass with a hyperintense center and hypointense rim and exhibited strong peripheral enhancement in contrast-enhanced images. Retained surgical gauze was removed surgically from 4 patients; in the remaining patients, the surgical specimens contained suture threads.
CONCLUSION: Gossypiboma should be included in the differential diagnosis of the paravertebral mass when a mass with a hyperintense center and peripheral hypointense rim on T2-weighted images and strong peripheral rim enhancement on contrast-enhanced T1-weighted MR images is seen in postoperative patients.
Overlooking a foreign body can sometimes occur despite extreme caution during surgery. A foreign body can trigger a granulomatous reaction and may result in the formation of a sizeable mass. “Gossypiboma” is a term used to describe a mass within the body that comprises a cotton matrix surrounded by a foreign-body reaction. The word is bilingually derived from Latin “gossypium” (cotton) and Kiswahili “boma” (place of concealment).1
Various reports in the literature have described the radiologic features of gossypibomas2,3; CT is the method of choice for evaluating them.3 Characteristic CT features include a spongiform pattern with gas bubbles or a heterogeneous low-attenuation mass with a thin high-attenuation capsule that exhibits marked enhancement in postcontrast CT images.
Although gossypibomas can be visualized readily by using standard radiographic and CT imaging because of the incorporation of radiopaque filaments into surgical sponges, the MR imaging features of gossypibomas are less well known.4 Here, we describe the MR imaging features of paravertebral gossypibomas following spinal surgery, which are relatively rare compared with gossypibomas due to abdominal surgery.2
Materials and Methods
Patient Selection and Clinical Data
Between October 1999 and December 2005, 7 cases of paravertebral gossypiboma were confirmed pathologically at 2 institutions. Computerized medical records and pathology reports associated with these cases were reviewed retrospectively. Among these cases, 5 patients had gossypibomas that were located in the lumbar posterior paravertebral area and 2 had gossypibomas in the cervical posterior paravertebral area. Two of 5 patients with lumbar lesions were referred to our institution from a local hospital for further treatment. We used the medical records of these patients to review several clinical features, including patient age and sex, initial diagnosis, the causative surgical procedure that resulted in surgical gauze or suture material remaining in the patient, the amount of time that elapsed between initial surgery and the presentation of symptoms of gossypiboma, tentative diagnosis, diagnostic methods, and radiologic findings.
MR Imaging Protocol and Findings
We performed all MR imaging with a 1.5T system after intravenous injection of contrast material. The MR imaging protocol included the collection of T1- and T2-weighted images as well as gadolinium-enhanced T1-weighted images in the axial and sagittal planes. MR imaging features were evaluated by 2 neuroradiologists who reached a consensus regarding the MR imaging features. The MR images were reviewed for the following characteristics: lesion size (greatest diameter) and location, lesion margin and shape, signal intensity, degree of contrast enhancement, and internal architecture. We correlated the MR imaging features with the results of a pathologic examination.
Results
Clinical Features
The patients who had paravertebral gossypiboma included 4 men and 3 women who ranged from 34 to 86 years of age (average, 52 years of age). In all patients, the causative surgical procedure was laminectomy with or without diskectomy due to a herniated disk. The amount of time that elapsed between the initial surgery and the presentation of symptoms of gossypiboma ranged from 4 months to 16 years. All patients were symptomatic at initial clinical presentation. Five patients with lumbar paravertebral gossypibomas presented with lower back pain that originated at the site of the lesion. Two patients with cervical paravertebral gossypibomas presented with nonspecific neck pain. None of the patients presented with symptoms of infection such as fever or local tenderness. None of the patients required urgent surgical intervention to remove the paravertebral mass. The amount of time that elapsed between symptom onset and MR imaging examination ranged from 2 weeks to 4 months. All gossypibomas were removed surgically within 3 weeks of the MR imaging examination, and the clinical symptoms resolved after their removal. Table 1 lists the clinical and MR imaging features of the 7 patients with paravertebral gossypiboma.
Clinical characteristics of the 7 patients with paravertebral gossypiboma
MR Imaging Features
The average maximum diameter of the lesions was 4.3 cm (range, 3.5–5.0 cm). Lesions were located within the posterior paravertebral space in the vicinity of the site at which the initial causative surgery had been performed. All lesions were well circumscribed in all imaging planes except for 2 patients (patients 1 and 2). Each lesion was round or ovoid with a lobulated contour. In all patients, T1-weighted MR images revealed lesions with a low or intermediate signal intensity compared with the signal intensity of the paravertebral back muscles. In 6 of the 7 patients, T2-weighted images revealed a high signal intensity within the center of the lesion and a low signal intensity within the peripheral rim (Figs 1 and 2). Gadolinium-enhanced MR images revealed strong enhancement of the peripheral rim of the lesion (Figs 2 and 3). In 1 patient with gossypiboma containing suture threads (patient 6), the T2-weighted MR image revealed a paravertebral mass that had low-signal-intensity and multifocal high-signal-intensity spots, whereas the contrast-enhanced T1-weighted MR image revealed a mass with heterogeneous strong enhancement and did not show a central necrosis (Fig 4).

A 59-year-old woman (patient 1) who underwent partial laminectomy 8 months before the MR imaging examination. The CT scan (A) shows a lobulating contoured isoattenuated paravertebral mass with a slightly hyperattenuated center. The axial T1-weighted image (B) shows the paravertebral mass with an intermediate signal intensity. The axial T2-weighted image (C) shows the paravertebral mass with a high signal intensity in the center and a low signal intensity at the periphery. Initial radiologic differential diagnosis was abscess. The pathologic specimen (D) of the mass shows a surgical gauze (arrow) at the center of the mass.

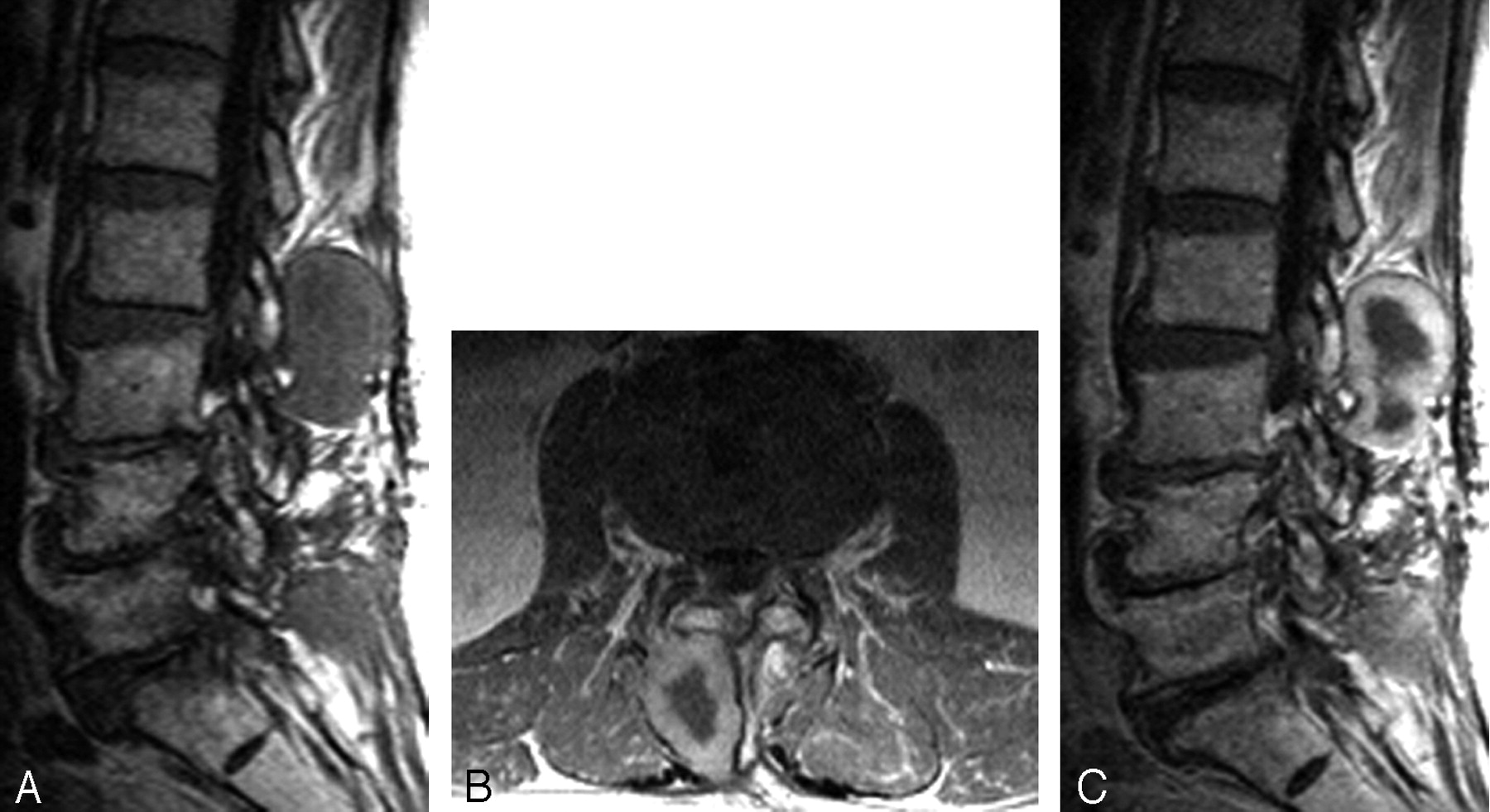
A 34-year-old man (patient 2) who underwent partial laminectomy and diskectomy 4 months before the MR imaging examination. Sagittal T2-weighted image (A) shows a paravertebral mass at the S1–2 level (arrow) with a high signal intensity in the center and a low signal intensity at the periphery. The axial T1-weighted image (B) with contrast enhancement shows bilateral posterior paravertebral masses with peripheral rim enhancement at the same location as in A. Initial radiologic differential diagnosis was abscess and gossypiboma. Small surgical gauzes were removed from the bilateral masses.

An 86-year-old man (patient 5) who underwent laminectomy and diskectomy 5 years before the MR imaging examination. Sagittal T1-weighted image (A) shows a posterior paravertebral mass with an intermediate signal intensity at the L2–3 level. Axial and sagittal T1-weighted images with contrast enhancement (B and C) show a right posterior paravertebral mass with peripheral rim enhancement. Initial radiologic differential diagnosis was abscess and gossypiboma. The mass was proved to contain a small surgical gauze surrounded by a thick fibrous capsule.

A 39-year-old man (patient 7) who underwent total laminectomy 7 years before the MR imaging examination. Sagittal T2-weighted image (A) shows a posterior paravertebral mass with low-signal-intensity and multifocal high-signal-intensity spots at the L4–5 level. Axial and sagittal T1-weighted images with contrast enhancement (B and C) show a mass with heterogeneous strong enhancement. Initial radiologic differential diagnosis was abscess, neurogenic tumor, and gossypiboma. Grossly, the mass did not contain a surgical gauze, but histopathologically, the cut surface of the mass contained suture threads surrounded by attenuated fibrosis related to the foreign body reaction.
In 3 of the 7 patients, gossypiboma was included in the differential imaging diagnosis preoperatively. In the other 4 patients, a definitive clinical diagnosis of gossypiboma was established intra- or postoperatively.
Pathology Findings
In 4 of the 7 patients, the retained surgical gauze was removed surgically (Fig 1D); in the remaining patients, suture threads were identified at the cut surface of the removed paravertebral mass.
Gross examination of the specimens revealed that the lesions were round or kidney-shaped and encapsulated. The external surface of each lesion was smooth and yellowish. Histopathologic examination of cross-sections of specimens revealed that each lesion contained surgical gauze around which a fibrous capsule had formed. The lesions contained a central necrotic area. The lesions that contained suture threads were associated with attenuated fibrosis around the suture threads. The mean maximal diameter of the mass was 4.5 cm in the surgical gauze group and 4.0 cm in the suture threads group.
Microscopic examination revealed that the lesions contained nonspecific suppurative inflammatory cells and foamy histiocytes surrounded by granulation tissue and fibrosis.
Discussion
A surgical sponge that is left accidentally in a surgical wound eventually develops into a textiloma.4,5 Strictly speaking the term “textiloma” should be reserved for a surgical sponge consisting of organic material. Currently, synthetic material has replaced cotton, so the definition “textiloma” must be adapted. “Gossypiboma” is a term that is used to describe a mass within the body that comprises a cotton matrix surrounded by a foreign-body reaction.6,7 The incidence of retained foreign bodies following surgery varies from 0.01% to 0.001%. Of these cases, 80% are gossypibomas, 75% of which are identified only after abdominal or pelvic surgery.2,3
The nonabsorbable materials of the retained surgical foreign bodies induce 2 types of reactions.8 One reaction is exudative in nature and leads to the formation of an abscess with or without secondary bacterial infection. A retained cotton matrix can lead very quickly, on the 1st day, to a local inflammation, which precludes a granulomatous reaction after approximately a week. If the retained material becomes infected, it may cause an abscess that can subsequently drain itself through a cutaneous fistula.2,3 Secondary infection of the cotton matrix mimics a nonspecific inflammatory reaction. The differential diagnosis in such cases includes postoperative collection, hematoma, and non-foreign body abscess. The other type of reaction is an aseptic fibrinous response, which creates adhesions and encapsulation and eventually results in the development of a foreign-body granuloma. Asymptomatic forms are sometimes discovered fortuitously. A delayed presentation may develop months or even years after the initial surgery. In this study, patients presented with symptoms of gossypiboma between 4 months and 16 years after the initial surgery. Adhesions and encapsulation are common features of gossypiboma, and the lesion may present as a mass. In such cases, the differential diagnosis typically includes tumor. The exudative type of gossypiboma causes symptoms earlier than the fibrinous type.8 Gossypibomas typically have an inconsistent radiologic appearance, which depends on the amount of time that the foreign body has been in situ, the type of material, and the anatomic location. Diagnosis of gossypiboma is difficult because patients with gossypiboma range from being asymptomatic to presenting with severe life-threatening illness.
In most countries, surgical sponges contain radiopaque material that facilitates detection by standard abdominal radiography. Such sponges can also be identified readily in CT images. However, surgical sponges without radiopaque markers are still used in many institutions,9 and this type of sponge is very difficult to identify by using standard radiographic and CT imaging. Therefore, retained surgical foreign bodies often make diagnosis intractable. On CT scans, abdominal gossypibomas appear as circumscribed masses with thick walls; these masses might contain gas bubbles and may exhibit calcification or enhancement of the wall after administration of contrast medium.10 The internal structure may appear to be whirl-like or spongiform because of the presence of gas trapped within the mesh of the sponge.11,12
In contrast, MR images can be difficult to interpret because radiopaque filaments cannot be visualized: The radiopaque filament is impregnated with barium sulfate, which is neither magnetic nor paramagnetic and therefore causes no artifacts on MR images. Furthermore, the filament contains very few free protons and, therefore, does not provide a strong MR signal intensity.6 Because radiopaque filaments are not visible in MR images, the differential diagnosis should include other postoperative changes such as scar formation and paraspinal abscess. If postoperative scarring occurs, these lesions usually exhibit moderate enhancement in contrast-enhanced T1-weighted images and generally exhibit a higher signal intensity in T2-weighted images.4,13 In our study, gossypiboma was diagnosed or included in the differential imaging diagnosis preoperatively in 3 of 7 patients; a definitive diagnosis of gossypiboma was established intra- or postoperatively in the remaining 4 cases.
There are few reports in which the MR imaging features of gossypiboma have been described, but these lesions appear to have a variable MR signal intensity that depends on the amount of fluid and protein associated with the lesion. Previous studies in which MR imaging was used to examine gossypibomas indicated that T1-weighted images typically reveal a well-circumscribed mass with a low signal intensity, whereas T2-weighted images reveal a very high signal intensity.3,4 The capsule is typically dark on T1- and T2-weighted images. Other previous studies reported that the presence of low-signal-intensity stripes suggesting gauze fiber on T2-weighted images may be a characteristic MR imaging appearance of gossypiboma.14,15 However, this imaging finding was not detected in our patients, and this difference is attributed to the nature of surgical gauze and the different foreign body reaction. Kuwashima et al16 reported that the signal intensity of the center of the gossypiboma varied on T1- and T2-weighted images. The mass with the center of high signal intensity on T1- and T2-weighted images had a surgical sponge that was rich in serosanguineous fluid with a high protein concentration, whereas the mass with the center of low signal intensity on T1- and T2-weighted images was mainly composed of organized cotton matrix with little fluid.16
In the present study, T1-weighted MR images revealed lesions with a low or intermediate signal intensity compared with that of the paravertebral back muscles. The lesions in T2-weighted images had a high-signal-intensity central core and a low-signal-intensity periphery that was indicative of granulation tissue and fibrosis. These MR imaging features are comparable with those in the previous studies.3,4 After intravenous injection of contrast material, the lesions exhibited a nonenhancing central core and strong enhancement of the peripheral rim in 6 patients. This enhancement pattern is comparable with the CT enhancement pattern reported previously.4,17 In 1 patient with gossypiboma containing suture threads, the contrast-enhanced MR image revealed a lesion with heterogeneous strong enhancement and did not show a nonenhancing central core. We did not identify gas bubbles within any of the lesions; therefore, gas bubbles may not be as prominent a feature of paravertebrally retained sponges as is the case for intra-abdominally retained sponges. When reviewed retrospectively, the characteristics of gossypibomas in MR images were sufficiently specific to enable a positive diagnosis.
Clinical symptoms associated with gossypiboma can be exhibited for several years or even for decades. The only remedy for clinical symptoms associated with gossypiboma is surgical removal of the mass. If the gossypiboma remains asymptomatic, the therapeutic approach must balance the potential risk of evolution of the foreign body and the risk of surgical removal. The clinical history can help to differentiate these 2 alternatives because the onset of complaints is usually much earlier in patients with postoperative scar formation compared with those with gossypiboma. However, although all patients presented with newly developed symptoms at the site of the mass, just because the gossypiboma is there does not necessarily mean that it is the cause of the patient's new symptoms. The careful clinical evaluation for the cause of the symptoms is needed.
Conclusion
Our clinical and MR imaging–based review of a series of 7 patients with paravertebral gossypiboma revealed that this type of lesion has some characteristic MR imaging features. Gossypiboma should be included in the differential diagnosis of the paravertebral mass when a mass with a hyperintense center and a peripheral hypointense rim on T2-weighted images and a strong peripheral rim enhancement on contrast-enhanced T1-weighted MR images is seen in postoperative patients.
References
- Received April 13, 2006.
- Accepted after revision June 18, 2006.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}