
Abstract
SUMMARY: We report 3 cases of vertebroplasty-induced intraspinal leakage of bone cement that were referred to us for management. Two patients received decompressive surgery, and one received rehabilitation. The gross surgical finding of yellowish dura mater and intradural fibrosis, adhesion, and microscopic finding of arachnoid membrane fibrosis are suggestive of late effect of thermal injury. These patients had residual lower extremity weakness and urinary and stool problems 13 months, 3 years, and 4.75 years postvertebroplasty, respectively.
Vertebral fractures are the most common complications of osteoporosis. These fractures result in significant mortality and morbidity, the latter of which includes prolonged and intractable pain.
Percutaneous vertebroplasty, a therapeutic procedure for filling the collapsed vertebral body with polymethylmethacrylate (PMMA) percutaneously, provides pain relief. This technique was first described by Galibert et al for the treatment of a case of hemangioma at the level of C2.1 Indications now extend to other tumors and to osteoporotic vertebral fractures.2–4 In general terms, percutaneous vertebroplasty is simple and safe if performed under continuing fluoroscopic control and with technical precautions; however, serious complications such as pulmonary emboli and paraplegia may occur if bone cement leaks into the pulmonary artery or spinal canal.5, 6
This report describes 3 cases of intraspinal leakage as a result of vertebroplasties performed at other hospitals and referred to us for further management. Two of our cases had delayed surgery and pathologic correlation.
Case Reports
Case 1.
A 54-year-old woman had back pain with acute deterioration. Conventional radiography of the spine showed compression fractures at T8, T10, and L1 vertebral bodies. MR of the lumbar spine 2 days before vertebroplasty showed no abnormal soft tissue or compression to the spinal cord up to T10. Percutaneous vertebroplasty was performed, and paralysis of both legs was observed after the procedure. Emergent CT scan revealed hyperattenuated bone cement in the anterior epidural space at all treated levels, with extension to the posterior epidural space from T7 to T8 level (Fig 1A, -B). Emergent laminectomy from T8 to T10 with removal of posterior epidural bone cement for decompression was performed for the T spine that afternoon. There was no clinical improvement and CT 5 days after the first decompression surgery showed large residual intraspinal bone cement at the T7 level with marked compression to the spinal cord. A second surgical decompression with laminectomy for the T6, T7, and L1 levels with removal of posterior epidural bone cement was performed on the same day. CT 4 days after the second decompression showed adequate removal of T7 epidural bone cement. MR imaging 5 days after the second decompression, however, showed bloody posterior spinal fluid collection with compression to the spinal cord. The woman was transferred to our hospital 49 days after vertebroplasty. On physical examination at admission, sensory loss was found to be present below the level of T6. Postural hypotension and urinary incontinence were observed, and anal tone was loose. Complete paralysis of both lower extremities with areflexia was observed. MR imaging 50 days after vertebroplasty showed the presence of residual low-signal-intensity bone cement inside bilateral anterior paracentral epidural space at T8, T9, T10, and L1 levels, and bilateral intervertebral foramina at T7/T8 and T8/T9. There was also bloody fluid collection in the posterior epidural space with spinal cord compression and edema of the spinal cord from the T6–T7 to the T11 levels (Fig 1C). The amount of posterior fluid collection was similar to the MR study 5 days after the second surgical decompression.

Case 1. A, Sagittal reconstructed CT scan performed same day as vertebroplasty shows postvertebroplasty appearance with hyperattenuated bone cement in T8, T10, and L1 vertebral bodies. Bone cement filled the anterior vertebral body, the posterior vertebral body, and the epidural space (arrows). The technical flaw in this case was allowing the bone cement to fill the posterior vertebral body and continue filling in the spinal canal.
B, Axial view at T7/T8 disk level performed same day as vertebroplasty shows bone cement in the epidural space (black arrows) and pulmonary arteries (white arrows).
C, T2-weighted MR imaging performed 50 days after vertebroplasty shows low-signal-intensity bone cement inside the anterior and posterior aspects of T8, T10, and L1 vertebral bodies (white arrows) and postlaminectomy appearance with bloody fluid collection (white arrowheads) causing posterior epidural compression to the spinal cord. There is high-signal- intensity change in the spinal cord on the T2-weighted images, because of compressive myelopathy or previous thermal injury. The posterior epidural compression and signal intensity change of the spinal cord are similar to the MR imaging performed 5 days after the second decompressive surgery. These changes were not present on MR imaging performed 2 days before vertebroplasty.
D, Fibrosis of arachnoid membrane (H&E stain).
Laminectomy for T11, T12, and L2, decompression of the previous laminectomy site of T8–10 and L2, and neurolysis from T8 to L2 were undertaken in our hospital 62 days after vertebroplasty. The spinal cord was pale at T8–10. The dura matter was yellow in color at T8–10, possibly from thermal injury as a result of vertebroplasty. A bone marrow biopsy revealed the presence of plasma cell myeloma, plasmacytic type (Lambda, IgA+). Microscopic examination of the removed arachnoid membrane revealed fibrosis (Fig 1D).
The third postvertebroplasty surgery alleviated her postural hypotension. On clinical follow-up 13 months after vertebroplasty, she remains paraplegic, with complete sensory loss in the lower extremities, and stool and urinary incontinence. Her multiple myeloma is under control. She is still receiving neurologic rehabilitation and hoping for recovery.
The history of this patient is somewhat complex. The patient could walk before vertebroplasty, paraplegia was found immediately after vertebroplasty, and the initial CT after vertebroplasty showed large epidural leak with severe spinal cord compression. Therefore, the initial cause of paraplegia and urinary and stool incontinence was epidural leak of bone cement. Although the surgeon performed decompression immediately on the same day, the decompression was not satisfactory. Furthermore, the second decompression surgery was complicated by posterior bloody fluid collection, which caused compression to the spinal cord. The third decompression surgery relieved the posterior compression and the positional hypotension and resulted in the final diagnosis of multiple myeloma.
On the basis of the imaging clue, the technical flaw in this case was allowing the bone cement to fill the posterior vertebral body and continued filling in the spinal canal.
Case 2.
A 79-year-old woman presented with a gait disturbance secondary to Parkinsonism. She experienced an osteoporotic vertebral fracture and received vertebroplasty at the L2 level with general anesthesia. Leak of bone cement along the needle tract into the epidural space and inside the dural sac was noted immediately. Therefore, immediate L1 and L2 laminectomy with removal of bone cement in the epidural space and inside the dural sac was performed. She was found to have bilateral lower extremity weakness after the operation.
Because of persistent lower extremity weakness, she sought help in our neurosurgical clinic 8 months after vertebroplasty. Conventional radiographs and MR imaging 8 months after vertebroplasty showed epidural and intradural leakage of bone cement (Fig 2). She received rehabilitation only in our hospital. At follow-up 3 years after the leakage, she still had weakness of both lower extremities and could not walk on her own. She had urinary incontinence and constipation.


Case 2. Lumbar spine plain films and MR imaging were taken 8 months after vertebroplasty.
A, AP view conventional radiograph of lumbar spine.
B, Lateral view conventional radiograph of lumbar spine.
C, Sagittal MR imaging.
D and E, Axial MR imaging.
There is hyperattenuated bone cement in L2 vertebral body and in the spinal canal (arrows) on the anteroposterior and lateral conventional radiographs (A and B). On the proton-weighted image (C) and T2-weighted image (D and E), bone cement is low in signal intensity. Bone cement is found inside the dural sac in C and D (arrow). Needle tract can be identified as a low-signal-intensity channel (arrows) in the vertebral body extending posteriorly to the epidural space (E). The technical flaw in this case was puncturing the epidural space with the needle allowing cement to extend posteriorly to the epidural space along the needle tract.
The surgeon agreed the epidural leak lead to the patient’s neurologic deficit after vertebroplasty. He also agreed that the technical flaw in this case was deviation of the needle, which broke the medial wall of the pedicle resulting in perforation of the dural sac by the needle. The needle tract could be identified on axial MR imaging (Fig 2E).
Case 3.
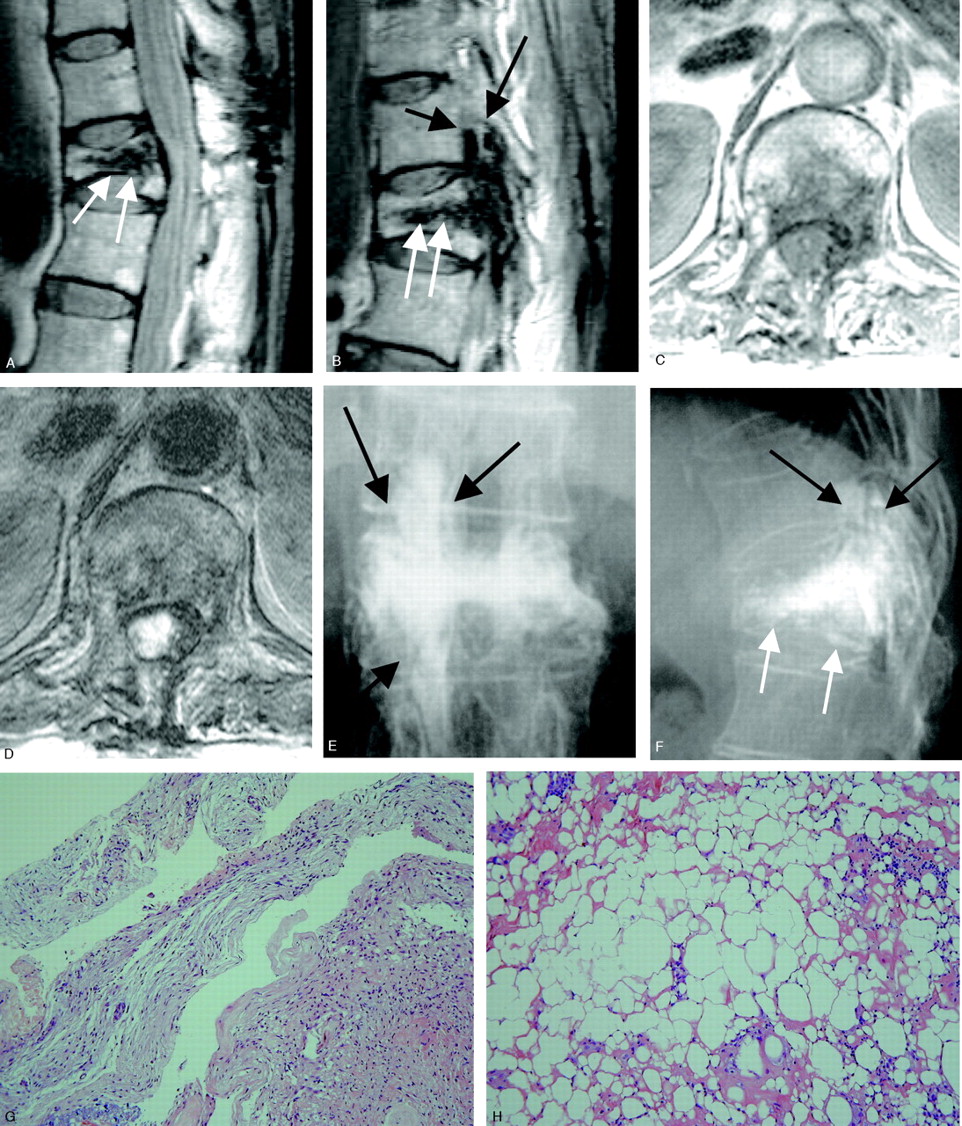
A 68-year-old woman was injured in a fall, and MR 11 months before vertebroplasty showed compression fracture with slight wedge deformity at the L1 vertebral body. The back pain became severe, and vertebroplasty for L1 was performed with general anesthesia. Leakage of bone cement along the needle tract into the epidural space was found during the procedure. Therefore, immediate right-side T12 and L1 laminectomy was performed to remove bone cement in epidural space for decompression. Numbness and paralysis of the left lower extremity, right leg weakness, and urinary and stool incontinence were observed after the vertebroplasty. At the request of the patient, a second surgical decompressive surgery was performed 30 days after vertebroplasty. Her condition did not improve, and she was referred to our hospital. MR imaging 73 days after vertebroplasty showed residual bone cement in the epidural space and intervertebral foramen of T12/L1 and L1/L2 (Fig 3). On physical examination, sensory loss was apparent at L2, with weakness of the left leg. An electromyogram revealed a lesion at the level of the cauda equina, severe and almost complete on the left side at L2–5 and S1–4, and severe but incomplete on the right L2–5 and S1–4. Detrusor areflexia was present, but with normal compliance. The anal tone was normal. Laminectomy with removal of spinous process for T11-L1 levels and neurolysis were performed 88 days after vertebroplasty. During surgery, 2 free pieces of bone cement were found compressing the spinal cord over the L1–2 level. A larger amount of whitish bone cement was located in the epidural space of T12–L2 and the foramen of T12/L1 and L1/L2 bilaterally. On pathologic examination, the arachnid membrane showed fibrosis and thickening (Fig 3G) and the epidural soft tissue showed fat necrosis and focal chronic inflammation cell infiltration (Fig 3H). On follow-up 4.75 years after percutaneous vertebroplasty, she still depends on a Foley catheter and is bedridden with stool incontinence. Her left leg can move, but not against gravity. Her right leg cannot move at all. Her son is seeking recovery from these problems, but this seems hopeless within the constraints of current medical practice.

Case 3. MR imaging taken 73 days after vertebroplasty (A–D) and conventional radiographs of lumbar spine (E and F) taken 86 days after vertebroplasty. Dense bone cement is found in the anterior and posterior aspects of the vertebral body (white arrows), epidural space (short arrow), and intervertebral foramen (arrows). The technical flaw of this vertebroplasty was use of the wrong needle and possibly drilling past the epidural space.
G, Arachnoid membrane shows active fibrosis and thickening (H&E stain).
H, Epidural soft tissue shows fat necrosis and focal chronic inflammatory cell infiltration (H&E stain).
The patient experienced no lower leg weakness before vertebroplasty. Laminectomy was performed immediately following vertebroplasty because of an intraspinal leak. Lower leg weakness was found after these procedures. The chief operator agrees that this patient’s new neurologic deficits appearing after vertebroplasty were caused by an intraspinal leak of bone cement.
This was an early case of a neurosurgeon with inadequate materials and an immature technique. He drilled a passage in the pedicle leading to the vertebral body. He then placed a Teflon needle inside the passage for injection of bone cement. Leakage of bone cement along the needle was found during the procedure. The surgeon agrees that it is possible that the needle entered the epidural space during the drilling process.
Discussion
Complications of percutaneous vertebroplasty include rib fractures, passage of PMMA to unwanted locations, and spinal cord compression from retropulsed bony fragments or tumors. In patients with severe osteoporosis, rib fractures may occur as a result of the prone position, and pressure to the chest wall that are required for this procedure.2, 4 PMMA may be passed to several unwanted locations, including the lumbar venous plexus, pulmonary artery, disk space, epidural space in the spinal canal, intervertebral foramina, and paravertebral region. A small amount of leak to the disk space is not usually harmful. A paravertebral leak or leakage into the intervertebral foramen may lead to nerve compression, aggravation of back pain, generation of new back pain, or motor radiculopathy.8, 9
Epidural leaks may occur more commonly than expected. Most of these leaks are subclinical with no overt clinical symptoms or signs. Leaks usually go undetected unless a careful postprocedure CT is performed. Ryu et al10 reviewed their cases of percutaneous vertebroplasty and found leak of cement into the epidural space in 92 (26.5%) of 347 treated vertebrae in 64 (40.3%) of 159 patients as demonstrated by postoperative CT.
The most severe and unwanted complications of epidural leak are motor weakness of the lower extremities and urinary and stool disturbances. Epidural leak may occur along one of the following routes: the fracture line extending to the posterior wall of the vertebral body, the basivertebral foramina, the anterior internal venous plexus, and the needle tract.10 Epidural leakage may easily occur along the needle tract if the needle perforates the medial wall of the pedicle and passes through the spinal canal. Injection of bone cement with the needle tip in the posterior vertebral body was associated with a higher frequency of epidural leak than was an injection with the needle tip in the anterior vertebral body.10
A direct relationship between the amount of PMMA injected and the incidence of leakage was observed elsewhere.10 Complete filling of the osteoporotic vertebral body is not necessary to achieve relief of fracture pain. Harrington5 recommended using approximately 1.5 mL of cement to be injected through each pedicle at each vertebral level and advised that no attempt be made to completely fill the vertebral cancellous space radiographically. From our experience, the amount of bone cement to be injected is related to the capacity of the anterior vertebral body. For a vertebral body with avascular necrosis and a large cavity present inside that body, a larger amount of bone cement is necessary. It is of critical importance to inject no more cement than can be accommodated by the anterior vertebral body and to stop the injection whenever leakage into veins or the paravertebral region occurs or any flow of bone cement to the posterior part of the vertebral body is observed.
Intraspinal leak may take place on either unilateral or bilateral pedicular approach. Harrington5 speculated that attempts to perform vertebroplasty unilaterally through a single pedicle increase the risk of cement extrusion because of the excessive local pressure generated by such injection. Ryu et al’s study, however, found that epidural cement leakage occurred more often when PMMA was injected via the bipedicular approach than when the cement was injected via the unilateral approach (P > .05).10
Cement viscosity is an important factor. A pastelike consistency is preferred to a liquid mobile consistency. Bone cement of liquid mobile form may flow quickly along the venous tract or fracture line to an unwanted site such as the pulmonary artery or spinal canal.
A screw syringe compressor enables slow and steady injection of the cement. Some authors consider that the use of a screw syringe adds to the safety of percutaneous vertebroplasty,9 though Ryu et al’s study found the use of an injector increased epidural leakage (P = .045).10 Intermittent release of injection pressure may be necessary to avoid fast flow of the bone cement to an undesirable site along the venous, needle, or fracture tract. Antecedent venography does not significantly improve the effectiveness or safety of percutaneous vertebroplasty if the vertebroplasty is performed by qualified, experienced operators.11 According to previous reports,1, 2, 4, 5, 12 standard barium-impregnated PMMA is often not sufficiently radiopaque to be adequately and safely visualized fluoroscopically during injection. Therefore, addition to the PMMA of sterile tantalum, tungsten, or barium sulfate, each of which increases visibility of the cement fluoroscopically, is necessary to enhance the safety of percutaneous vertebroplasty.
Some authors13, 14 believe that performance of vertebroplasty at approximately 3–4 weeks after a fracture increases the safety of the procedure. The intervening interval is thought to allow consolidation of the fractured posterior elements and clotting of the venous plexus such that the risks of leakage related to the introduction of the relatively liquid cement are decreased. This hypothesis needs further verification.
We propose that the following factors should increase the safety of vertebroplasty: (1) adequate opacification of bone cement; (2) efforts to prevent the needle from breaking the medial wall of the pedicle or passing through the spinal canal as it is advanced into the vertebral body; (3) constant monitoring of the injection of bone cement by using high-resolution biplanar fluoroscopy; (4) immediate cessation of injection when the cement reaches the posterior one fourth of the vertebral body; (5) injection of bone cement with intermittent release of injection pressure.
Injection of bone cement with the patient under local, rather than general, anesthesia has been recommended for the treatment of severe osteoporosis with vertebral collapse.5 The rationale for this recommendation is that clinical detection of neurologic compromise during the procedure is more likely in the conscious patient.
The possible causes of neurologic deficit after intraspinal leak of bone cement include direct mass effect and thermal injury to the spinal cord or nerve root. A recent study with injection of bone cement in osteoporotic cadaveric vertebral bodies found the temperature in the center of bone cement ranged from 49°C to 112°C and dwell times at temperatures above 50°C ranged from 0 to 8 minutes.15 Therefore, there is a risk of thermal necrosis when the nerve tissue is in direct contact with the bone cement. The gross appearance of yellowish dura mater that was in direct contact with bone cement found during surgery was considered to be thermal effect by the surgeon who performed the operation in case 1. The surgical gross finding of intradural fibrosis and adhesion and microscopic findings of fibrosis in the arachnoid membrane (cases 1 and 3) should represent delayed effects of thermal injury due to vertebroplasty because there was no previous history of surgical opening of the dura. The microscopic findings of fat necrosis with chronic inflammation and fibrosis in the epidural region (case 3) may also represent a late thermal effect.
Immediate surgical decompression with removal of bone cement should be helpful in case of epidural leak to prevent or revert new onset neurologic deficits in lower extremities if their cause is direct mass effect. Surgical exploration for removal of bone cement in the anterior epidural space, intervertebral foramina, intradurally in the anterior aspect of the spinal cord, or mixed with nerve fibers in the quauda equina is difficult. Although intraspinal leakage was found and laminectomy for removal of bone cement was attempted immediately in cases 2 and 3, bone cement was still present in the spinal canal in later imaging studies.
Because the dwell times at temperatures above 50°C ranged from 0 to 8 minutes,15 the thermal injury takes place in a short time. None of our patients received immediate satisfactory removal of bone cement in the intervertebral foramina, epidural space, or inside the dural sac. Whether immediate satisfactory surgical removal of bone cement is helpful to prevent new onset neurologic deficit from occurring or persisting needs further observation and more evidence.
References
- Received December 22, 2004.
- Accepted after revision January 26, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Large intraspinal cement leak during multilevel cement-augmented screw fixation
- Pulmonary embolism with coexistent incidental pulmonary cement embolism post vertebroplasty
- Sacral bone cyst treatment resulting in paraplegia
- Use and evaluation of a semi-permeable mesh implant in vertebral augmentation for the treatment of painful osteoporotic vertebral compression fractures