
Saur and colleagues are to be congratulated on a well-written article that compared findings at unenhanced CT with those of diffusion weighted MR imaging (1). Saur et al use a high-contrast-resolution algorithm with a high tube current (ie, 480 mAs) and then photograph at 50/30 HU to produce good-quality CT scans. We have reviewed >900 CT scans from Canadian centers by using tPA and were surprised that some still use windows of 100/40 HU, which produce flat CT scans unsuitable for assessing the subtle changes of early ischemia; however, we believe that the authors may not have interpreted their baseline CT scans adequately.
The authors report that their sensitivity for early ischemic change is better for diffusion-weighted imaging than for unenhanced CT. They state that their results support the application of stroke MR imaging for the treatment of patients with acute stroke.
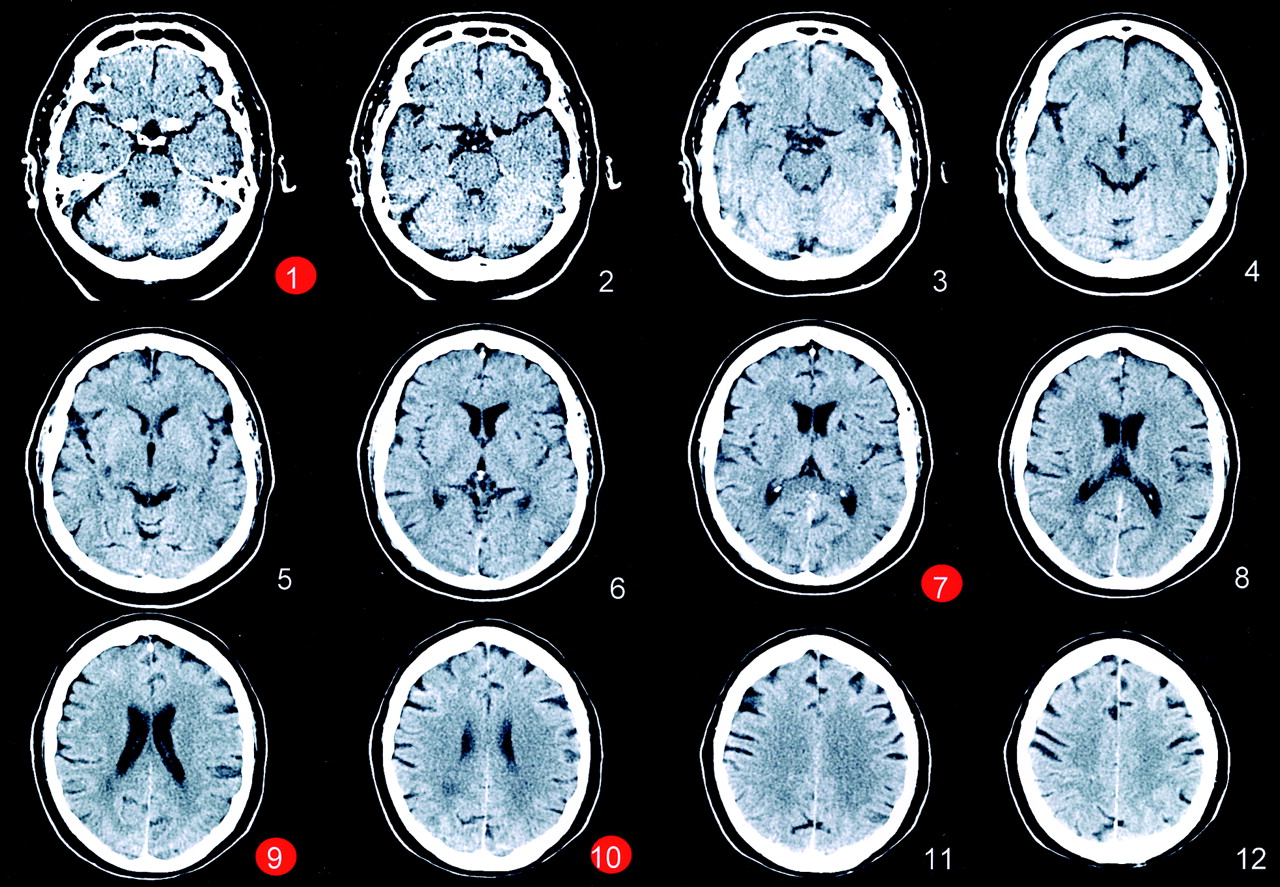
We note that the unenhanced CT shown in Figure 1 was rated as normal by five of the six raters. Amazed at this, a neuroradiologist (J.H.W.P.) showed, in turn, this unenhanced CT scan, while covering the rest of the figure, to four stroke neurologists (A.M.B., A.M.D., M.D.H., P.A.B.) and two stroke fellows (J.E.S., S.B.C.) in our department. They all independently stated that Figure 1 showed signs of ischemia. They saw in the left hemisphere (right side of CT scan) compared with the right the following:
A 3 scan: Blurring of cortical gray matter and white matter. Gray matter in the left cortex is not as hyperattenuated as that on the right side.
A 4 scan: Increased hypoattenuation seen defusely in white matter in the posterior half of the middle cerebral artery territory with cortical gray matter and white matter blurring. There is a smaller, more obvious, focal white old lesion in the posterior part of the right hemisphere.
In addition, some thought that in A2 there was patchy hypoattenuation in the insular ribbon, but we note that in both Figures 1 and 2 of Saur et al’s (1) article, the A2 scan is really too high to assess the insula and basal ganglia properly. The hyperattenuated MCA sign on the CT in Figure 2 (A1) is not mentioned.
We have previously used a semiquantitative scoring tool, ASPECTS (Alberta stroke program early CT score), and showed that it is more reliable than the middle cerebral one-third rule (2, 3). Careful assessment of the baseline CT scan provides invaluable information on the status of the tissue. Although we acknowledge that diffusion-weighted imaging is more sensitive than unenhanced CT in the diagnosis of acute middle cerebral artery stroke, this is only true for small lesions. For larger lesions, the CT scan predicts the diffusion-weighted findings in a linear fashion (4). CT remains the best method of rapidly assessing the brain in a disease where every 15-minute delay in the administration of thrombolysis can make the difference between an independent and dependent outcome.


CT scan of a 62-year-old patient with aphasia and right hemiparesis obtained 100 minutes after symptom onset. Five of six blinded raters judged the scans negative in a study comparing the sensitivity and interrater agreement of CT and diffusion findings in hyperacute stroke. In contrast, five readers found blurring of cortical gray/white matter on section 9 and increased hypoattenuation in white matter in the posterior part of the middle cerebral artery territory on section 10.
Only the red marked scans were included in the original article for illustration of a false-negative rating. The presentation of only a subset of all sections might have been misleading, because rating of early CT signs in the patients study as a whole may be judged as negative with a better approximation to reality.
Reply–Hyperacute Stroke: Experience Does Not Prevent Misinterpretation of Native CT Scans
We thank Dr. Pexman and colleagues for their interest in our study (1). They make the criticism that the CT scans in our article were not normal but showed discrete early signs of ischemia.
We very much appreciate their letter, because it demonstrates exactly the problem of early CT scans in acute stroke: disagreement among experts. What is the value of a test that produces as many false-negative ratings as early CT? What is the value of a test that is not reliable even in the hands of experts?
CT imaging is still the workhorse for the diagnosis of acute neurologic disease. Many cerebrovascular centers, however, have implemented MR imaging as the first-choice imaging technique in acute cerebral ischemia. One of the arguments for MR imaging is its multimodality, which provides information relative to tissue diffusion, perfusion and the vessel status by MR angiography. Multimodal stroke MR imaging therefore opens the opportunity to expand the narrow time window for thrombolysis (2) and prevents stroke mimics from unnecessary thrombolytic treatment.
Our CT scans were rated under real-life condition. The time for evaluation of each study was limited to 2–3 minutes. The rating was not performed by an expert panel, but by stroke residents who are involved in the decision-making process on a daily basis, especially at night. Our results are in line with a recent study by Fiebach et al, who found that “DWI has a substantially better sensitivity and accuracy than CT even if the raters have limited experience” (3).
The ASPECTS score is not widely used, and its advantage over the one-third rule was recently challenged (4). It seems rather euphemistic to state that “careful assessment of the baseline CT scan provides invaluable information on the status of the tissue.” It was only recently that we published work on the pathophysiological background of CT hypoattenuation, a neglected area of imaging research (5).
We agree that CT remains a good tool for the rapid assessment of the cerebrum; however, MR imaging does not necessarily delay the administration of thrombolytic drugs, and thrombolysis can be started as soon as diffusion-weighted imaging, a T2* sequence for the exclusion of hemorrhage and the vessel status, is assessed. MR imaging is the diagnostic tool of choice if additional information on vessel status and perfusion is required to expand the time window and diffusion-weighted imaging facilitates the recognition of early ischemia even for residents.
- Copyright © American Society of Neuroradiology








{kind=link}
{kind=link}