
Abstract
Summary: The MR imaging appearances in three cases of nasopharyngeal tuberculosis are reported, and the findings are combined with three additional cases from a review of the literature. Two patterns of nasopharyngeal tuberculosis were identified. The first pattern is a discrete polypoid mass in the adenoids, and the second pattern is a more diffuse soft-tissue thickening of one or two of the walls of the nasopharynx. Extension outside the confines of the nasopharynx was not a feature, except in one case with early involvement of the prevertebral muscles.
Nasopharyngeal tuberculosis is uncommon. It usually occurs in the presence of active pulmonary or systemic infection; the route of infection is via hematogenous or lymphatic spread. Primary nasopharyngeal tuberculosis is even rarer and is thought to result from direct infection of the upper respiratory tract. Nasopharyngeal tuberculosis is probably an under-diagnosed disease. Documentation of the cross-sectional appearances on MR images or CT scans is scanty and confined to case reports in the general (1–3) or radiologic literature (4).
Nasopharyngeal tuberculosis, especially the primary form, has a similar clinical presentation to that of nasopharyngeal carcinoma; both can present with cervical lymphadenopathy, nasal discharge, or nasal obstruction (5). Therefore, in the southern Chinese population, where the incidence of nasopharyngeal carcinoma is high, patients with tuberculosis may undergo intensive investigation of the nasopharynx for suspected malignancy. We report on three patients with proved primary mycobacterium tuberculosis of the nasopharynx who initially underwent MR imaging for suspected nasopharyngeal carcinoma. The MR imaging features of nasopharyngeal tuberculosis are described, and the literature is reviewed.
Case Reports
During the past 16 years, nasopharyngeal tuberculosis has been diagnosed in 36 patients at our institution. Three of these patients underwent MR imaging.
Case 1
A 63-year-old woman presented with right-sided cervical lymphadenopathy. She underwent flexible nasopharyngoscopy that revealed a large mass in the roof of the nasopharynx. MR imaging revealed a 2-cm polypoid mass in the nasopharynx, arising from the midline of the roof and upper posterior wall at the site of the adenoids. The mass was of intermediate T2 and T1 signal intensity with moderate contrast enhancement (Fig 1). Partial septations were just discernible. No extension was seen outside the confines of the nasopharynx. Small nonenlarged retropharyngeal nodes and multiple slightly enlarged nodes were seen in the posterior triangles and internal jugular chains. Ziehl-Neelson staining of a biopsy of the mass revealed granulomatous inflammation and acid-fast bacilli. No malignant cells were observed. Culture confirmed Mycobacterium tuberculosis. No evidence of active tuberculosis in the chest and no systemic tuberculosis were observed. The nasopharyngeal mass resolved on antituberculous therapy.

Images from the case of a 63-year-old woman who presented with right-sided cervical lymphadenopathy (case 1).
A, Axial contrast-enhanced T1-weighted image (505/12/2 [TR/TE/NEX]) of the nasopharynx shows a discrete moderately enhancing polypoid mass in the central roof and upper posterior wall at the site of the adenoids.
B, Coronal T2-weighted image (2500/100/3) shows a discrete polypoid mass of intermediate T2 signal intensity in the central roof/upper posterior wall at the site of the adenoids.
Case 2
A 29-year-old woman presented with bilateral cervical lymphadenopathy. She underwent flexible nasopharyngoscopy, which revealed a central swelling in the nasopharynx. MR imaging revealed a 1-cm polypoid mass in the nasopharynx arising from the midline of the roof and upper posterior wall at the site of the adenoids. The mass was of intermediate T2 and T1 signal intensity, with moderate contrast enhancement. It contained a 3-mm eccentric focus of high T2, low T1 signal intensity, in keeping with an area of necrosis (Fig 2). Partial septations were just discernible. No extension was seen outside the confines of the nasopharynx. Small nonenlarged retropharyngeal nodes and multiple necrotic nodes were seen in the posterior triangles and internal jugular chains. Ziehl-Neelson staining of a biopsy of the mass revealed granulomatous inflammation and acid-fast bacilli. No malignant cells were observed. No evidence of active pulmonary or systemic tuberculosis was observed. The patient’s symptoms resolved with antituberculous therapy.

Images from the case of a 29-year-old woman with bilateral cervical lymphadenopathy (case 2).
A, Axial contrast-enhanced T1-weighted image (499/12/2) of the nasopharynx shows a discrete moderately enhancing polypoid mass in the central roof and upper posterior wall, with a small focus of necrosis at the site of the adenoids.
B, Coronal contrast-enhanced T1-weighted image (425/13/2) shows a moderately enhancing polypoid mass in the central roof/upper posterior wall with a small focus of necrosis at the site of the adenoids.
Case 3
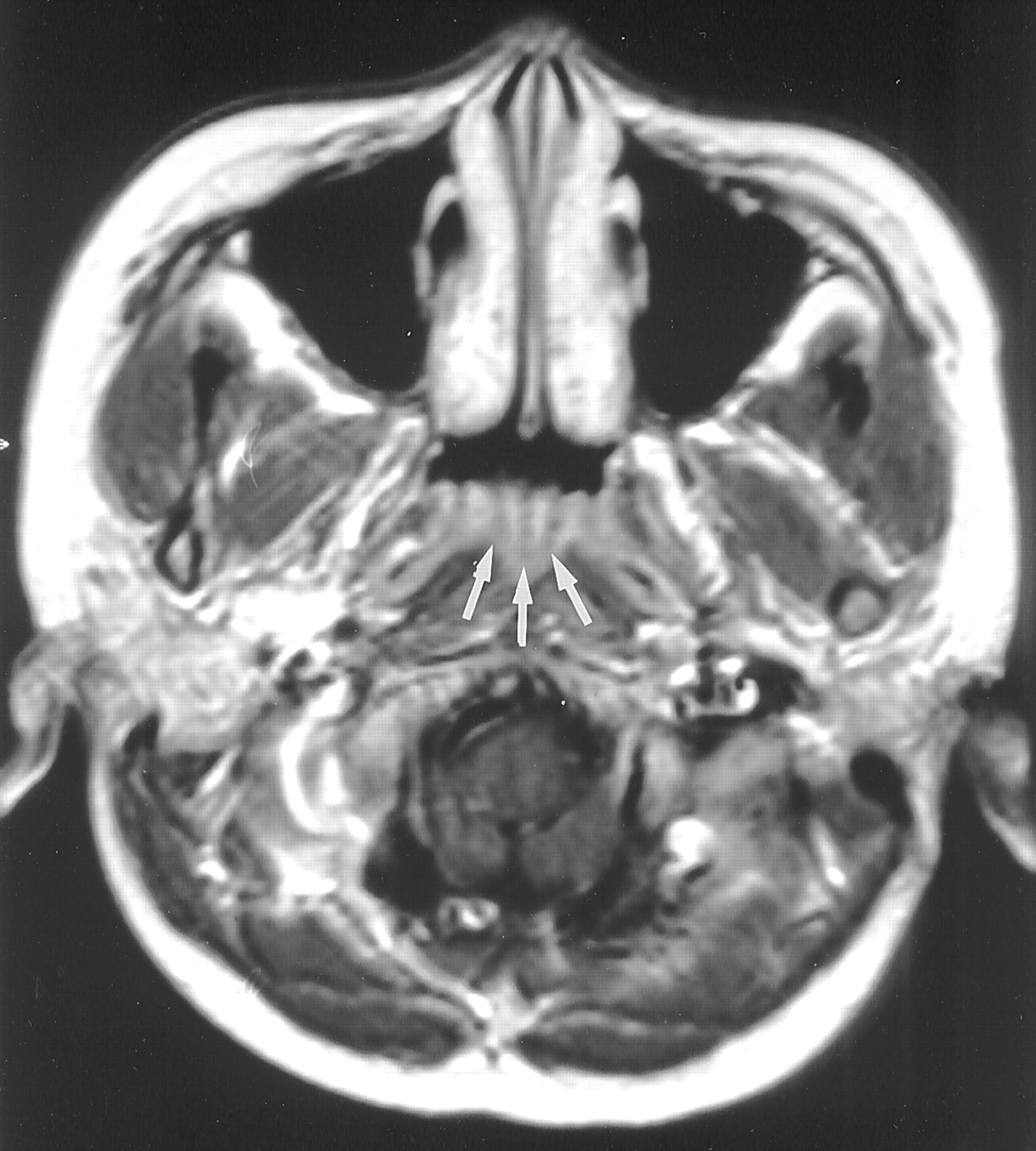
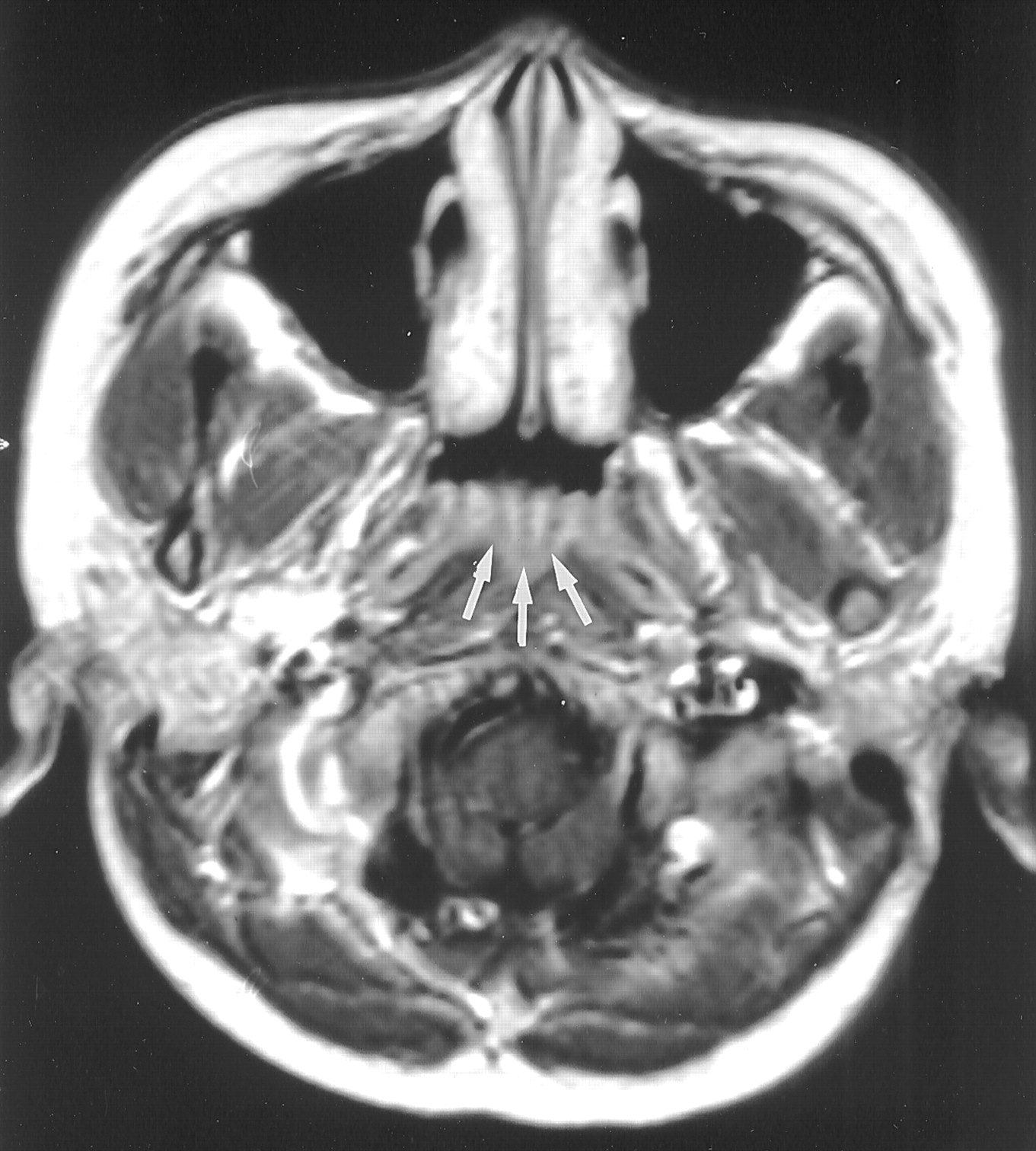
A 61-year-old man presented with postnasal drip. No cervical lymphadenopathy was present. He underwent flexible nasopharyngoscopy that revealed a mass in the left side of the roof of the nasopharynx. MR imaging revealed mild diffuse mucosal thickening in the left side of the roof that was of intermediate T2 and T1 signal intensity with moderate contrast enhancement (Fig 3). No extension was seen outside the confines of the nasopharynx. No lymphadenopathy was observed. The biopsy, performed 2 weeks before the MR imaging, revealed granulomatous inflammation and acid-fast bacilli with Ziehl-Neelson staining. No malignant cells were observed. No evidence of active tuberculosis in the chest and no systemic tuberculosis were observed.

Image from the case of a 61-year-old man with postnasal drip (case 3). Axial contrast-enhanced T1-weighted image (506/12/2) of the nasopharynx shows mild diffuse mucosal thickening in the left side of the roof of the nasopharynx (arrows).
Literature Review
The literature was reviewed, and the MR imaging features of nasopharyngeal tuberculosis were documented. Reports, including a description of the radiologic findings and an MR image, were included in the review. The results are presented in the Table
Literature review of the imaging features of nasopharyngeal tuberculosis
Discussion
Before the advent of anti-tuberculous therapy, tuberculosis of the nasopharynx was not an uncommon disease (6, 7). Since the widespread use of anti-tuberculous therapy, nasopharyngeal tuberculosis became rare. A study by Rohwedder (8) found involvement of the nasopharynx in only 0.1% of patients with active pulmonary tuberculous. Primary nasopharyngeal tuberculosis is thought to be even rarer (5), and most of the literature is limited to single case reports. However, the nasopharynx is a relatively silent region and the disease may be more common than suspected (5, 9), especially in endemic areas and with the increase in HIV.
The diagnosis of nasopharyngeal tuberculosis is made on the basis of pathologic and microbiologic findings of a biopsy sample. Pathologic examination reveals granulomatous inflammation with epithelioid giant cells and caseous necrosis. Acid-fast bacilli can be found, and the culture isolates the M. tuberculosis and confirms drug sensitivity. However, although a granulomatous reaction is frequently found, the isolation of acid-fast bacilli and the culture of M. tuberculosis can be extremely difficult. This problem is highlighted in two case reports in which M. tuberculosis was isolated only after the second (3) and third (1) nasopharyngeal biopsies. The elusive nature of the infection probably leads to the underdiagnosis of the disease. The clinical picture is further complicated in regions where both nasopharyngeal tuberculosis and nasopharyngeal carcinoma are found. Both diseases may have not only a similar clinical presentation but also a granulomatous inflammatory reaction. Nasopharyngeal carcinoma can develop a granulomatous reaction, similar to that of tuberculosis, in the tissue adjacent to the carcinoma, causing diagnostic confusion if a biopsy is obtained from peritumoral tissue. In addition, granulomatous inflammation with necrosis and ulceration can also occur as a reaction to radiation therapy, which is the primary treatment of nasopharyngeal carcinoma. This problem is compounded in that several case reports of simultaneous nasopharyngeal carcinoma and tuberculosis (10, 11) and of nasopharyngeal tuberculosis developing after radiation therapy for nasopharyngeal carcinoma (5, 12) have been published. The correct detection of nasopharyngeal tuberculosis in these cases can be hampered by the difficulty in isolating the M. tuberculosis.
Direct examination of the nasopharynx revealed three main patterns of involvement: 1) normal nasopharynx, 2) irregularity and ulceration of the mucosa, and 3) mass lesion that may cause bulging of the wall or a polypoid mass. The latter mass may arise at the site of the adenoids with the appearance of a mass or adenoidal hyperplasia.
Two of the cases reported herein showed discrete polypoid masses in the center of the roof and upper posterior wall of the nasopharynx, arising from the site of the adenoids. The adenoids are often identified in normal children and very young adults and have characteristic septations on T2-weighted images and especially on contrast-enhanced T1-weighted images (Fig 4). However, in adults, usually no lymphoid tissue or only tiny “tags” of residual tissue are discernible at this site on MR images. The presence of a mass at this site was therefore abnormal for the two adult patients in the present study. We presume that in those cases, tuberculosis involved the lymphoid tissue to cause not only enlargement but also destruction of normal lymphoid architecture. The signal intensity of polypoid tuberculous mass on T2-weighted images was intermediate and similar to that of gray matter. However, because normal lymphoid tissue has similar signal intensity, this signal intensity was not thought to be of value in distinguishing lymphoid hyperplasia from tuberculosis. Imaging did reveal that normal lymphoid septations were partially destroyed. This might be a valuable sign in distinguishing these two entities, although we are not aware of whether septations can invariably be identified in all patients with lymphoid hyperplasia. In the two patients with polypoid mass, the abnormality was confined to the nasopharynx with no extension into the adjacent tissues. A review of the literature revealed one additional case of a similar polypoid mass arising at the site of the adenoids, which was confined to the nasopharynx.
Axial contrast-enhanced T1-weighted image (500/15/2) of a nasopharynx shows the septations in normal lymphoid tissue (arrows).
The third patient showed a more diffuse mucosal thickening localized to the left side of the roof. Although the imaging was performed after the biopsy, the biopsy had been performed 2 weeks previously, so that by the time of the imaging, it is likely that post-biopsy changes had resolved. In addition, the distribution of the mucosal abnormality corresponded to that identified by endoscopy. Two additional cases in the literature also showed this second pattern of involvement, characterized by a more diffuse thickening in the nasopharyngeal mucosa on MR images, with one additional reported case that included CT scans (3). The diffuse form appears to cause asymmetrical involvement of the nasopharynx that usually is limited to one or two walls. Only one case of nasopharyngeal tuberculosis has revealed extension outside the walls of the nasopharynx, and this was mild, being limited to mild involvement of the longus capitis muscle. No case of nasopharyngeal tuberculosis has revealed deep extension into the parapharyngeal fat, nasal cavity, oropharynx, skull base, or cranium.
The differential diagnoses for nasopharyngeal tuberculosis on cross-sectional images depends on the pattern of disease. For patients with a polypoid mass in the region of the adenoids, the differential diagnosis includes lymphoid hyperplasia, nasopharyngeal carcinoma, lymphoma, and Castleman’s disease. Nasopharyngeal tuberculosis may not be distinguishable from these diagnoses on the basis of MR imaging appearance alone. However, in our experience, a polypoidal mass isolated to this region is not a very common finding in nasopharyngeal carcinoma. This, together with the absence of local soft-tissue extension, should alert the radiologist to the possibility of an alternative diagnosis of tuberculosis, especially if the biopsy reveals a granulomatous reaction. The second pattern of nasopharyngeal tuberculosis, with which more diffuse thickening of the nasopharyngeal wall occurs, has no imaging features to distinguish it from tumors such as early local stage nasopharyngeal carcinoma, minor salivary gland tumors, and lymphoma. The limited reports of Wegener’s granulomatosis in this region also describe a diffuse thickening along the wall of the nasopharynx. However, infiltration of the eustachian tube is usually present (13, 14) and was not found in this small series of nasopharyngeal tuberculosis. Infection such as syphilis, fungal infection, and leprosy may have an appearance similar to that of nasopharyngeal tuberculosis on direct examination of the nasopharynx and biopsy. To our knowledge, however, no cases are reported in the literature to confirm that they have similar features on images.
Conclusion
In this small series, the three case reports combined with a review of the literature revealed two patterns of nasopharyngeal tuberculosis on cross-sectional images. The first pattern is a polypoid mass of the adenoids. The second pattern is a diffuse thickening of the mucosal wall of the nasopharynx. In only one case in our report was extension outside the nasopharynx shown, and this was limited to a small area in the adjacent prevertebral muscle. In no case was deep invasion into the parapharyngeal fat, skull base, or cranium shown.
References
- Received March 4, 2002.
- Accepted after revision July 16, 2002.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}