
Abstract
Summary: The ectopic eruption of the teeth into the nasal cavity is a rare phenomenon. We report cases: two involving the nasal cavity and one involving the hard palate and complicated by Aspergillus rhinitis. We describe the clinical and radiologic presentation of these cases and discuss their etiology, complications, diagnosis, and treatment.
Nasal teeth are a rare form of supernumerary teeth (1). This article describes two cases of intranasal teeth and a case of an ectopic palatine tooth, all the result of ectopic eruption. CT scanning is helpful in making the diagnosis and planning treatment.
Case Reports
Case 1
An 8-year-old boy was referred to the otolaryngology clinic with left-sided nasal obstruction and an intranasal mass. Examination of the nose revealed a white mass surrounded by granulation tissue in the left nasal cavity. Necrotic debris was noted behind the mass. His intraoral dentition was normal. No previous history of maxillofacial trauma or surgery was elicited, and the patient’s general medical history was unremarkable.
The CT scan showed a smooth mass located in the floor of the left nasal cavity between the inferior turbinate and the nasal septum, with a homogeneous high attenuation equivalent to that of the teeth (Fig 1A). The mass was surrounded by soft tissue, consistent with the clinical finding of granulation tissue. A slit-like cavity along the long axis (Fig 1B) was appreciated within the mass with a bone window setting of a 600-HU window level (WL) and 4,000-HU window width (WW).
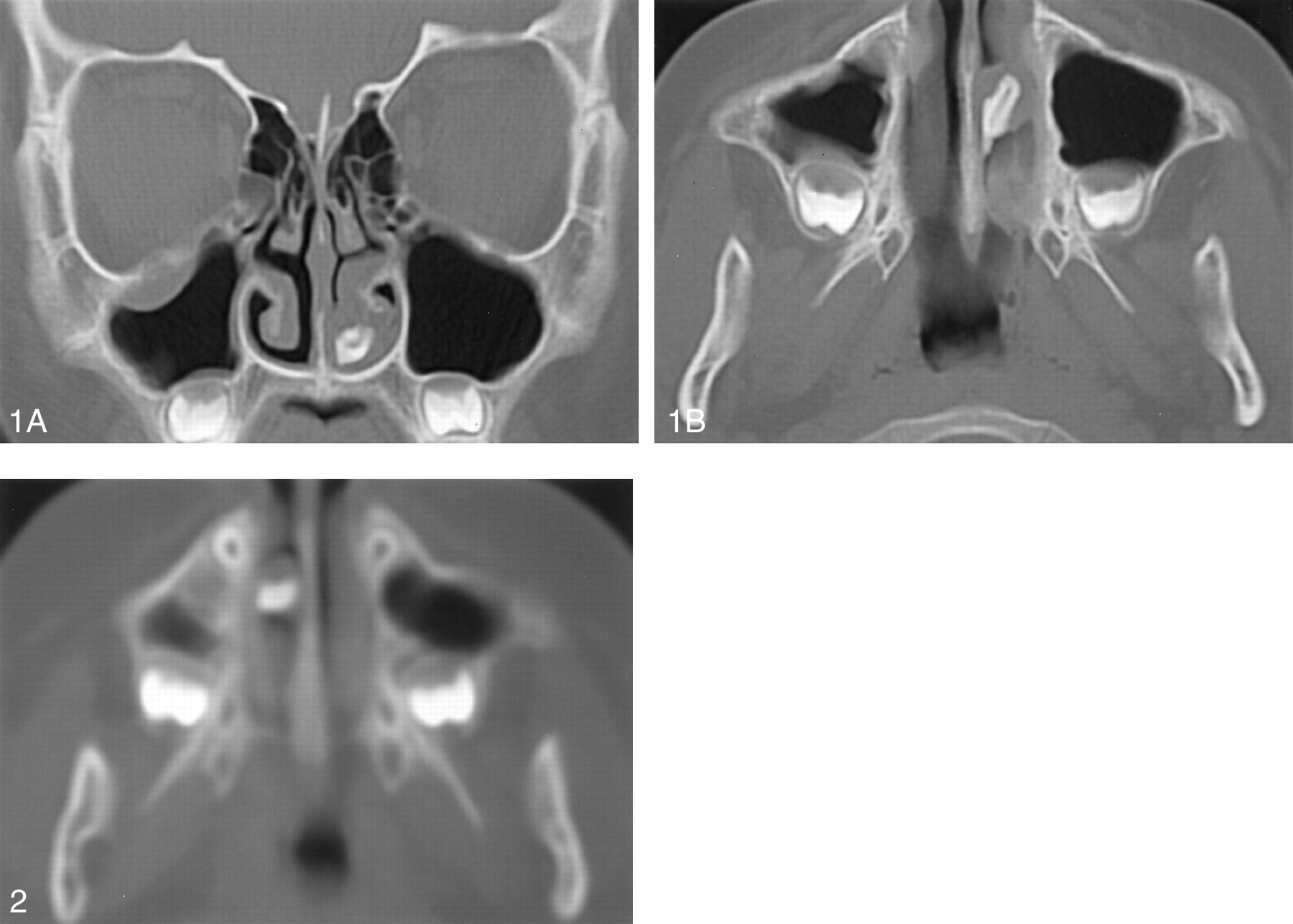
Case 1. CT scans in an 8-year-old boy with an ectopic tooth in the left nasal cavity.
A, Coronal scan obtained with a bone window setting of 600-HU WL and 4,000-HU WW reveals that the attenuation of the mass is the same as that of the oral teeth. The mass is separated from the underlying palatine process of the maxilla.
B, Axial scan obtained with the bone window setting shows the slit-like cavity well.
He underwent endoscopic removal of the nasal mass. Microscopically, the hard mass was a tooth composed of dentin and covered by a layer of poorly organized enamel. The central region of the tooth contained the pulp cavity. At follow-up in the outpatient clinic 2 weeks later, the patient was asymptomatic, and no nasal mucosal abnormalities were observed.
Case 2
A 7-year-old girl came to the outpatient clinic with a right-sided nasal obstruction associated with purulent discharge for 1 week. Intranasal examination revealed a white mass surrounded by granulation tissue in the floor of the right nasal cavity. Findings in the remainder of the head and neck examination were unremarkable.
The CT scan demonstrated a radiopaque mass located in the right nasal cavity between the inferior turbinate and the nasal septum (Fig 2). Soft tissue that surrounded the mass was consistent with the clinical finding of granulation tissue. The patient underwent endoscopic removal of the mass. Findings at histologic examination confirmed its dental nature. The symptoms of right nasal obstruction and purulent discharge completely resolved after surgery.

Case 2. Axial CT scan in a 7-year-old girl with an ectopic tooth in the right nasal cavity shows that the mass is surrounded by granulation tissue.
Case 3
A 59-year-old woman had a left nasal obstruction with a fetid odor for 2 years. Examination of the nose revealed a white, hard mass in the floor of left nasal cavity that was surrounded by black-yellowish greasy material. The patient had been edentulous for many years.
Radiography revealed a toothlike structure in the left nasal cavity (Fig 3A). CT scans demonstrated that the lesion had a shallow bony socket in the hard palate (Fig 3B). Irregular nodular and fine punctate radiopacities were appreciated posterior to the toothlike structure (Fig 3C). Because of the absence of any history of trauma or foreign body, the possibility of an ectopic tooth associated with fungal rhinitis was considered. Endoscopic surgery was performed to extract the toothlike structure and remove the black-yellowish greasy material. A tooth structure with an atypical crown was confirmed on histologic examination, and Aspergillus fungal hyphae were also observed. On follow-up examination 3 weeks later, the patient was symptom free.

Case 3. Images in a 59-year-old woman with an ectopic tooth on the left hard palate complicated by Aspergillus rhinitis.
A, Plain-film radiograph shows a radiopaque mass in the left nasal cavity.
B, Coronal CT scan shows that the lesion has tooth-equivalent attenuation and a shallow bony socket in the hard palate.
C, Axial CT scan reveals irregular nodular and fine punctate radiopacities posterior to the toothlike structure.
Discussion
The incidence of supernumerary teeth generally affects 0.1–1% of the population (1). The most common location is the upper incisor area, known as mesiodens. The extra teeth have an atypical crown, and they may be in a vertical, horizontal, or inverted position. They may grow and appear on the palate as extra teeth (case 3), or they may grow into the nasal cavity (cases 1 and 2). The teeth may be asymptomatic or cause a variety of signs and symptoms, including facial pain, nasal obstruction, headache, epistaxis, foul-smelling rhinorrhea, external nasal deformities, and nasolacrimal duct obstruction (2, 3). Complications of nasal teeth include rhinitis caseosa with septal perforation, aspergillosis (case 3), and naso-oral fistula (4).
Supernumerary teeth develop either from a third tooth bed that arises from the dental lamina near the permanent tooth bud or, possibly, from splitting of the permanent bud itself (1). Another theory is that their development is a reversion to the dentition of extinct primates, which had three pairs of incisors (1). Although the cause of ectopic growth is not well understood, it has been attributed to obstruction at the time of tooth eruption secondary to crowded dentition, persistent deciduous teeth, or exceptionally dense bone (5). Other proposed pathogenetic factors include a genetic predisposition; developmental disturbances, such as a cleft palate; rhinogenic or odontogenic infection; and displacement as a result of trauma or cysts (5).
The diagnosis of nasal teeth is made on the basis of clinical and radiographic findings. Clinically, an intranasal tooth may be seen as a white mass in the nasal cavity surrounded by granulation tissue and debris (2). Radiographically, the nasal teeth in our patients appeared as radiopaque lesions with the same attenuation as that of the oral teeth. With the bone window setting, the central radiolucency, which is correlated with the pulp cavity, may have a spot or slit, depending on the orientation of the teeth. The soft tissue surrounding the radiopaque lesion is consistent with granulation tissue found on clinical and pathologic examinations.
The differential diagnosis of nasal teeth includes radiopaque foreign body; rhinolith; inflammatory lesions due to syphilis, tuberculosis, or fungal infection with calcification; benign tumors, including hemangioma, osteoma, calcified polyps, enchondroma, and dermoid; and malignant tumors, such as chondrosarcoma and osteosarcoma. However, the CT findings of tooth-equivalent attenuation and a centrally located cavity are highly discriminating features that help to confirm the diagnosis.
Removal of nasal teeth is generally advocated to alleviate the symptoms and prevent complications. When an extra tooth is in the nasal cavity, the procedure is usually a minor operation. When a tooth has a bony socket in the floor of the nose, it may be extremely difficult to extract (6). CT is useful to evaluate the depth of the eruption site. The best time to remove the tooth is after the roots of the permanent teeth have completely formed, to avoid injury during their development (7).
Conclusion
Nasal teeth result from the ectopic eruption of supernumerary teeth and may cause a variety of symptoms and complications. Their clinical and radiologic presentation is so characteristic that their diagnosis is not difficult. CT scanning is helpful in planning their treatment.
- Received July 27, 2001.
- Accepted after revision September 24, 2001.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}