
Abstract
BACKGROUND AND PURPOSE: High-resolution T2-weighted fast spin-echo MR imaging provides excellent depiction of the cisternal and intracanalicular segments of the vestibulocochlear and facial nerves. Absence or reduction in caliber of the cochlear nerve (deficiency) has been described in association with congenital sensorineural hearing loss (SNHL). Depiction of cochlear nerve integrity may be important for diagnosis and management of SNHL.
METHODS: We retrospectively reviewed high-resolution T2-weighted fast spin-echo MR images of 22 patients examined for SNHL who had deficiency of the cochlear nerve. Images were evaluated for the presence and comparative size of the component nerves (facial, cochlear, superior vestibular, and inferior vestibular nerves), relative size of the internal auditory canal (IAC), and any associated inner ear abnormalities. The clinical history, results of the clinical examination, and audiometric findings were reviewed for each patient.
RESULTS: Deficiency of the cochlear nerve was observed in 12 patients with congenital SNHL and in 10 patients with acquired SNHL. Hypoplasia of the IAC was observed in association with congenital deficiency of the cochlear nerve in 11 of 12 patients. Deficiency of the cochlear nerve was observed in association with acoustic schwannoma in two cases and with acquired labyrinthine abnormalities in seven cases. Hypoplasia of the IAC was not observed in association with acquired SNHL.
CONCLUSION: Deficiency of the cochlear nerve can be shown by high-resolution T2-weighted fast spin-echo MR imaging. Deficiency may be observed in association with congenital or acquired SNHL and may be important in the assessment of patients for cochlear implantation. Hypoplasia of the IAC is an indicator of congenital cochlear nerve deficiency.
High-resolution T2-weighted fast spin-echo MR imaging provides excellent images of the cisternal and intracanalicular segments of the facial nerve and the three divisions of the vestibulocochlear nerve: the superior vestibular, inferior vestibular, and cochlear nerve (1, 2). These four nerves can be readily recognized in the distal or mid internal auditory canal (IAC) in normal patients by using oblique plane sagittal view imaging (Fig 1). At the lateral aspect of the IAC, the facial nerve lies in the anterosuperior portion, the cochlear nerve lies in the anteroinferior portion, and the superior and inferior vestibular nerves lie in the posterior portion of the canal. The site of separation of the vestibulocochlear nerve into its three components is variable, and division is complete only in the lateral aspect of the IAC (1, 2). The nervus intermedius is infrequently visualized as a small nerve adjacent to the facial nerve.

High-resolution T2-weighted fast spin-echo MR images provide excellent depiction of the cisternal and intracanalicular segments of the facial nerve and the three divisions of the vestibulocochlear nerve.
A, Axial view of the left cerebellopontine angle and IAC shows the normal anatomy. Parallel lines illustrate the plane prescribed for oblique plane sagittal images obtained perpendicular to the nerves of the IAC.
B, Oblique plane sagittal image obtained at the fundus of the IAC, oriented with anterior to the left and the cerebellum to the right. High-signal-intensity CSF delineates the four nerves of the IAC. In the anterior aspect of the canal, the facial nerve (Fn) lies superiorly, with the cochlear nerve (Cn) inferior to it. Superior (Vsn) and inferior (Vin) vestibular nerves lie posteriorly.
By using this knowledge of the anatomy and high- resolution MR imaging techniques, it is possible to determine which nerves are present and their relative size. In 90% of normal cases, the cochlear nerve is larger than either the superior or inferior vestibular nerve. The cochlear nerve is of similar size or larger than the facial nerve in 64% of cases (2). In addition, the relative size of the four nerves is symmetrical with the contralateral IAC in 70% of cases (2).
Detection of absence of the cochlear nerve or of reduction of its caliber (deficiency) with high-resolution MR imaging has been described in cases of congenital sensorineural hearing loss (SNHL) (3). Both congenital deficiency and acquired degeneration of the cochlear nerve have been shown pathologically in deaf patients (4–7). Acquired degeneration resulting in a deficient nerve had not been recognized radiologically before the introduction of high-resolution T2-weighted MR imaging. Additionally, a distinction between acquired degeneration resulting in a deficient nerve and the appearance of congenital neural deficiency has not been made. Because cochlear nerve size is thought to be correlated with spiral ganglion cell population, determination of the nerve caliber in cases of congenital or acquired SNHL may prove to be helpful in predicting the outcome of cochlear implantation (4). Our purpose was to show that absence or deficiency of the caliber of the cochlear nerve can be seen on high-resolution MR images, which may be important in the diagnosis and management of SNHL.
Methods
We reviewed the MR images of 22 patients who underwent high-resolution T2-weighted fast spin-echo MR imaging for congenital or acquired SNHL in whom the cochlear nerve was absent or decreased in its caliber. Each of these cases had been designated as having an absent or deficient cochlear nerve. All patients had undergone dedicated T2-weighted fast spin-echo MR imaging of the IAC in three planes on a 1.5-T imager with a superconducting magnet and a 3-in phased-array surface coil.
Axial 3D or 2D Imaging
3D T2-weighted fast spin-echo MR imaging was performed by using the following parameters: 4000/130/1 (TR/TE/NEX); echo train length, 64; matrix, 256 × 256; field of view, 13 cm. Data were zero-filled interpolated to produce a section thickness of 0.4 mm. The acquisition time was 8 minutes 1 second.
2D T2-weighted fast spin-echo MR imaging was performed by using the following parameters: 4000/102/6; echo train length, 32; matrix, 512 × 512; field of view, 20 × 10 cm; section thickness, 2 mm; section gap, 1 mm. The acquisition time was 9 minutes 50 seconds.
Eleven patients were studied with 3D T2-weighted fast spin-echo MR imaging and 11 with 2D T2-weighted fast spin-echo MR imaging. Coronal images, either as a reconstruction from the axially acquired 3D data set or as a direct coronal sequence by using parameters similar to those of the axial 2D sequence, were obtained. Oblique sagittal images were obtained through the IAC perpendicular to its axial plane, by using the following parameters: 4500/102/4; echo train length, 16; matrix, 256 × 256; field of view, 10 cm; thickness of contiguous sections, 2 mm. Acquisition time was 4 minutes 48 seconds. Intravenously administered contrast material was not used with any study.
The MR images were evaluated for the presence and relative size of the nerves in the IAC. We evaluated the nerves from the mid to lateral aspect of the IAC after separation of the three divisions of the vestibulocochlear nerve. In the sagittal plane, the caliber of the cochlear nerve was compared with the facial nerve, the superior and inferior vestibular nerves, and the contralateral cochlear nerve. We designated the cochlear nerve as small when it appeared decreased in size compared with the other nerves of the IAC. We designated the cochlear nerve as absent when it could not be identified on the axial, coronal, and oblique plane sagittal images.
The word deficiency was primarily used to indicate a smaller than expected cochlear nerve size, as compared with the other nerves of the IAC. The deficiency may have been due to either congenital hypoplasia of the nerve or acquired degeneration or atrophy. We designated the cochlear nerve as absent when it could not be identified on the axial, coronal, or oblique sagittal images. An extremely small nerve below the limits of spatial resolution of MR imaging would appear absent. Thus, in its broadest sense, the term deficient nerve can encompass all three situations: a small nerve, an imperceptible nerve, and one that is truly absent.
We evaluated the size and shape of the IAC and compared them with those of the contralateral side. The IAC was determined to be abnormal if it was <4 mm in either the vertical or transverse diameter, if it was irregularly shaped, or if it was appreciably asymmetrically small when compared with the contralateral side. The IAC has been previously well documented as virtually symmetric in healthy individuals, with a difference of <1 mm in 99% of patients and 1–2 mm in 1% (8).
The inner ear structures (cochlea, modiolus, vestibule, semicircular canals, and endolymphatic duct and sac) were evaluated for abnormalities in contour, size, and signal intensity. The clinical history was reviewed, with particular note being taken of the history and duration of SNHL, congenital anomalies or syndromes, family history of SNHL, other cranial nerve abnormalities, and audiometry findings.
Results
Of the 22 patients with cochlear deficiency, 10 had histories of acquired SNHL of known or unknown cause and 12 had identified congenital causes of SNHL. The clinical and imaging data are summarized in Tables 1 and 2. Of the 12 patients with congenital SNHL, six had unilateral absence of the cochlear nerve, four had bilateral absence of the cochlear nerve, and two had bilaterally decreased caliber of the cochlear nerve.
Clinical and imaging data of patients with congenital hearing loss
Clinical and imaging data of patients with acquired hearing loss
Marked reduction in caliber of the IAC ipsilateral to the deficient cochlear nerve was evident in 11 of the 12 patients (16 of 18 ears). One patient had small cochlear nerves bilaterally but a normal size IAC.
All 12 patients with congenital SNHL had ipsilateral abnormalities of the inner ear structures. Of the six patients with unilateral neural abnormalities, five had deficient modioli, one had an enlarged endolymphatic duct and sac, and one had a small vestibule (three patients had multiple abnormalities). Two patients had abnormal bone filling the small canal at the fundus of the IAC, through which the cochlear nerve passes to enter the cochlea. This is called the cochlear aperture, and the condition in which the aperture is absent is called an isolated cochlea (previously termed hypoplasia of the cochlear canal) (9) (Fig 2).
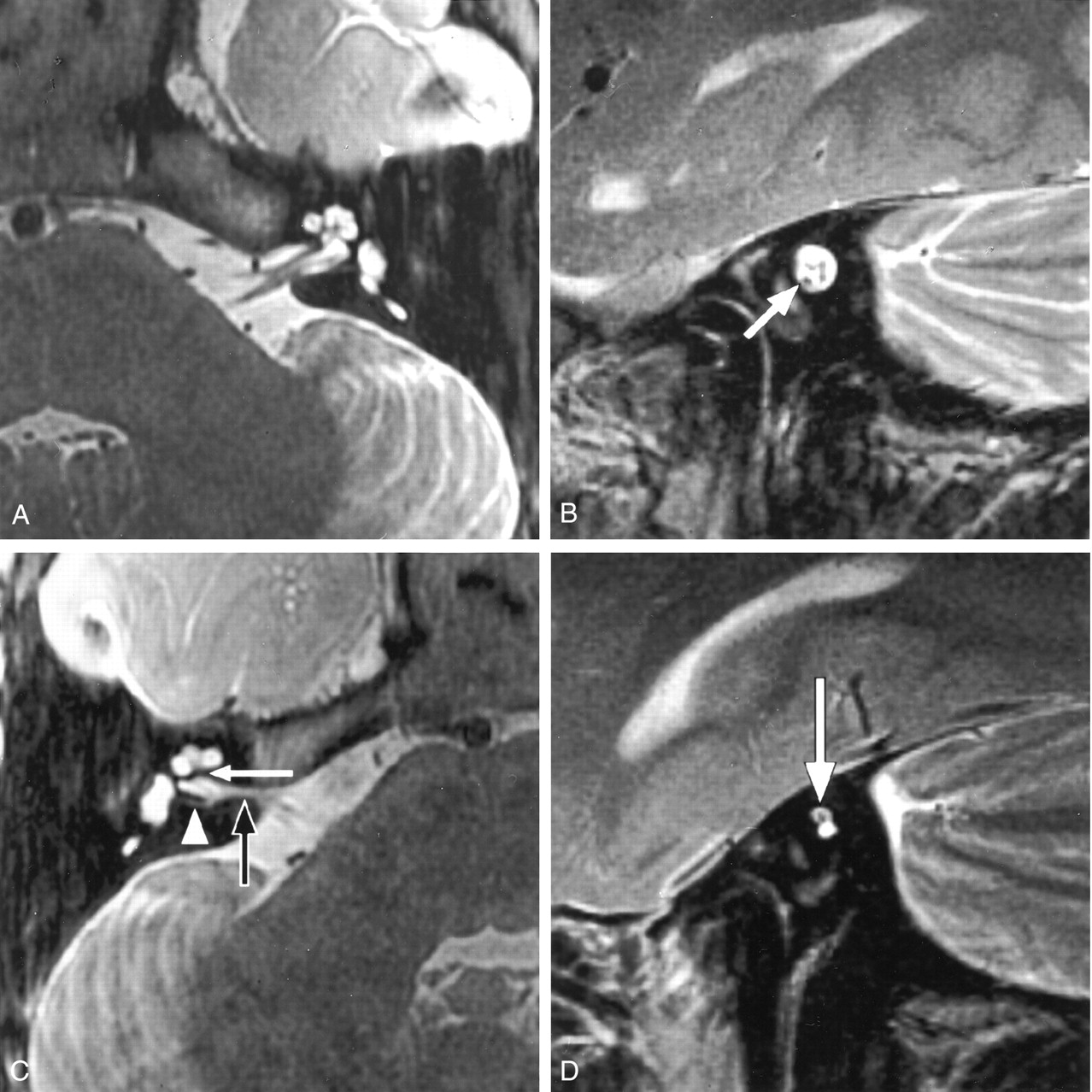
Congenital absence of the cochlear nerve with an isolated cochlea. Axial and oblique sagittal T2-weighted fast spin-echo MR images of a 5-year-old girl with profound unilateral hearing loss (patient C8).
A, Image of the normal left side shows the normal contours of the cochlea and other labyrinthine structures.
B, IAC is of normal size and contains four nerves of comparative size. Cochlear nerve lies anteroinferiorly (arrow).
C, Right side shows a deformed contour of the IAC (black arrow). Low-signal-intensity bar separates the fundus of the IAC from the modiolus (white arrow), which was confirmed to be bony at CT. We describe this as an isolated cochlea. The arrowhead indicates a singular canal containing the nerve of the posterior semicircular canal.
D, Oblique sagittal image of the distal IAC shows a solitary nerve within the superior aspect of the small, deformed canal (arrow). The cochlear nerve is absent in this patient with normal facial nerve function.
Of those patients with bilateral cochlear nerve abnormalities, four had bilateral vestibulocochlear dysplasia, one had bilaterally enlarged endolymphatic duct and sac, one had unilaterally enlarged endolymphatic duct and sac, and three had deficient modioli (three patients had multiple abnormalities). One patient had been diagnosed with complex congenital syndrome with somatic and craniofacial anomalies (CHARGE syndrome), and one had unspecified leukodystrophy.
Eleven patients had normal function of the facial nerves (House-Brackmann grade 1/6), confirming that a solitary nerve in the small IAC was the facial nerve. Patients C4 and C9 had unilateral facial nerve paralysis (House-Brackmann grade 6/6) (Table 1, Figs 2 and 3).

Bilateral cochlear nerve absence in a 7-year-old patient with severe dysplasia and bilateral absence of the cochlea (patient C10). Facial nerve function was preserved.
A, Axial T2-weighted fast spin-echo MR image of the left side shows dysplasia of the vestibule and semicircular canals (arrow). Cochlea was absent.
B, Oblique sagittal MR image obtained on the same side shows a small IAC containing only two nerves. The intact facial nerve lies anteriorly (arrowhead). We suspected that the posterior nerve was vestibular, on the basis of its position and the absence of cochlear structures (arrow).
Of the 10 patients with acquired SNHL, three had unilateral absence of the cochlear nerve and six had unilateral reduced caliber of the cochlear nerve. One patient had unilateral absence of the cochlear nerve with decreased caliber of the contralateral nerve. None of these patients with acquired SNHL and cochlear deficiency had a small IAC.
Two patients had ipsilateral acoustic schwannomas. Seven of the 10 patients had visible abnormalities of the labyrinthine structures ipsilateral to the cochlear nerve abnormality: Two had labyrinthitis ossificans, four had small modioli, and one had abnormal low signal intensity in the modiolus (presumed to be caused by previous hemorrhage or postinflammatory change). One patient with a long history of SNHL since the age of 5 years had no visible eighth cranial nerve but also no evidence of labyrinthine abnormality (Table 2, Figs 4–6).

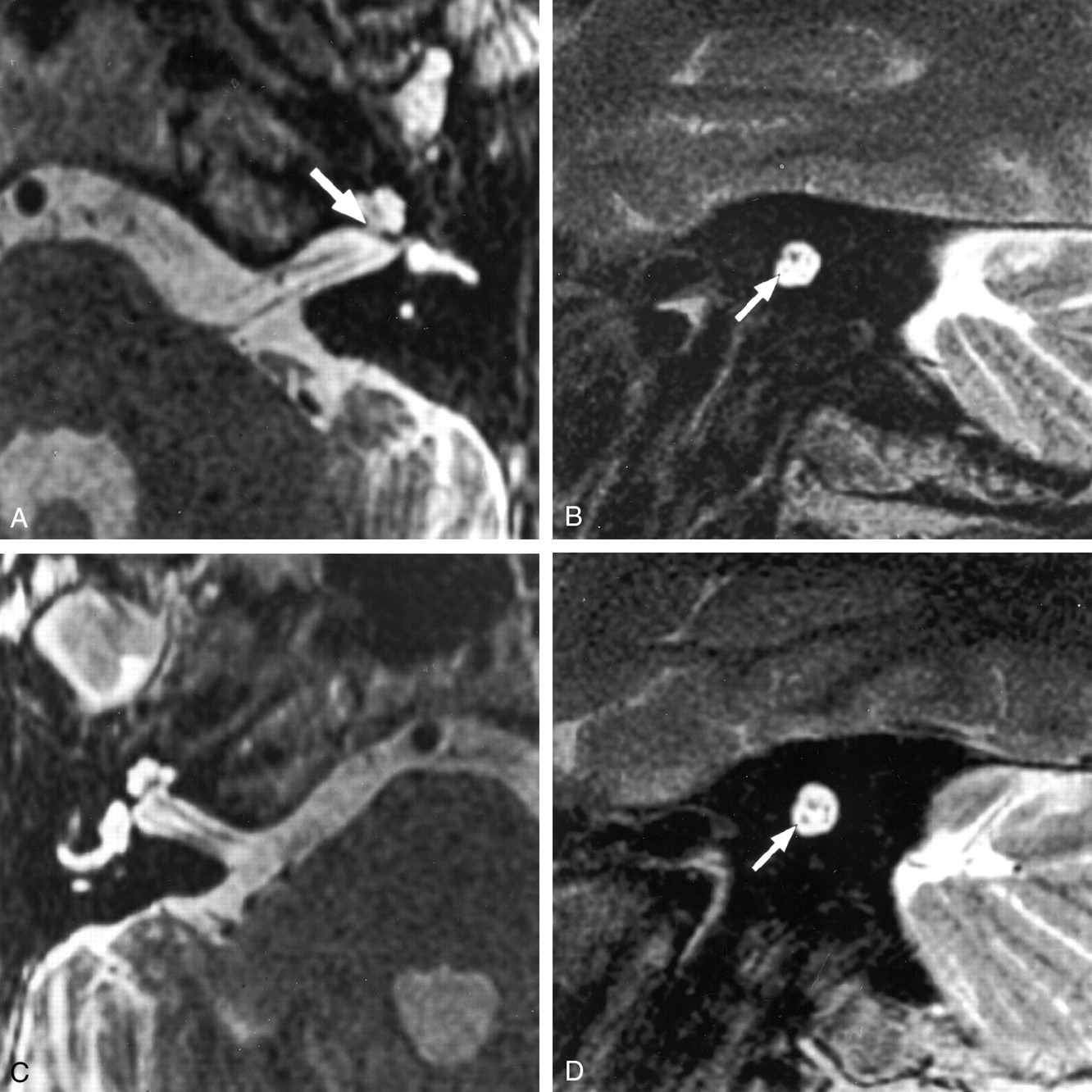
Deficient cochlear nerve in a 60-year-old patient with a 50-year history of left hearing loss after a motor vehicle accident (patient A10). This patient presented with a 3-month history of right-sided hearing loss.
A, Axial T2-weighted fast spin-echo MR image shows a small left modiolus (arrow) but no other structural cochlear abnormalities.
B, Corresponding oblique sagittal image shows a small caliber cochlear nerve (arrow) in a normal-sized IAC.
C, Axial T2-weighted fast spin-echo MR image of the right side shows no abnormality to explain the recent hearing loss.
D, Oblique sagittal T2-weighted fast spin-echo MR image of the right side also shows no abnormality to explain the recent hearing loss. A normal-caliber cochlear nerve is seen (arrow). Cochlear implantation was successfully performed on this side.

Acquired cochlear nerve deficiency in a 14-year-old patient with hearing loss after meningococcal meningitis at the age of 6 months (patient A3). Bilateral labyrinthitis ossificans was shown by CT (not shown).
A, Axial T2-weighted fast spin-echo MR image of the right side shows loss of the normal high-signal-intensity CSF in the labyrinth. The asterisk indicates the vestibule; arrow, arterior inferior cerebellar artery (AICA) loop.
B, Corresponding oblique sagittal image shows three nerves in the IAC. The cochlear nerve cannot be identified. Note the normal size of the IAC in this acquired cochlear nerve deficiency. Fn indicates the facial nerve; Vsn, superior vestibular nerve; and Vin, inferior vestibular nerve.

Acquired left-sided hearing loss of unknown etiology in patient A6. Axial high-resolution MR images showed a small left modiolus but no other labyrinthine abnormality (not shown). Cn indicates cochlear nerve; Fn indicates facial nerve; Vin, inferior vestibular nerve; and Vsn, superior vestibular nerve.
A, Right oblique sagittal T2-weighted fast spin-echo MR image clearly shows four normally sized nerves in the IAC.
B, On the affected left side, the cochlear nerve is not identified. Note the normal size of the IAC, which indicates an acquired abnormality after in utero formation of the canal.
Discussion
Previous studies have shown the IAC neural anatomy and inner ear structures with high-resolution T2-weighted MR imaging (1). Sagittal images obtained in the oblique plane perpendicular to the long axis of the IAC best distinguish each of the four major nerves of the IAC: facial, cochlear, superior vestibular, and inferior vestibular nerves (2). This imaging has allowed detection of a deficient cochlear nerve in some cases of congenital SNHL (3). The present study confirms that the cochlear nerve may be deficient in cases of congenital SNHL. In addition, the IAC caliber was reduced in all congenital cases in which the nerve was absent. This confirms suspicions of otologists that IAC hypoplasia may be due to absence of neural structures and hence a contraindication to cochlear implantation (10). Our study also shows that the cochlear nerve may also be deficient in cases of acquired SNHL. This is important because it suggests that secondary degeneration of the cochlear nerve may occur after injury.
Congenital Nerve Deficiency
When interpreting imaging findings associated with congenital SNHL, it is important to understand the embryology of the inner ear and IAC. Labyrinthine development commences at approximately 3 weeks’ gestation with the formation of the otic placode that will become the otic vesicle. At 7 weeks, the spiral organ of Corti develops from the cochlear duct, with fibers from the spiral ganglia forming the cochlear nerve. Simultaneous development of the ampulla with vestibular ganglia results in formation of the vestibular branches of the vestibulocochlear nerve (11).
At approximately 9 weeks’ gestation, the mesenchyme surrounding the otic vesicle begins to chondrify and will form the otic capsule that ossifies. The bony labyrinth is routinely identified on CT scans as hyperdense bone surrounding the inner ear structures. The IAC is formed by inhibition of cartilage formation at the medial aspect of the otic vesicle. This inhibition requires the presence of the vestibulocochlear nerve. In the absence of the nerve, a canal will not be formed (12). Not only does the presence of the vestibulocochlear nerve allow formation of the IAC, but survival and promotion of the nerve seems to require the presence of a growth factor from the otic vesicle (13).
The facial nerve develops independently of the vestibulocochlear nerve and becomes caught in otic vesicle cartilage formation (11). In the absence of the vestibulocochlear nerve, the IAC caliber becomes that of the facial nerve alone, which, in previous linear tomographic and CT studies, was defined as IAC aplasia (14–16).
Shelton et al (10) proposed that the aplastic IAC revealed by CT did not contain a cochlear nerve and was a contraindication to cochlear implantation. With high resolution MR imaging, it is possible to show that these patients indeed lack the cochlear nerve. We suggest that there may be variation in size of the IAC depending on the volume of nerve fibers traversing the canal and thus the volume producing an inhibitory substance to cartilage formation. That is, the absence of all components of the vestibulocochlear nerve produces an aplastic IAC (containing only the facial nerve) but absence of the cochlear nerve alone might produce an intermediate size IAC. In these cases, aggressive auditory testing, including cochlear promontory stimulation, should guide cochlear implant decisions.
One of our 12 cases of congenital neural deficiency did not have a small IAC. It is possible that an insult occurring after completion of formation of the IAC (either intrauterine or perinatal) may injure the cochlear nerve without effect on IAC size. These patients would be diagnosed as having congenital SNHL and possibly deficient nerve but normal IAC caliber. Conversely, we have not seen hypoplasia of the IAC with which a normal caliber cochlear nerve was evident.
Abnormality of inner ear structures may be subtle at MR imaging despite abnormality of the nerve caliber. The only inner ear abnormality observed in four of our cases was a deficient modiolus. Modiolar deficiency has been described with CT and MR imaging and probably represents a subtle form of cochlear dysplasia; it may occur in isolation or in association with other congenital inner ear abnormalities (17, 18). In the series presented by Casselman et al (3), the labyrinth appeared normal in two cases despite deficiency of the cochlear nerve and small IAC. In this situation, the cochlear abnormality may be microscopic or there may have been direct insult to the nerve before completion of IAC formation (approximately 5 months’ gestation).
Acquired Nerve Deficiency
Acquired cochlear nerve deficiency is a more complex entity to explain. A direct insult (either vascular, traumatic, compressive, or inflammatory) within the cerebellopontine angle or IAC might injure the cochlear nerve. Alternatively, cochlear nerve deficiency may result from degeneration of the nerve fibers in the IAC after cochlear injury.
Destruction of the cochlear neuroepithelium leads to retrograde destruction of the spiral ganglia in the modiolus (19, 20). Retrograde degeneration starts almost immediately after insult and rapidly leads to destruction of nerve fibers in the osseous spiral lamina. Months later, the spiral ganglion population will have reduced significantly. Insults such as mechanical destruction, acoustic trauma, anoxia, and ototoxic antibiotics result in a reduction in the neuronal population to 5–10%. Vascular impairment of the cochlea or direct neuronal infection produces almost 100% destruction of the neuronal population (20). Studies in humans show a near total loss of neurons when the deafness is due to trauma, meningitis, or bacterial labyrinthitis. Modiolar neuronal loss is less common in cases of viral labyrinthitis with which the endolymphatic epithelial structures are mainly affected and cochlear neurons are spared (20, 21). In comparison, neuronal degeneration in association with hereditary causes of deafness (eg, cochleosaccular degeneration) tends to be slower and more incomplete than in acquired causes of destruction of the organ of Corti. This neuronal degeneration also may vary considerably among syndromes (20).
Degeneration of the nerve fibers toward the brainstem is described as anterograde degeneration. Degeneration of the cochlear nerve after spiral ganglion destruction has been shown to occur after production of cochlear lesions in animals. After initial insult, fiber swelling occurs, then myelin sheath breakdown and fiber collapse. Continued loss of fibers and decreased cross-sectional area of the cochlear nerve are observed during longer survival times after the insult (22, 23).
Operative and autopsy studies in humans suggest that cochlear nerve degeneration is more unpredictable and has a more variable time course than in animals (5, 24, 25). The cochlear nerve in the IAC may appear relatively well preserved despite degeneration of most of the spiral ganglion cells (6). It is suggested, however, that severe pathologic changes of the axons revealed by electron microscopy would preclude proper functioning (7). In a small series of patients with deafness of varying duration and causes, Felix and Hoffmann (5) showed one patient with a 17-year history of congenital profound SNHL but a normal nerve fiber count and morphology revealed by electron microscopy. In the same study, noticeable atrophy of the cochlear nerve was also observed in four cases with variable causes and duration of SNHL.
The variability in cochlear neuronal destruction with different types of end-organ insults, as well as variability of extent and rate of secondary cochlear nerve degeneration and its manifestation, may explain why cochlear nerve deficiency is not a consistent MR imaging finding in deaf patients. Many of the patients who undergo imaging have no appreciable reduction in cochlear nerve caliber at MR imaging.
Because the cochlear nerve may have an appreciable reduction in fibers and still effectively transmit impulses to allow hearing (6), MR imaging depiction of a small nerve is only a relative contraindication to cochlear implantation. It does seem prudent to implant the more normal appearing inner ear and larger cochlear nerve until more is understood about these abnormalities. It has also been suggested that when nerve integrity is questioned, intracochlear electrical stimulation to determine the auditory nerve action potential and auditory brainstem response may be valuable tests to conduct before performing cochlear implantation (26).
A 1992 study (4) showed a correlation between nerve size and spiral ganglion cell population with significant decreases in both in a deaf population. It was suggested that cochlear nerve size might then be helpful for predicting the likely outcome of cochlear implantation. At that time, however, imaging was thought to be inadequate to depict abnormality of nerve size. Our current study suggests that identification of these abnormalities is now possible.
The absent cochlear nerve is the rare absolute contraindication with which there is no connection between the cochlea and brain stem nuclei. Care must be taken not to overinterpret an image as having an absent nerve when a small nerve is present. For this reason, complete clinical evaluation, including electrical stimulation (transtympanic stimulation of the promontory or intracochlear stimulation) is still important to select those patients who may benefit from implantation.
Conclusion
High-resolution T2-weighted fast spin-echo MR imaging can be used to depict deficiency of nerves in the IAC. Absence of the cochlear nerve may be observed in cases with congenital SNHL. This finding is associated with a hypoplastic IAC and is an absolute contraindication to cochlear implantation. Inner ear dysplasia or other cranial nerve abnormalities are often identified in these cases. The finding of an intermediate-size IAC with small or absent nerves should prompt careful auditory testing before cochlear implantation.
Acquired SNHL may also result in deficiency of the cochlear nerve. Acquired neural deficiency is not associated with a small IAC, and the finding of a normal size IAC with a deficient cochlear nerve suggests an acquired cause of SNHL. Determining the size of the vestibulocochlear nerve may prove to be of importance in predicting the likely success of cochlear implantation and determining the best side for implantation.
Footnotes
This work was presented in abstract form at the Annual Meeting of the American Society of Neuroradiology, San Diego, May 1999.
References
- Received May 9, 2001.
- Accepted after revision December 3, 2001.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Whether A Positive Response at approximately 4.5 ms in Auditory Brainstem Response Signifies Cochlear Nerve Deficiency in Infants?
- MRI Evaluation of the Normal and Abnormal Endolymphatic Duct in the Pediatric Population: A Comparison with High-Resolution CT
- Unilateral facial nerve hypoplasia without evident facial palsy
- Comparison of a Photon-Counting-Detector CT with an Energy-Integrating-Detector CT for Temporal Bone Imaging: A Cadaveric Study
- Evaluation of the Normal Cochlear Second Interscalar Ridge Angle and Depth on 3D T2-Weighted Images: A Tool for the Diagnosis of Scala Communis and Incomplete Partition Type II
- Vestibular Aqueduct Measurements in the 45{degrees} Oblique (Pöschl) Plane
- Mutations in apoptosis-inducing factor cause X-linked recessive auditory neuropathy spectrum disorder
- Pediatric Sensorineural Hearing Loss, Part 1: Practical Aspects for Neuroradiologists
- Brain Stem and Inner Ear Abnormalities in Children with Auditory Neuropathy Spectrum Disorder and Cochlear Nerve Deficiency
- Vertigo and Hearing Loss
- Complete Labyrinthine Aplasia: Clinical and Radiologic Findings with Review of the Literature