
Abstract
BACKGROUND AND PURPOSE: Tumors of the cranial nerve sheath constitute 5% to 10% of all intracranial neoplasms, yet few articles have described their CT and MR characteristics. We report the imaging findings in a relatively large series of schwannomas of the jugular foramen, contrasting them with other disease entities, especially vestibular schwannomas and tumors of the glomus jugulare.
METHODS: CT and/or MR studies of eight patients who underwent surgery for histologically proved schwannomas were reviewed retrospectively. One additional patient with an assumed schwannoma of the jugular foramen, who did not have surgery, was also included.
RESULTS: Surgical findings showed schwannomas of the glossopharyngeal nerve in seven patients and tumor involvement of both the glossopharyngeal and vagal nerves in one patient. All tumors were partially located within the jugular foramen. Growth extending within the temporal bone was typical. Tumor extended into the posterior cranial fossa in all nine patients and produced mass effect on the brain stem and/or cerebellum in seven patients; in five patients, tumor extended below the skull base. On unenhanced CT scans, tumors were isodense with brain in six patients and hypodense in two. In seven patients, CT scans with bone algorithm showed an enlarged jugular foramen with sharply rounded bone borders and a sclerotic rim. On MR images, T1 signal from tumor was low and T2 signal was high relative to white matter in all patients. Contrast enhancement on CT and/or MR studies was strong in eight patients and moderate in one.
CONCLUSION: Schwannoma of the jugular foramen is characteristically a sharply demarcated, contrast-enhancing tumor, typically centered on or based in an enlarged jugular foramen with sharply rounded bone borders and a sclerotic rim. Intraosseous extension may be marked.
Cranial nerve sheath tumors constitute 5% to 10% of all intracranial neoplasms. They most commonly arise from the vestibular portion of the eighth cranial nerve (1). A very large vestibular schwannoma may cause ninth cranial nerve palsy. Schwannomas of the jugular foramen, usually with origin from the ninth nerve, are rare, but the presenting symptoms may be similar to those of a vestibular schwannoma owing to mass effect by tumor growth in the posterior cranial fossa (2–4). About 130 patients with neurogenic tumors of the jugular foramen without associated neurofibromatosis have been reported. When the origin could be identified, almost all these tumors were histologically proved to be schwannomas of the glossopharyngeal nerve. Many of the published studies are case reports or small series, reported primarily in the surgical literature, without special attention to imaging characteristics (5–8). Few articles have described the CT and MR imaging appearance of these tumors (3, 9–11). In this series of nine patients, we emphasize the typical CT and MR imaging characteristics, including tumor location and growth pattern. Some clinical correlation is made, and differential diagnoses are discussed.
Methods
We retrospectively studied the imaging findings in nine patients (seven women and two men) with a diagnosis of schwannoma of the jugular foramen referred to our institution from 1984 to 1996. Patients with neurofibromatosis were not included. The patients were identified through a search of the files of the neurosurgery section and radiology department, but most were already known to us through our routine clinical work. The average age of the patients was 36 years (range, 19–63 years) at the time of diagnosis. All patients had imaging studies from referring institutions, and the imaging techniques varied, including the use of different types of MR and CT scanners.
MR images were available in six patients, and all included noncontrast T1- and T2-weighted sequences and contrast-enhanced T1-weighted sequences. CT scans without and with contrast enhancement were available in eight patients, and CT scans with bone algorithm were available in seven of these patients. In three patients, CT was the only imaging examination performed. All images were evaluated on two or more separate occasions by the first and third authors working together, and at least once more by the first and second authors working together. Agreement was reached by consensus, and there were no significant disagreements. The degree of enhancement that might be expected for a solid meningioma was considered strong enhancement, and significantly less enhancement was considered moderate. We did not feel comfortable using gradations of T1 or HU values, since many images were copies (sometimes of suboptimal quality) of studies from other institutions. The sizes and borders of the jugular foramina as well as the tumor growth patterns were noted.
Histologic findings were obtained from surgery in eight patients (five of the patients had been operated on previous to the current surgery), and the ninth patient (case 8) was treated with radiosurgery without prior biopsy. This patient was included because the imaging characteristics of the mass were similar to those seen in the other tumors and because a schwannoma of the jugular foramen was suspected on the basis of clinical evidence. Six patients had conventional angiography. Five of the nine patients have been the subjects of previous reports in the surgical literature, in which the surgical approach was emphasized (4).
Results
Unilateral hearing loss was the main presenting symptom in five patients at the time of initial diagnosis. Only two patients presented with true glossopharyngeal symptoms, such as dysphagia or reduced gag reflex. Other symptoms were seventh cranial nerve paralysis, dizziness, nystagmus, blurred vision, otalgia, vocal cord palsy, and tongue atrophy (see Table).
Clinical presentation and growth pattern in nine patients with schwannoma of the jugular foramen
Tumor Origin
At surgery, the tumor was thought to originate from the glossopharyngeal nerve in seven patients. In one patient the site of origin was either the glossopharyngeal or the vagal nerve, with both nerves surrounded by tumor. In patient 8, radiosurgery was performed without prior biopsy and the nerve origin was not identified. The histologic findings were consistent with schwannoma in all eight patients who had surgery.
Growth Pattern and Imaging Characteristics
MR images were available in six of nine patients and CT scans in eight of nine patients, with bone detail algorithm available in seven cases. The growth pattern and imaging characteristics are described in the Table and shown in Figures 1 through 3.

Case 5: 39-year-old woman with hearing loss.
A, Axial CT scan with bone algorithm shows an enlarged right jugular foramen (arrows). Note the sharp, rounded bone borders of the intraosseous extension, including a thin sclerotic rim and slightly bulging and eroded cortex (arrowheads).
B, Coronal contrast-enhanced T1-weighted MR image shows dumbbell-shaped tumor extending both into the posterior cranial fossa (arrows) and below the skull base (star).
C, Axial CT scan with bone algorithm shows a flared IAC meatus (arrow), which may be normal, although it is probably due in part to tumor eroding its posterior margin (compare with D).
D, Axial T2-weighted MR image shows a large tumor with high, slightly inhomogeneous signal in the posterior cranial fossa abutting but not extending into the right IAC (arrow). Note deformity of the brain stem, fourth ventricle, and cerebellum by the tumor.
In all patients, tumor was present within the jugular foramen (Figs 1–3). In eight of nine patients, the tumor extended from the foramen into the adjacent bone, occasionally to a marked degree. Intraosseous extension appeared to occur as a sharply marginated mass advancing into and replacing the medullary space, sometimes with outward bulging of the cortex around such tumor extension (Figs 1A, 2A and B). In patient 4, most of the tumor was located in the posterior cranial fossa, with only a slight bulge of tumor into a remodeled jugular foramen. Enlargement of the jugular foramen was always in the form of rounded, sharp contours with a sclerotic rim well appreciated on CT scans with bone algorithm (Figs 1A, 2A and B). All tumors had smooth borders and some portion growing in the posterior cranial fossa (Figs 1–3). In seven patients the tumor displaced the cerebellum and, to a lesser degree, the brain stem and fourth ventricle (Fig 1B and D). In patient 2, a small part of the tumor grew into the internal auditory canal (IAC) from within the temporal bone and also from the cerebellopontine angle (CPA), and in this latter regard simulated a vestibular schwannoma (Fig 2E). However, the main portion of the tumor was in the enlarged jugular foramen and low posterior cranial fossa, extending into the CPA (Fig 2D and F). Patient 5 had a flared IAC meatus and an adjacent CPA mass extending from the jugular foramen (Fig 1). The other patients had normal IACs. In five patients tumor extended below the skull base (Figs 1–3).
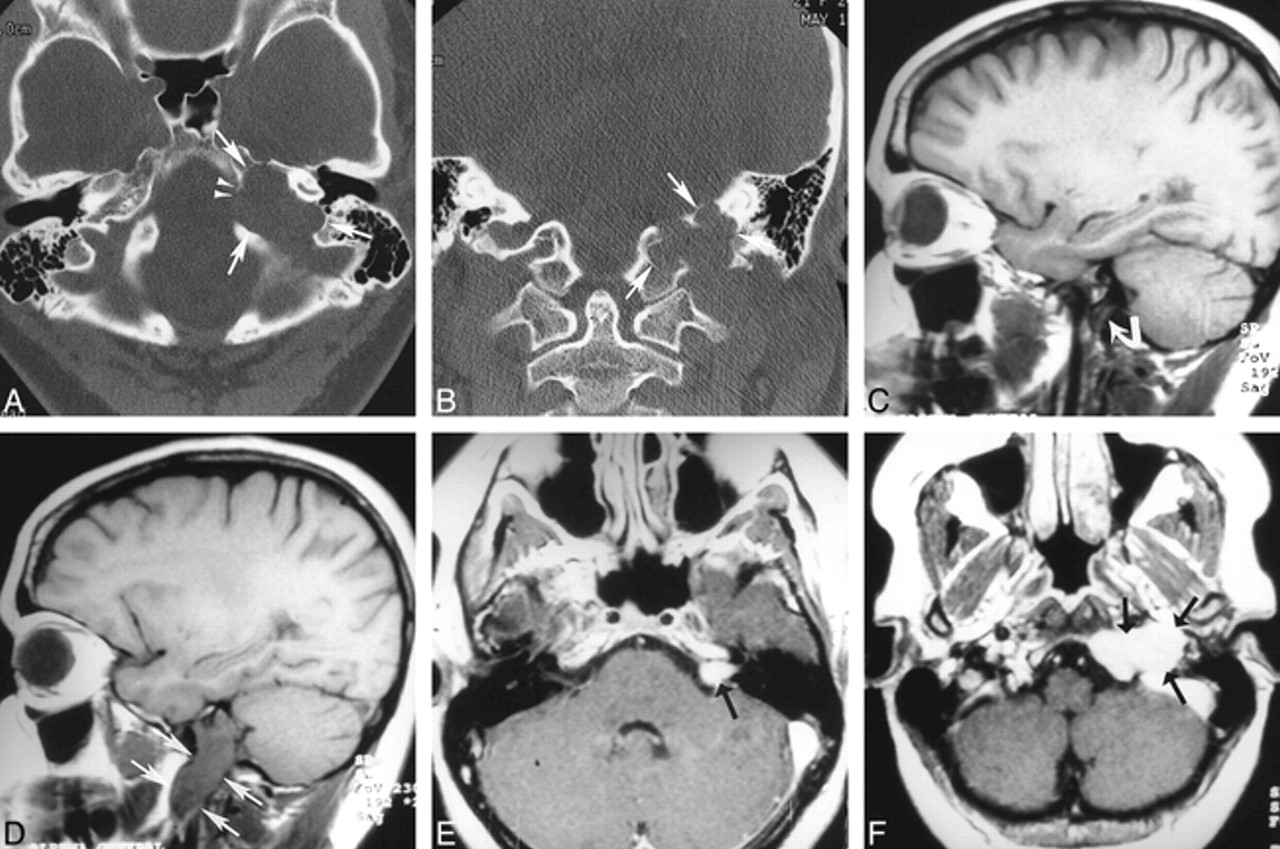
Case 2: 21-year-old woman with otalgia and sudden seventh cranial nerve paralysis.
A, Axial CT scan with bone algorithm shows marked tumor growth eroding the bone (arrows). Note rounded, sharply demarcated margins as well as erosion and bulging of cortex along the medial border (arrowheads).
B, Coronal CT scan with bone algorithm shows marked intraosseous tumor growth, rounded and sharp bone borders, and erosion and slight bulging of cortex (arrows).
C, Sagittal noncontrast T1-weighted MR image shows the patient's normal right side (arrow points to jugular foramen).
D, Sagittal noncontrast T1-weighted MR image shows a tumor with low signal intensity in the left jugular foramen, extending below the skull base (arrows).
E, Axial contrast-enhanced T1-weighted MR image shows tumor growth into the IAC (arrow), which was confirmed on coronal MR images (not shown).
F, Axial contrast-enhanced T1-weighted MR image shows that the main portion of the tumor is located within the jugular foramen and below the skull base (arrows) (compare with D).
The tumors were isodense with brain on noncontrast CT scans in six patients and hypodense in two patients. All tumors had low T1 signal and high T2 signal intensity on noncontrast MR images (Figs 1D, 2D, and 3A). Eight tumors enhanced strongly and one enhanced moderately after contrast injection on CT and/or MR studies (Figs 1B, 2F, and 3B). Three tumors had inhomogeneous enhancement and three additional tumors showed cyst formation or necrosis on CT and/or MR images. One patient had a compressed sigmoid sinus, and in seven patients the sigmoid sinus was occluded at the site of the tumor. On conventional angiography, the jugular vein on the side of the tumor was occluded in five patients and was patent in one. In one patient (case 2) mild contrast staining of the tumor was noted. Mass effect in the form of displacement of veins and/or arteries of the posterior fossa was seen in all six patients in whom angiography was performed.
Discussion
The clinical presentation of schwannomas of the jugular foramen varies significantly according to the tumor's growth pattern (7). In a relatively large series of 13 patients, deafness, vertigo, and ataxia were present if the mass was intracranial. Sweasey et al (4) reviewed the surgical literature and found that 25 of 27 reported patients with schwannomas of the jugular foramen presented with symptoms of decreased hearing; Suzuki et al (10) reported two patients with neurologic signs and CT findings suggestive of acoustic neurinoma. Hoarseness and weakness of the trapezius and sternocleidomastoid muscles occurred in some patients in whom the tumor was within the bone or extracranial (7). Except for the absence of 11th cranial nerve injury and the relative scarcity of 10th cranial nerve symptoms, our series essentially confirms this pattern, especially regarding intracranial extension. Most tumors were large, extending both into the posterior cranial fossa and below the skull base. The most common clinical presentation was hearing loss or symptoms relating to a posterior fossa mass. In patients with a large proportion of the tumor below the skull base, the symptoms tended to reflect glossopharyngeal injury.
A very large vestibular schwannoma may grow to involve the jugular foramen or the nerves entering the jugular foramen. Patients with a large vestibular schwannoma rarely have normal IACs. Pool and Pava (12) found involvement of the ninth and 10th cranial nerves in 28 of 122 patients with surgically proved vestibular schwannoma; all had enlarged IACs. In our series, all patients had an enlarged jugular foramen on the side of the tumor with rounded, sharp, and thin sclerotic rims. The IACs were normal in six of eight patients in whom CT scans were available. Patient 5 had a flared meatus of the IAC, which may have been normal although was probably due in part to tumor eroding its posterior margin, but the predominant tumor bulk was within the jugular foramen with posterior cranial fossa and intraosseous growth cephalad to involve the IAC (Fig 1). Patient 2 had similar extension to the IAC (Fig 2E and F).
In accordance with other studies, all tumors in this series showed low T1 signal, high T2 signal, and marked (or moderate) contrast enhancement (3, 9–11). Such contrast enhancement is also typical of meningiomas, although meningiomas usually have a lower T2 signal and higher precontrast CT attenuation than do schwannomas (13, 14). In addition, they may show calcification and hyperostosis; growth within the jugular foramen and/or below the skull base is unusual.
Another important differential diagnosis is tumor of the glomus jugulare. This is a highly vascular tumor, with intense contrast enhancement and, typically, multiple small flow voids (“salt and pepper” appearance on MR images). The schwannomas do not show internal flow voids, although we have seen flow voids at the periphery of some relatively vascular vestibular schwannomas. In our experience, schwannomas of the jugular foramen do not appear very vascular at conventional angiography (which was performed in six of our patients), whereas glomus jugulare tumors are highly vascular, with an intense contrast stain and readily apparent vascular pedicle(s). Vogl et al (15) assessed contrast enhancement of skull base tumors dynamically with the use of a gradient-recalled sequence. The time-intensity curve showed a dropout effect in the form of a dip in the curve during early enhancement of the sigmoid sinus and jugular bulb; this same phenomenon was found within glomus tumors of the skull base but not within schwannomas or meningiomas. In contrast to schwannomas of the jugular foramen, glomus jugulare tumors that have enlarged the jugular foramen produce irregular erosion of the margin of the jugular foramen, with decalcification or destruction of the surrounding bone (16, 17). CT with bone algorithm usually permits differentiation between glomus tumor and schwannoma. Although a schwannoma of the jugular foramen may show marked intraosseous extension (Table; Figs 1A, 2B and C), the smooth and sharply demarcated tumor margin as well as the smooth, sharply outlined, and sclerotic margin of the eroded adjacent bone suggest a histologically benign mass, as opposed to a mass with an indistinct border and irregular and destroyed adjacent bone, which would suggest an infiltrative, permeative process, such as a glomus jugulare tumor or a malignant neoplasm. While schwannomas tend to compress the jugular bulb/vein, glomus jugulare tumors tend to invade the vein and may show intraluminal growth.
Metastatic malignant tumors or lymphoma may involve the jugular foramen. Their clinical manifestations and signal characteristics may be indistinguishable from a schwannoma. However, the bone changes are most likely to be osteolytic or destructive, with less sharply marked bone borders as compared with schwannomas (18). Other lesions of the jugular foramen include pseudomass, such as normal vascular asymmetry, a high jugular bulb, or a jugular diverticulum. However, the bone structure would be normal and flow-sensitive MR imaging would confirm the vascular anatomic variant.
The surgical literature is replete with comments of how often schwannomas of the jugular foramen are confused with vestibular schwannomas (4, 8, 10, 19). If a clinical request for imaging says “unilateral hearing loss” or “acoustic neuroma,” this could lead the radiologist astray and result in an improper imaging technique and/or interpretation. To image schwannomas of the jugular foramen, dedicated CT with bone detail algorithm using 1- to 3-mm axial and/or coronal slices through the skull base is recommended, in addition to contrast-enhanced CT or MR imaging. The advantages of MR imaging are its multiplanar capabilities and the possibility of using fat suppression to reveal the exact lesion characteristics (Fig 3B).
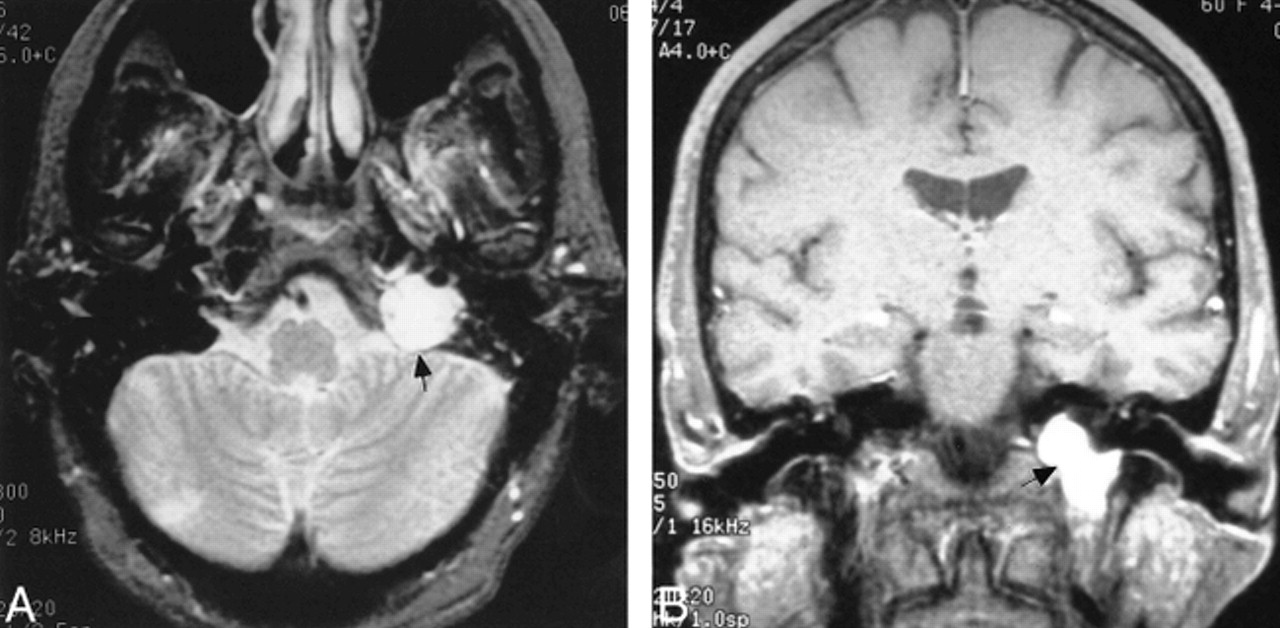
Case 9: 63-year-old woman with hearing loss, reduced gag reflex, and nystagmus.
A, Axial T2-weighted MR image shows tumor with high signal intensity within the enlarged left jugular foramen. The tumor is well demarcated with smooth borders. There is only a small tumor bulge into the posterior cranial fossa (arrow).
B, Coronal contrast-enhanced T1-weighted MR image with fat suppression shows strong and homogeneous contrast enhancement in schwannoma located below the skull base (arrow indicates level of the jugular foramen).
Conclusion
Schwannomas of the jugular foramen are rare. Patients often present with symptoms consistent with eighth cranial nerve injury or cerebellar or brain stem compression. Symptoms relating to injury of the ninth or 10th to 12th cranial nerves are less common. Although the clinical presentation of a schwannoma of the jugular foramen may suggest the presence of a vestibular schwannoma, appropriate imaging techniques and interpretation should permit correct differentiation of tumor origin and type and suggest the appropriate surgical approach. Schwannoma of the jugular foramen appears as a sharply demarcated, contrast-enhancing tumor, which is typically centered or based in an enlarged jugular foramen with sharply rounded bone borders having a sclerotic rim. Intraosseous extension may be marked.
Footnotes
1 Presented in part at the annual meeting of the American Society of Neuroradiology, Toronto, Canada, May 1997.
↵2 Address reprint requests to O. Petter Eldevik, MD.
References
- Received April 19, 1999.
- Accepted after revision January 13, 2000.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Differentiation of Jugular Foramen Paragangliomas versus Schwannomas Using Golden-Angle Radial Sparse Parallel Dynamic Contrast-Enhanced MRI
- A Compartment-Based Approach for the Imaging Evaluation of Tinnitus
- The use of CT and MRI in the characterization of intracranial mass lesions
- An unusual cause of dysphagia and dysphonia