
Abstract
BACKGROUND AND PURPOSE: Intrasaccular flow diverters are increasingly being used in the treatment of wide-neck and bifurcation aneurysms. We performed a systematic review and meta-analysis of existing literature on the Woven EndoBridge device in the treatment of intracranial aneurysms.
MATERIALS AND METHODS: A comprehensive literature search was performed through October 1, 2015. We extracted information on baseline aneurysm and patient characteristics. Outcomes studied included immediate and midterm (>3 month) angiographic outcomes (complete occlusion as well as adequate occlusion, defined as complete occlusion or neck remnant), aneurysm retreatment, intraoperative rupture, perioperative morbidity and mortality, thromboembolic complications, and treatment failure. Meta-analysis was performed by using the random-effects model.
RESULTS: Fifteen uncontrolled series were included in this analysis, including 565 patients with 588 aneurysms, of which 127 were ruptured. Initial complete and adequate occlusion rates were 27% (95% CI, 15%–39%) and 59% (95% CI, 39%–78%), respectively. Midterm complete and adequate occlusion rates after a median of 7 months were 39% (95% CI, 26%–52%) and 85% (95% CI, 78%–91%), respectively. Perioperative morbidity and mortality rates were 4% (95% CI, 1%–8%) and 1% (95% CI, 0%–2%), respectively. Midterm adequate occlusion rates for ruptured aneurysms were 85% (95% CI, 67%–98%), compared with 84% (95% CI, 72%–94%) for unruptured aneurysms (P = .89). Patients with ruptured aneurysm had similar rates of perioperative morbidity to patients with unruptured aneurysm (2%; 95% CI, 0%–26% versus 2%; 95% CI, 0%–6%, respectively; P = .35).
CONCLUSIONS: Early evidence derived from uncontrolled studies suggests that Woven EndoBridge treatment has a good safety profile and promising rates of adequate occlusion, especially given the complexity of aneurysms treated. Further prospective clinical trials are needed to confirm these results and better define the risks and benefits of use of the Woven EndoBridge device in treating wide-neck and wide-neck bifurcation aneurysms.
ABBREVIATION:
- WEB
- Woven EndoBridge
With the advent of stent-assisted and balloon-assisted coiling, wide-neck and wide-neck bifurcation intracranial aneurysms are increasingly treated with endovascular techniques. Both stent-assisted and balloon-assisted coiling have been shown safe and effective in treating these aneurysms by allowing for increased packing and lower rates of parent artery occlusion compared with conventional coiling alone.1⇓⇓⇓⇓⇓–7 However, because of less than satisfactory occlusion rates with coil embolization of wide-neck and wide-neck bifurcation aneurysms, there has been a push toward treating these lesions with intrasaccular and intraluminal flow diverters.
The Woven EndoBridge (WEB; Sequent Medical, Aliso Viejo, California) is a nitinol braided-wire intravascular device designed to disrupt blood flow at the aneurysmal neck. This device is specifically designed for the treatment of wide-neck bifurcation aneurysms.8,9 To date, several case series have demonstrated that the WEB device is both safe and effective in treatment of wide-neck and wide-neck bifurcation aneurysms.10⇓⇓–13 We present the results of a systematic review and meta-analysis examining outcomes of endovascular treatment of wide-neck and wide-neck bifurcation aneurysms with the WEB device. The aim of our study was to assess both angiographic and clinical outcomes.
Materials and Methods
Literature Search
A comprehensive literature search of 3 data bases (PubMed, Ovid MEDLINE, and Ovid EMBASE) was designed and conducted by an experienced librarian with input from the authors. The keywords “intracranial aneurysm,” “cerebral aneurysm,” “aneurysm,” “wide-neck,” “bifurcation,” “WEB device,” and “intraluminal flow diverter” were used in both “AND” and “OR” combinations. The search was limited to articles published from January 1, 2010, to October 1, 2015, and was supplemented by contacting experts in the field for any additional studies. All studies reporting patients with aneurysms treated with the WEB device were included. Inclusion criteria were the following: 1) English language, 2) study reporting a consecutive series of aneurysms treated with the WEB device, and 3) series of at least 5 patients reporting angiographic and/or clinical outcomes. Review articles, comments, guidelines, technical notes, and editorials were excluded. Two of the authors selected the included studies. A third author arbitrated in cases of disagreement.
Outcomes and Data Extraction
For each study, we extracted the following baseline information: number of patients, aneurysm rupture status, patient sex, mean age, use of core lab in assessing angiographic outcomes, number of aneurysms treated, mean aneurysm size, mean aneurysm neck size, length of clinical follow-up, and length of angiographic follow-up.
Outcomes studied included immediate and midterm (>3 month) angiographic outcomes (complete occlusion and adequate occlusion, which was defined as complete occlusion or neck remnant), aneurysm retreatment, intraoperative rupture, perioperative morbidity and mortality, thromboembolic complication, and treatment failure. Treatment failure was defined as a failed attempt at WEB device placement. Outcomes were calculated for the overall patient population with subgroup analysis by rupture status (ruptured versus unruptured). Morbidity was defined as mRS score >1. There were variable classification scales to assess aneurysm occlusion used in this study. For studies that used the WEB Occlusion Scale, complete occlusion was defined as no contrast opacification of the aneurysm with or without contrast opacification of the proximal recess of the device. Earlier studies that did not use the WEB Occlusion Scale and used the Raymond scale instead often classified contrast opacification of the proximal recess of the device as a neck remnant or did not specify recess opacification rates. Thus, for the purposes of this meta-analysis, we report adequate occlusion, which was defined as complete occlusion or neck remnant (complete occlusion with opacification of the neck).
Study Risk of Bias
We modified the Newcastle-Ottawa Quality Assessment Scale for Case Control Studies to assess the risk of bias of the studies included in this meta-analysis. This tool is designed for use in comparative studies; however, because none of the included studies were controlled, we assessed study risk of bias based on selected items from the tool, focusing on the following questions: 1) did the study include all patients or consecutive patients versus a selected sample?; 2) was the study retrospective or prospective?; 3) was angiographic and clinical follow-up satisfactory, thus allowing for ascertainment of all outcomes?; 4) were outcomes clearly reported?; and, 5) were the interventionalists treating the patients the same as those who assessed angiographic and clinical outcomes?
Statistical Analysis
We estimated from each study the cumulative incidence (event rate at the end of the study) and 95% CI. Because we anticipated marked heterogeneity in the populations and interventions across the various included studies, a random-effects model was used to pool incidence rates across studies.14 Variance was estimated by using the Freeman-Tukey double arcsine method.15 The I2 statistic was used to express the proportion of inconsistency that is not attributable to chance.16 Analysis was conducted by using STATA Statistical Software: Release 14 (StataCorp, College Station, Texas).
Results
Study Selection and Characteristics
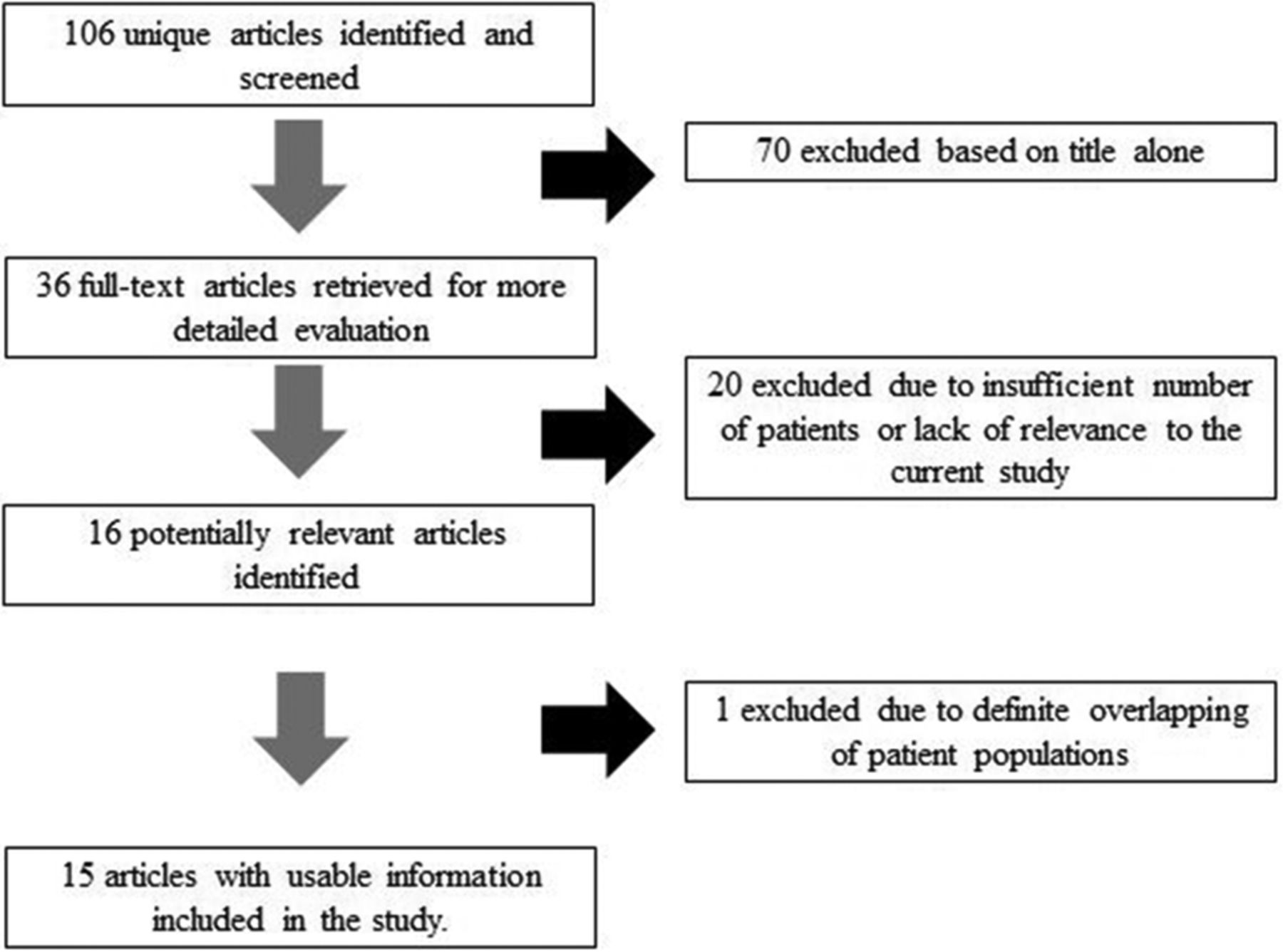
The initial literature search yielded 106 articles. Upon review of the abstracts and titles, 90 articles were excluded. Sixteen articles were selected for full-text screening. In total, 15 studies including 565 patients with 588 aneurysms were included. Of these, 127 aneurysms (22%) were ruptured and 461 aneurysms (78%) were unruptured; in no case was the rupture status unknown. There were 470 aneurysms (80%) in the anterior circulation and 118 (20%) in the posterior circulation. Seventy-three aneurysms (12.0%) were treated with adjunctive coiling, stent placement, or stent-assisted coiling. Type of pre- and postoperative antiplatelet therapy varied widely between studies.
Of the 15 studies, 6 had a low risk of bias, 3 had a high risk of bias, and 6 had a moderate risk of bias. The smallest study had 6 patients with 6 aneurysms, and the largest study had 90 patients with 98 aneurysms. Eleven studies had angiographic follow-up at 6 months or longer. A summary of included studies is provided in the On-line Table. Flow chart for study selection is provided in Fig 1.
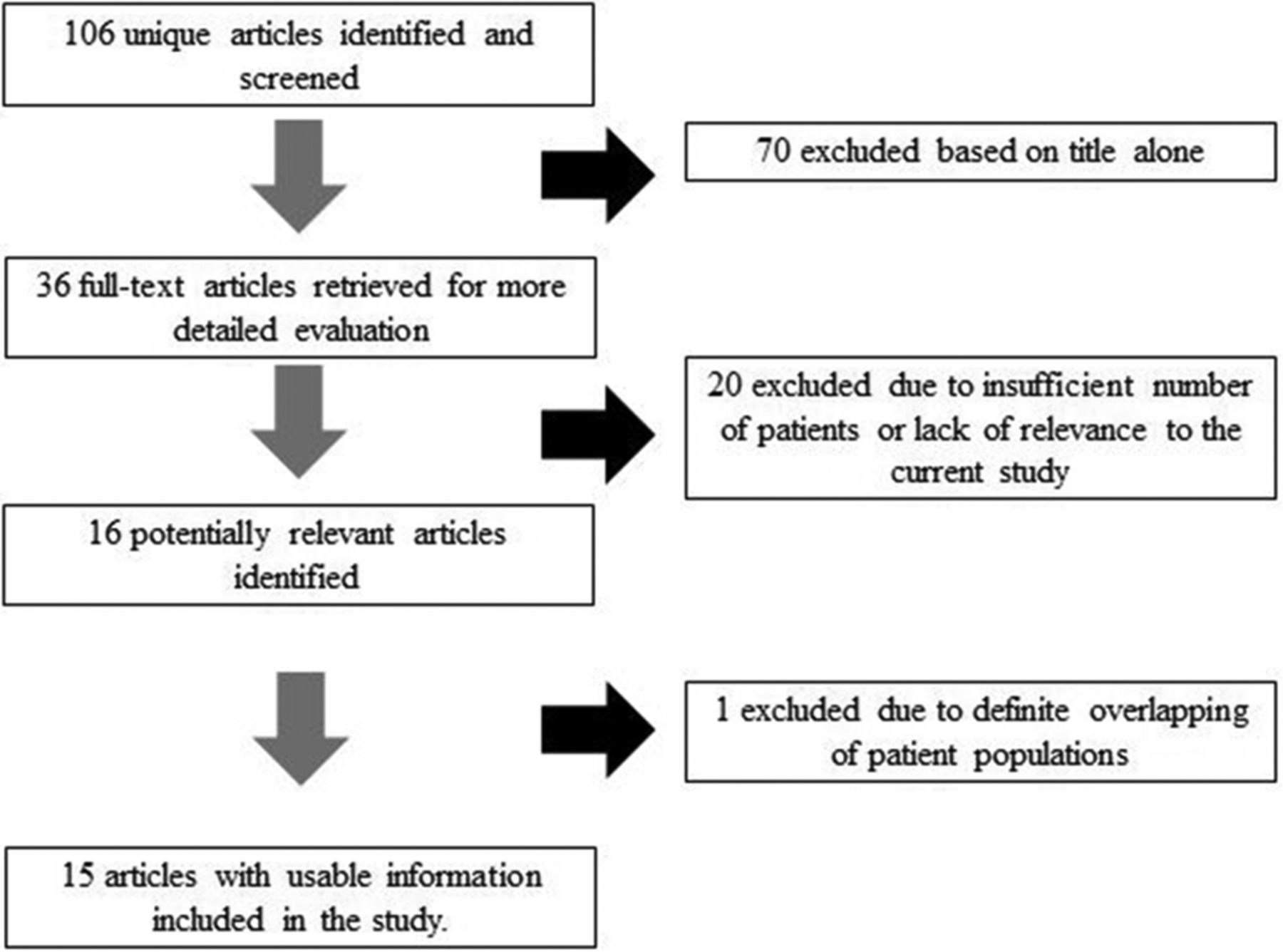
Search strategy results.
Overall Outcomes
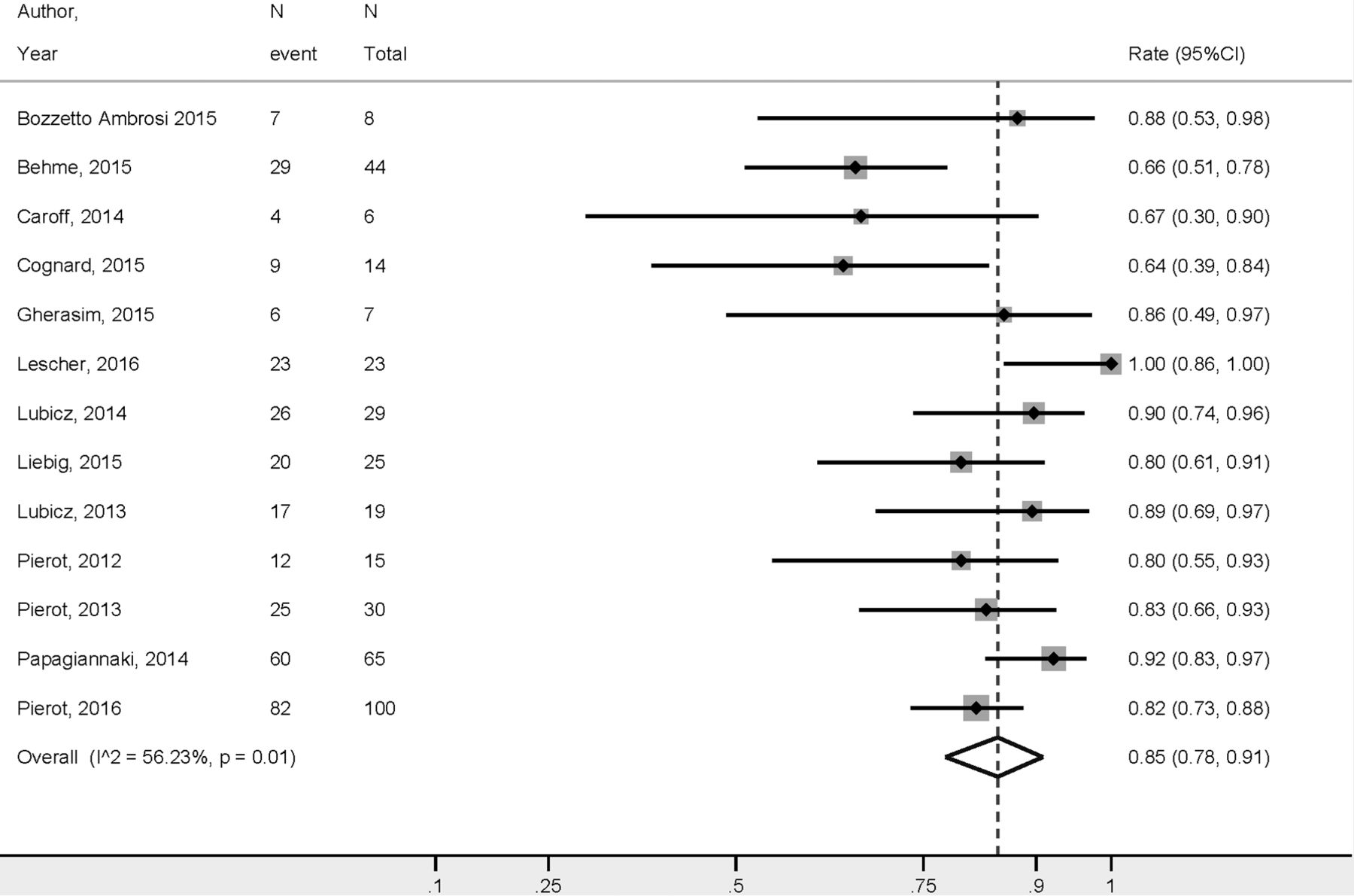
The WEB treatment outcomes are presented in Table 1. Initial complete occlusion rates and adequate occlusion rates were 27% (95% CI, 15%–39%) and 59% (95% CI, 39%–78%), respectively. Midterm complete occlusion rates after a median of 7 months were 39% (95% CI, 26%–52%) and midterm adequate occlusion rates were 85% (95% CI, 78%–91%) (Fig 2). Treatment failure occurred in 3% of cases (95% CI, 1%–6%). Perioperative morbidity and mortality rates were 4% (95% CI, 1%–8%) and 1% (95% CI, 0%–2%), respectively. The rate of thromboembolic complications was 8% (95% CI, 5%–12%). Midterm good neurologic outcome rates are provided in Fig 3.
Summary of outcomes

Midterm adequate occlusion rates overall.
Midterm good neurologic outcome rates.
Angiographic and Clinical Outcomes by Rupture Status
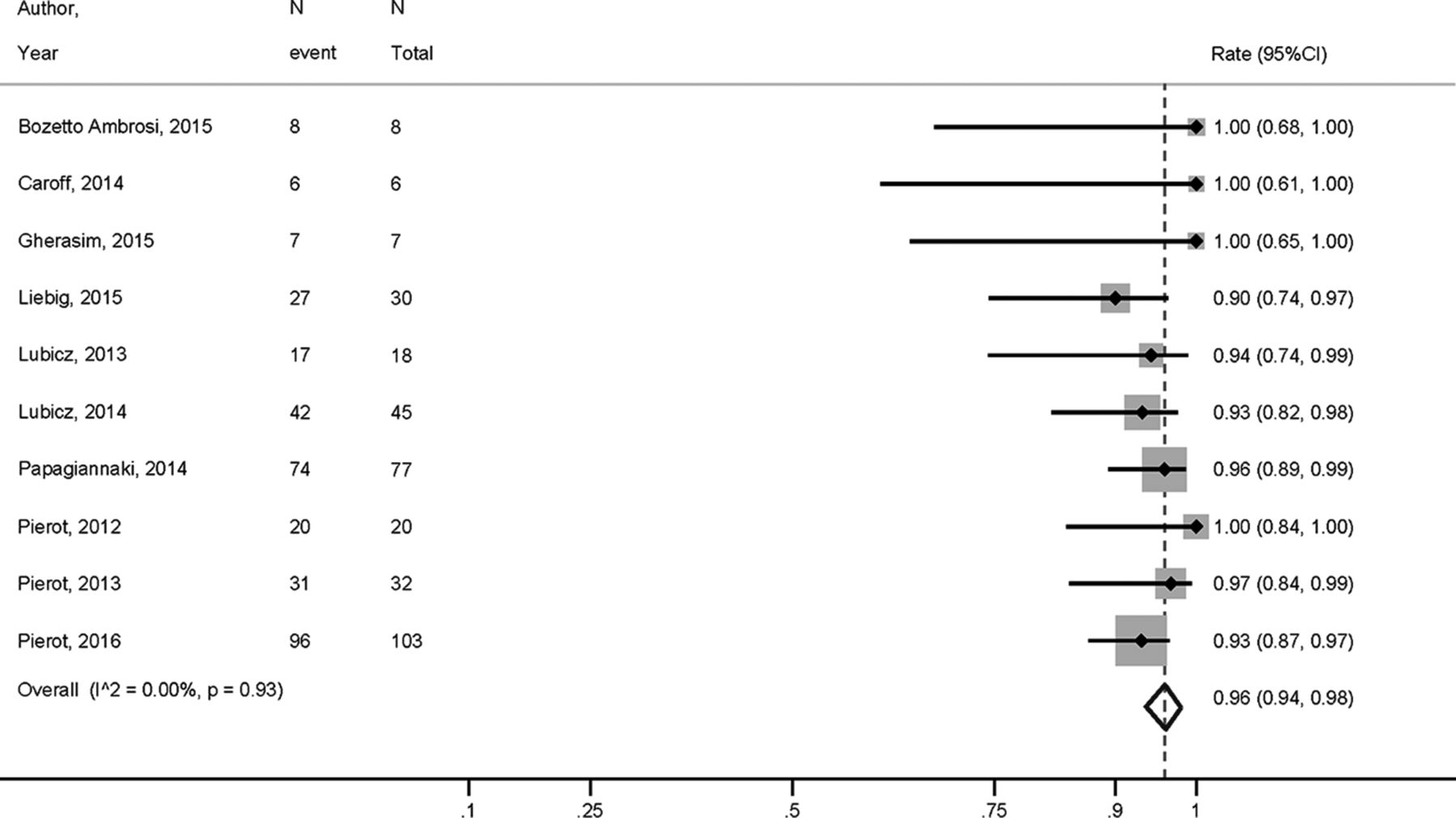
The rate of midterm complete occlusion was 45% (95% CI, 25%–65%) for the ruptured group and 22% (11%–33%) for the unruptured group (P = .008). The rate of midterm adequate occlusion for ruptured aneurysms was 85% (95% CI, 67%–98%), compared with 84% (95% CI, 72%–94%) for unruptured aneurysms (P = .89). Data on initial occlusion by rupture status were not consistently reported, and no meta-analysis could be performed for this outcome.
Patients with ruptured aneurysms had similar rates of perioperative morbidity as those with unruptured aneurysms (2%; 95% CI, 0%–26% versus 2%; 95% CI, 0%–6%, respectively; P = .35). Rates of intraoperative rupture in ruptured and unruptured aneurysms were 6% (95% CI, 0%–11%) and 1% (95% CI, 0%–3%), respectively (P = .08). Treatment failure occurred at a higher rate for unruptured aneurysms (6%; 95% CI, 3%–9%) compared with the ruptured aneurysms (0%; 95% CI, 0%–4%) (P = .04). These results are presented in Table 2.
Outcomes by rupture status
Discussion
This systematic review and meta-analysis of 15 uncontrolled studies demonstrated that treatment of wide-neck bifurcation aneurysms with the WEB device was achieved with high rates of technical success and low rates of complications. Initial adequate occlusion rate was nearly 60%, and adequate occlusion rate at follow-up was 85%. There were no substantial differences in outcomes by rupture status. These findings are important because they suggest that the WEB device might be a valuable tool in the treatment of wide-neck bifurcation aneurysms regardless of rupture status.
As demonstrated by this meta-analysis, a number of prior studies have examined the safety and efficacy of the WEB device. In a systematic review of 6 studies by Armoiry et al,17 the authors reported high rates of treatment feasibility (93%–100%) with adequate occlusion rates between 65% and 85% at midterm follow-up. Permanent morbidity rates ranged from 2%–7% depending on the series, and mortality ranged from 0%–17%. Our study differs from the systematic review performed by Armoiry et al17 in that we conducted a formal meta-analysis and were able to pool data from 15 studies including over 550 patients. By doing so, we were able to report efficacy and complication rates with narrow confidence intervals and provide important subgroup analyses of outcomes by rupture status.
Midterm occlusion rates with the WEB device were slightly higher than those reported for stent-assisted coil treatment of wide-neck bifurcation intracranial aneurysms. Typical long-term complete or near-complete occlusion rates for coiling of wide-neck and bifurcation aneurysms is generally on the order of 70%.18⇓–20 One recently published meta-analysis of over 2000 patients undergoing stent-assisted coiling of wide-neck bifurcation aneurysms found long-term occlusion rates of 73%.21 Meanwhile, our study found a long-term adequate occlusion rate of 80%. Initial occlusion rates were approximately 60% with the WEB device, compared with 54% for stent-assisted coiling of wide-neck bifurcation aneurysms. In addition to improved occlusion rates, a distinct advantage of treatment with the WEB device compared with stent-assisted coiling is the fact that pre- and/or intraoperative antiplatelet therapy is generally not required for WEB treatment. This is particularly important in the treatment of ruptured aneurysms.
Given the short length of follow-up available in many of the included studies (median of 7 months), the angiographic outcomes of the WEB device are generally similar to flow diversion. Complete occlusion rates in studies reporting 6–12 month follow-up for flow diversion typically range from 70%–93%.22⇓⇓⇓–26 One large meta-analysis of 1451 patients with 1654 aneurysms treated with flow diverters found complete occlusion rates of 76%, with a vast amount of studies reporting follow-up after less than 12 months, similar to our results. In general, occlusion rates with flow diversion improve with increased follow-up as studies with 24 months or more of follow-up report occlusion rates over 90%.26⇓–28 Similar to flow-diversion therapy, occlusion rates with the WEB device generally increase with time because the healing process after placement of an intra-aneurysmal flow diverter involves a complex process of loose connective tissue deposition followed by endothelialization of the device–neck interface. Given the lack of consistent long-term (ie, >12 months) follow-up in the studies included in this meta-analysis, it is possible that we are in fact underestimating long-term occlusion rates.
This systematic review also demonstrated that complication rates associated with the WEB device were relatively low. Among unruptured aneurysms, perioperative morbidity rates were less than 3% despite a thromboembolic and iatrogenic rupture rate of 9%. Ruptured aneurysms had higher complication rates, which are likely due in part to preoperative morbidity and aneurysm complexity. Perioperative morbidity and mortality rates for stent-assisted coiling of unruptured aneurysms are similar, ranging from 3%–5% depending on the study.29,30 One recently published meta-analysis of stent-assisted coiling of wide-neck and bifurcation aneurysms found procedure-related morbidity and mortality rates of 3% and 1%, respectively.21 However, these conventional techniques are associated with poorer long-term angiographic outcomes and are hampered by the need for perioperative dual antiplatelet therapy, a factor that is particularly important in the treatment of ruptured aneurysms.31,32 Permanent morbidity and mortality rates related to flow-diverter treatment range from 8%–10%.33 Thus, our findings suggest that the WEB device has a safety profile similar to flow diversion.
Limitations
The main limitation of this meta-analysis is that all the included studies were uncontrolled and many were retrospective. Many were also single-center and reported a wide variety of aneurysm morphologies and patient scenarios. There also might be variability in practice patterns and operator and medical center expertise. This is evident by the wide range of antiplatelet therapy regimens that were administered to patients before and after WEB treatment. There remains the possibility that there could be overlap in patients among studies. Although we were careful to exclude studies that had overlapping patient populations by examining the time periods studied and institutions where the patients were treated, in some cases, articles were not clear as to whether patients included in their studies were included in prior publications or in larger registries. The mean length of follow-up in the reviewed literature was modest. Another limitation is the lack of stratification of outcomes based on important variables such as type and size of the WEB device in many of the included studies. Publication bias is quite likely, and the role of the device manufacturer in the research is not fully clear. Lastly, we do not have data on baseline patient morbidity. Thus, we are unable to determine what proportion of patients with poor neurologic function at follow-up developed this after the procedure. Therefore, the overall certainty in the evidence at present is rated very low.34
Conclusions
Our meta-analysis of 15 studies including over 500 patients with over 500 aneurysms treated with the WEB device demonstrated that the WEB device has a safety profile similar to other endovascular devices such as coils and flow diverters. Furthermore, the WEB device is associated with satisfactory midterm angiographic adequate occlusion rates. These findings are particularly important given the complexity of aneurysms treated. Further prospective clinical trials, including clinical trials comparing WEB device treatment with conventional endovascular and surgical techniques, are needed to confirm these results and better define the risks and benefits of using the WEB device in treatment of wide-neck and wide-neck bifurcation aneurysms.
Footnotes
Disclosures: Laurent Pierot—RELATED: Consulting Fee or Honorarium: Sequent; UNRELATED: Consultancy: Blockade, Medtronic, Microvention, Neural, Penumbra. David F. Kallmes—UNRELATED: Board Membership: GE Healthcare,* Comments: cost-effectiveness board; Consultancy: Medtronic,* Comments: clinical trials planning and implementation; Grants/Grants Pending: Sequent Medical,* MicroVention,* Codman,* Medtronic,* NeuroSigma,* Surmodics,* Comments: preclinical research and clinical trials support; Travel/Accommodations/Meeting Expenses Unrelated to Activities Listed: Medtronic,* Comments: presentation at FDA panel meeting. *Money paid to the institution.
References
- Received April 4, 2016.
- Accepted after revision June 24, 2016.
- © 2016 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Large Single-Center Experience with Short-Term Follow-up of Neqstent-Assisted Coiling
- WEB for recurrent aneurysms: a case series to review technical nuances
- Management of aneurysmal recurrence after Woven EndoBridge (WEB) treatment
- Systematic Review and Meta-Analysis of Endovascular Therapy Effectiveness for Unruptured Saccular Intracranial Aneurysms
- Use of the Woven EndoBridge Device for Sidewall Aneurysms: Systematic Review and Meta-analysis
- A mini-review of intrasaccular flow diverters
- WEB Treatment of Ruptured Intracranial Aneurysms: Long-Term Follow-up of a Single-Center Cohort of 100 Patients
- Intracranial aneurysm treatment with intrasaccular flow disruption: comparison of WEB-21 and WEB-17 systems
- Intracranial aneurysm treatment with WEB and adjunctive stent: preliminary evaluation in a single-center series
- Woven EndoBridge device for ruptured aneurysms: perioperative results of a US multicenter experience
- High-resolution image-guided WEB aneurysm embolization by high-frequency optical coherence tomography
- Woven EndoBridge (WEB) device in the treatment of ruptured aneurysms
- Shape Modification is Common in Woven EndoBridge-Treated Intracranial Aneurysms: A Longitudinal Quantitative Analysis Study
- Endosaccular flow disruption: where are we now?
- Low-Profile Intra-Aneurysmal Flow Disruptor WEB 17 versus WEB Predecessor Systems for Treatment of Small Intracranial Aneurysms: Comparative Analysis of Procedural Safety and Feasibility
- Predicting Factors of Angiographic Aneurysm Occlusion after Treatment with the Woven EndoBridge Device: A Single-Center Experience with Midterm Follow-Up
- Two-Center Experience in the Endovascular Treatment of Intracranial Aneurysms Using the Woven EndoBridge 17 Device Including Midterm Follow-Up Results: A Retrospective Analysis
- Clipping of recanalized intracerebral aneurysms initially treated by the Woven EndoBridge device
- Stent-assisted coiling of cerebral aneurysms using the Y-stenting technique: a systematic review and meta-analysis
- Treatment of Wide-Neck Intracranial Aneurysms with the Woven EndoBridge Device Associated with Stenting: A Single-Center Experience
- Safety and efficiency of the fifth generation Woven EndoBridge device: technical note
- Balloon remodeling-assisted Woven EndoBridge technique: description and feasibility for complex bifurcation aneurysms
- Aneurysm Characteristics, Study Population, and Endovascular Techniques for the Treatment of Intracranial Aneurysms in a Large, Prospective, Multicenter Cohort: Results of the Analysis of Recanalization after Endovascular Treatment of Intracranial Aneurysm Study
- Y-Stent-Assisted Coiling of Wide-Neck Bifurcation Intracranial Aneurysms: A Meta-Analysis
- Treatment of recurrent aneurysms using the Woven EndoBridge (WEB): anatomical and clinical results
- The New Low-Profile WEB 17 System for Treatment of Intracranial Aneurysms: First Clinical Experiences
- Endovascular treatment of intracranial aneurysms with the Woven EndoBridge device: mid term and long term results
- Two-Center Experience in the Endovascular Treatment of Ruptured and Unruptured Intracranial Aneurysms Using the WEB Device: A Retrospective Analysis
- WEB Device: Ready for Ruptured Aneurysms?
- WEB Treatment of Ruptured Intracranial Aneurysms: A Single-Center Cohort of 100 Patients
- Safety and Efficacy of Aneurysm Treatment with the WEB: Results of the WEBCAST 2 Study
- Reply:
- More Transparency Is Needed in the Reporting of Clinical Research Studies