
Abstract
BACKGROUND AND PURPOSE: Membrane filters are EPDs, which preserve ICA flow during CAS. However, ICA flow arrest may occur with filter use. This report describes the angiographic, clinical, and histopathologic features of the filter occlusion.
MATERIALS AND METHODS: Sixty-one consecutive patients with cervical carotid stenosis treated by CAS by using a single type of filter device were evaluated. All patients were on dual antiplatelet treatment and fully heparinized. Prestent dilation was performed in all patients. Poststent dilation was performed in 15 patients. Control angiograms were obtained and evaluated after each step of the CAS procedure. All filters were inspected for debris, and if present, histology was obtained.
RESULTS: CAS was successfully performed in all cases with <20% residual stenosis. Filter occlusion occurred in 6 patients (9.8%). It developed immediately after stent deployment in 4, and after a second prestent dilation in 2. Five of the 6 had severe carotid stenosis. In all patients, filter withdrawal led to immediate and complete restoration of ICA flow. In 1 patient, acute embolic M1 occlusion occurred immediately after filter withdrawal but was successfully treated with thrombolysis. None of filter-occlusion group had permanent neurologic deficits. Gross and microscopic examinations demonstrated that the pores of the filters were occluded mainly by fibrin. Postoperative diffusion MR imaging revealed no difference between filter-occlusion and non-filter-occlusion groups.
CONCLUSIONS: ICA flow arrest due to filter occlusion during CAS is relatively common and occurs more frequently in severe stenosis. It resolves rapidly after filter removal and does not appear to worsen outcome.
ABBREVIATIONS:
- ACT
- activated clotting time
- aPTT
- activated partial thromboplastin time
- CAS
- carotid artery stent placement
- EPD
- embolic protection device
EPDs have been widely used to reduce embolic risk during CAS.1 One type of EPD is a filter device that has the advantage of preserving ICA flow during the procedure. This may be advantageous in cases of poor collateral circulation including severe stenosis of the contralateral carotid artery and/or stenosis of the vertebral arteries. One possible disadvantage of the filter device that has been encountered is a severe stagnation or arrest of ICA flow. Several reports suggest that it is relatively common, occurring with ≤30% incidence and caused by occlusion with embolic material.2⇓⇓–5 This unexpected event could possibly cause ischemia, lead operators to proceed in haste, and consequently lead to complications. In this article, we describe our experience with filter occlusion, including its angiographic and histopathologic characteristics and the clinical implications. Additionally, a pathophysiologic mechanism for this event is suggested.
Materials and Methods
Sixty-one patients with cervical carotid stenosis were treated in Seoul National University Bundang Hospital by elective stent placement with the use of a single filter-protection device (Emboshield; Abbott Vascular Devices, Redwood City, California) during a 2-year period (June 2004–July 2006). There were 58 men and 3 women with a mean age of 69.8 ± 7.5 years (range 47–87 years). Fifty-nine patients (97%) had previous symptoms of TIA and/or stroke.
The degree of stenosis was assessed by 3D reconstruction angiograms and described according to the NASCET criteria. Ulceration was described when the depth of the ulcerative lesion was >1 mm on the angiographic 3D image. The time interval from the last TIA or stroke to CAS was recorded. During the study period, early intervention was not routine; therefore, only 3 patients underwent CAS within 3 weeks after the last symptom. Cumulatively, CAS was performed in 18 patients within 4 weeks (30.5%), 26 (44.1%) within 2 months, 36 (59.0%) within 3 months, 40 (65.6%) in 6 months, and 58 (95.1%) within 1 year after last the neurologic symptom. The maximum was 2 years.
All CAS procedures were performed with the patient under local anesthesia in a neuroangiography suite by using biplane angiography equipment (Integris; Philips Healthcare, Best, the Netherlands). An 8F sheath was used for access. The Emboshield was first positioned and opened distal to the stenosis. In 14 cases in which the stenosis appeared too tight to allow the filter passage, prefilter dilation was performed with a 2.5- to 3-mm diameter balloon. Prestent dilation was performed after filter placement in all patients by using balloon sizes ranging from 4 to 6 mm. The balloons were generally inflated just once. In 6 cases, a second prestent dilation by using the same or a larger balloon was required to obtain satisfactory angiographic results. The S.M.A.R.T. Control stent (Cordis, Miami Lakes, Florida) was implanted in 51 patients, and the Zilver stent (Cook, Bloomington, Indiana), in 10. Poststent dilation was performed in 15 patients by using 4- to 6-mm balloons. Control angiograms were obtained and evaluated after each step of the procedure (before and after filter placement, prestent dilation, stent deployment, poststent dilation, and, finally, after withdrawal of the filter devices).
All filters were extracted from the retrieval catheter and inspected for embolic debris in the angiography suite immediately after the CAS procedure. The blood inside the filter often interfered with clear visualization of possible debris. Therefore during the early period of our experience, we gently irrigated the filter basket with saline, while holding the proximal filter frames. Occasionally, filters were squeezed gently with saline-soaked gauze to remove contaminants. We realized that a significant amount of captured embolic material could be lost with such manipulation and started routinely removing contaminants with sharp forceps without irrigation to minimize loss of debris. Any debris found inside the filter was sent for pathologic analysis.
All patients received 3000 U of unfractionated heparin intravenously at the start of the procedure. In most cases, the entire procedure took <1 hour, so additional heparin was not administered. aPTT was checked 1 day before the procedure as the baseline and within 30 minutes after the procedure in 60 patients (98%). It was longer than 5 times the baseline (>180 seconds) in 37 (61%), 4–5 times in 12 (20%), 3–4 times in 7 (11%), and 2–3 times in 4 (6%). All patients were pretreated with aspirin (100 mg daily) and clopidogrel (75 mg daily) at least 7 days before the procedure, and these were continued for 6 months after CAS. If no recurrent symptoms or signs at clinical and imaging follow-up were encountered, clopidogrel was discontinued at 6 months, while aspirin was continued life-long. One patient in whom acute embolic M1 occlusion developed after filter removal was given low-molecular-weight heparin for 3 days. Routine diffusion MR imaging was performed 1 day after CAS in 57/61 (93.4%) patients. The Fisher exact test and χ2 test were used to analyze a potential relationship between various variables and the occurrence of filter occlusion.
Results
CAS was successfully performed in all attempted cases with no more than 20% residual stenosis. The mean pretreatment stenosis was 83 ± 13% (range, 50%–99%). Forty-six percent of patients had severe stenosis (stenosis ≥90%). Twenty-eight patients (46%) had at least 1 ulceration on pretreatment angiography. There were 10 (16.4%) procedure-related neurologic events during or within 7 days following CAS. These included 7 transient neurologic deficits, 2 minor strokes, and 1 death due to massive intracerebral hemorrhage.
Filter occlusion occurred in 6 patients (9.8%). It developed immediately after stent deployment in 4 patients (Figs 1 and 2) and after the second prestent dilation in 2 patients. In all cases of filter occlusion, angiograms showed complete or near-complete occlusion of ICA flow. Neither dissection nor spasm severe enough to produce ICA flow impairment was observed. In all 6, ICA flow was promptly restored as soon as the filters were retrieved. No other specific treatment was introduced to the patients with filter occlusion.
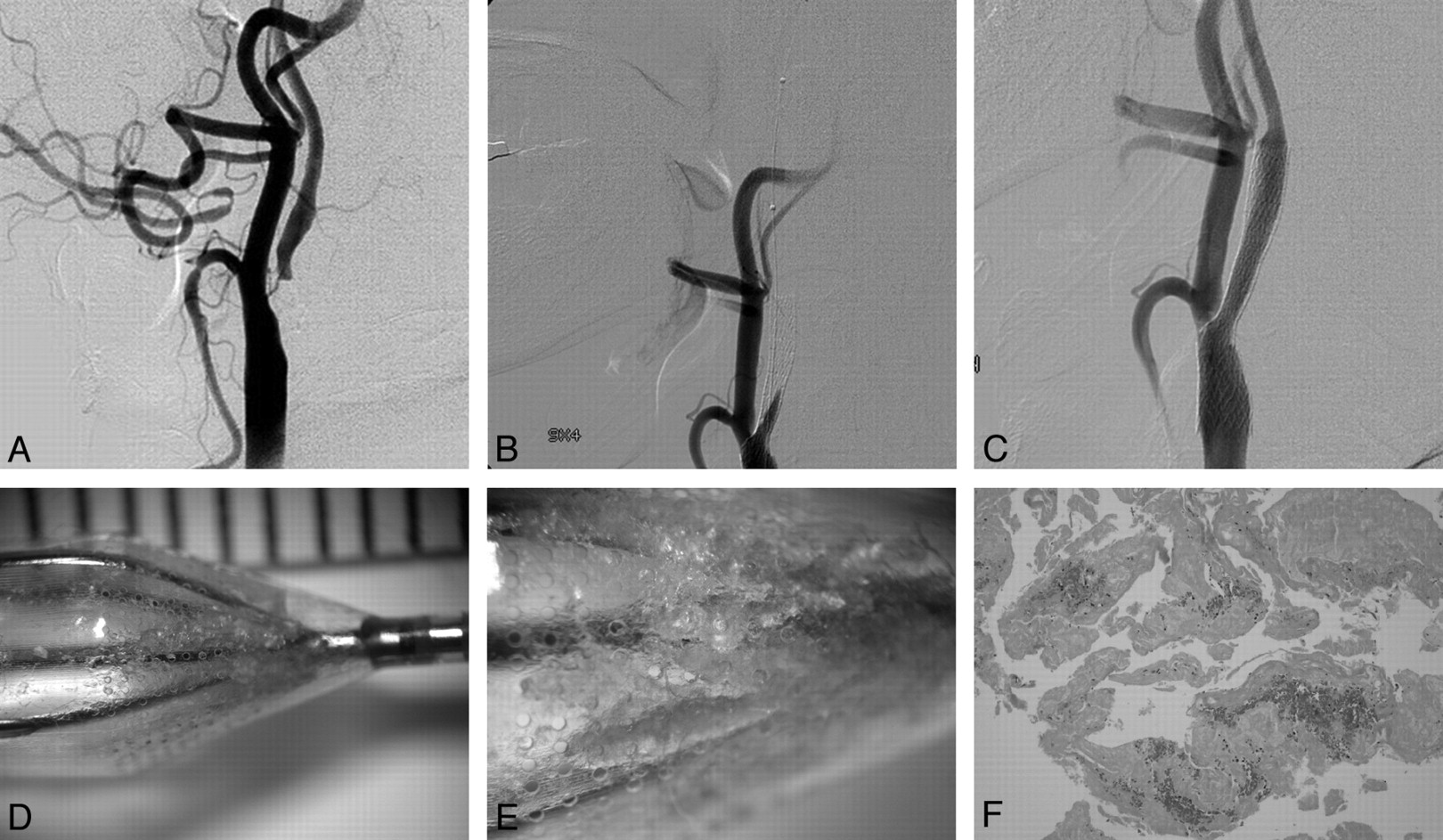
A 56-year-old male patient who presented with left hemiparesis and dysarthria. A, Right common carotid angiogram shows a severe stenosis of >95%. An Emboshield was placed after prefilter dilation by using a 2.5-mm balloon; then, prestent dilation was performed with a 4-mm balloon (not shown). B, Angiogram obtained immediately after stent (S.M.A.R.T., 9 × 40 mm) deployment shows ICA flow arrest. C, ICA flow is normalized immediately after filter withdrawal. D, Gross inspection reveals several open pores in the filter membrane and a relatively small amount of debris within the filter. E, More magnified view demonstrates that many pores are occluded by semitranslucent debris. F, Histopathologic examination shows that these materials mainly consist of fibrin (H&E, original magnification ×40).
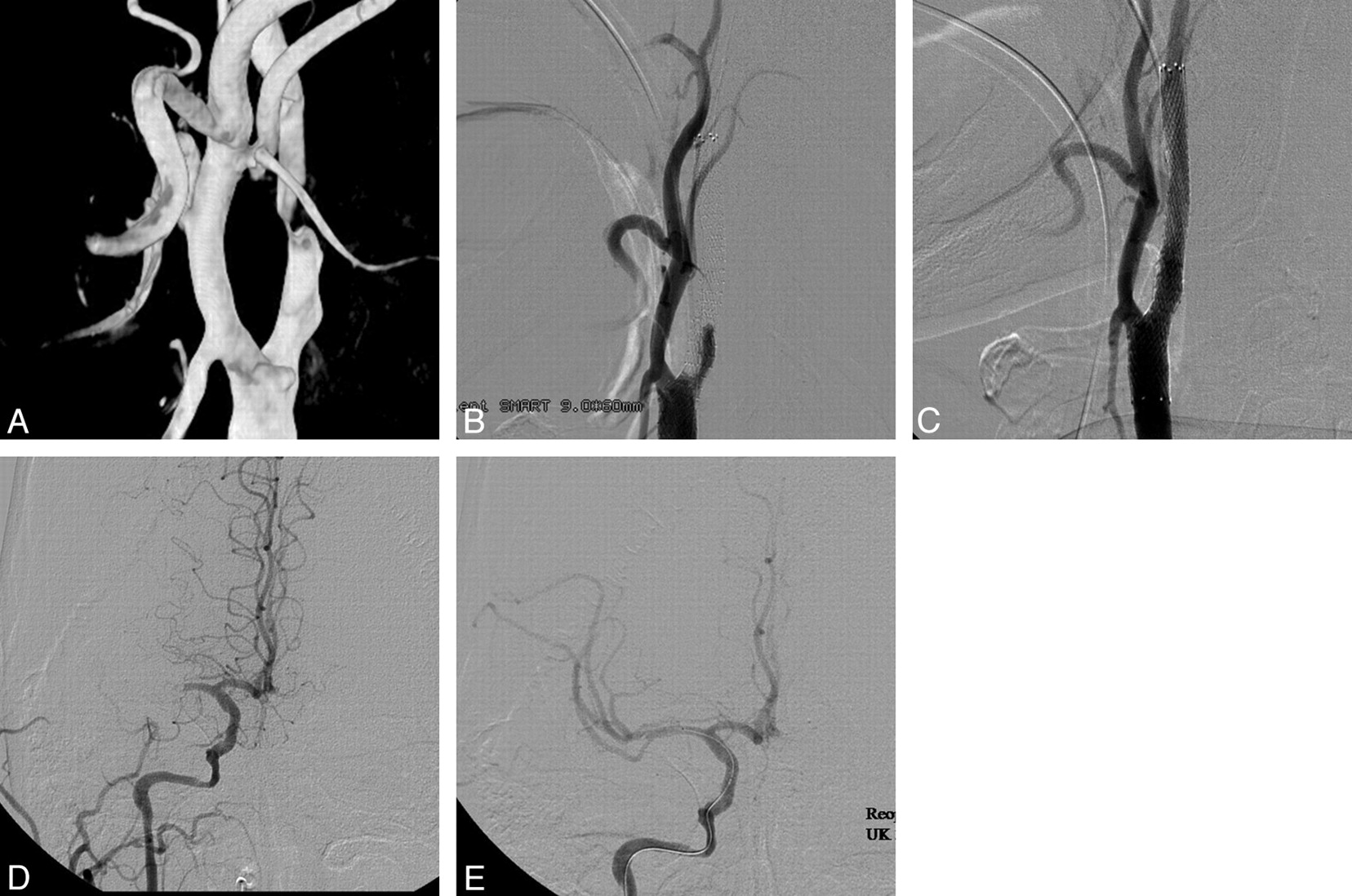
A 64-year-old male patient who presented with transient left hemiparesis. A, 3D reconstruction angiogram shows severe carotid stenosis. An Emboshield was placed after prefilter dilation by using a 3-mm balloon; then, prestent dilation was performed with a 4-mm balloon (not shown). B, Angiogram after stent (S.M.A.R.T., 9 × 60 mm) deployment shows ICA flow arrest. C, ICA flow is normalized immediately after filter withdrawal. D, Cerebral angiogram shows acute embolic M1 occlusion. The patient became stuporous and hemiparetic. E, Right M1 is recanalized after intra-arterial thrombolysis with 380,000 U urokinase and 6 mg abciximab.
In the filter-occlusion group, 5 of the 6 had severe carotid stenosis (≥90%). The sixth patient had 80% stenosis. Five of 6 patients also had pretreatment ulceration. Statistical analysis did not reveal variables that correlated with filter occlusion, including degree of stenosis, ulceration, preoperative TIA, prior stroke, and timing of CAS. In 3 of 6 patients with filter occlusion, aPTT, checked within 30 minutes of CAS, was beyond 180 seconds; in 2 patients, it was 4–5 times the baseline and 3–4 times in 1. In the filter-occlusion group, poststent dilatation was not attempted to reduce the time of ICA flow arrest. However, residual stenosis was <20% in all these patients because prestent angioplasty was performed with relatively large-sized balloons.
In all of the 6 patients with filter occlusion, no neurologic symptom developed during the ICA flow arrest. One patient with filter occlusion experienced a temporary deficit. This was due to an acute embolic M1 occlusion that occurred as the filter was withdrawn. The occlusion led to hemiparesis, which rapidly resolved with intra-arterial urokinase and abciximab (Fig 2). None of filter-occlusion group had permanent neurologic deficits.
Fifty-seven patients were studied by MR imaging and 25 (44%) showed new ischemic lesions. Lesions were observed in 43% of the non-filter-occlusion group and 50% of the filter-occlusion group (P = 1.0).
In all patients, clinical follow-up was performed for a minimum of 6 months (average, 18.5 ± 7.2 months); during the follow-up, 3 patients experienced TIA. All patients in the filter-occlusion group had clinical follow-up for >12 months (range, 13–25 months), and none experienced recurrent symptoms. Follow-up imaging for carotid artery stents included conventional angiography and/or CT angiography. This was performed at least 12 months after CAS in 34 patients (55.7%) and demonstrated restenosis of >20% in 5 patients, including 1 patient in the filter-occlusion group.
A substantial amount of filter debris was present in 14 cases (25.5%) in the non-filter-occlusion group and 4 cases (66.6%) of the filter-occlusion group. In the remaining 43 collected filters, it is believed that only blood contaminants were present on the filters. When embolic debris was present, it consisted of mainly gelatinous yellow-whitish or sometimes whitish semisolid materials. Most were collected at the distal end of the filter membrane, but some of the gelatinous materials were attached to the nitinol frames of the filter (Fig 3A). In the filter-occlusion group, many pores of the filter membrane were mechanically occluded by semitranslucent gelatinous materials (Fig 1D, -E). Histopathologically, the debris consisted predominantly of fibrin embedded in blood components such as red and white blood cells. Sometimes, small amounts of atherosclerotic plaque material such as lipid-rich macrophages and cholesterol were also found (Fig 1F).
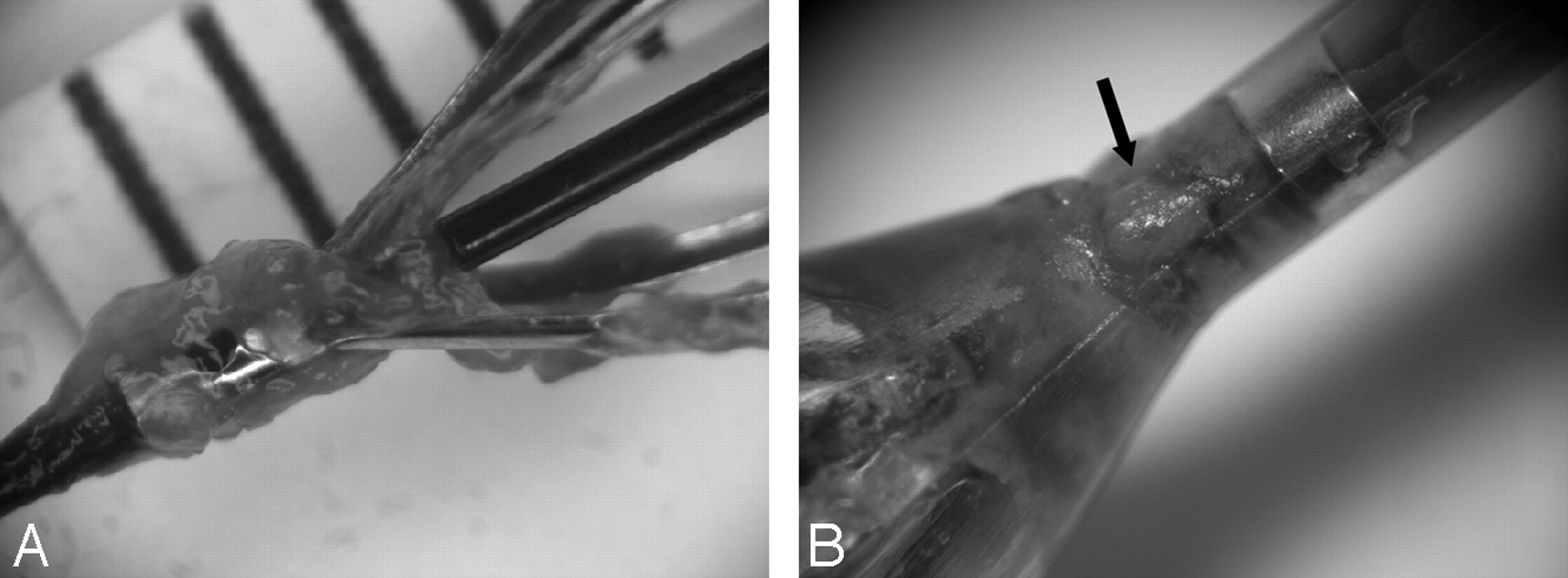
A, A photograph of the filter after carotid artery stent placement shows that gelatinous fibrin material is collected within a filter (filter membrane was removed). B, A magnified view demonstrates that squeezed embolic material is located outside the filter membrane (arrow).
Discussion
ICA flow arrest or slowing due to filter occlusion during CAS is a significant technical drawback, which eliminates the advantage of preserving ICA flow with filter-type EPD use. There have been several reports of this event2⇓⇓–5 that suggest that this is not rare. Angelini et al2 observed ICA flow impairment in 21% of 37 lesions treated with CAS. In a series of 53 patients, Bonaldi et al3 observed a slowing of the ICA flow in 9 and total occlusion in 6 patients, so the incidence of the event was approximately 30%. Castellan et al4 also reported a 30% incidence. Recently, Kwon et al5 showed an 8% incidence, similar to that of the present study. This event occurred shortly after either balloon dilation (mostly poststent dilation) or stent deployment. In addition, it is not confined to a specific filter. Various membrane-type filter devices such as AngioGuard (Cordis), FilterWire (Boston Scientific, Natick, Massachusetts), or Emboshield have been implicated.
There are several clinical implications of this event. First, associated ICA flow impairment may lead to cerebral ischemia. In a series of 72 patients, Kwon et al5 reported 6 patients with flow impairment during protected CAS, and 4 of them had neurologic symptoms. Our patients remained stable, and neurologic symptoms did not emerge despite the filter occlusion, probably due to good collateral circulation and rapid flow restoration by filter withdrawal.
Although patients remained stable during ICA flow arrest, these events led the operator to speed up the remaining procedure—retrieval of the stent delivery catheter, poststent dilation, introducing the filter-retrieval catheter, and withdrawal of the filter. This change can precipitate unexpected procedure-related complications. The acute embolic M1 occlusion experienced in this series might well have resulted from squeezing embolic debris through the filter pores during the filter capture into the retrieval catheter. Because of the character and amount of debris, entrapping the filter into the retrieval catheter could squeeze out the semisolid gel-like fibrin through the filter pores. Indeed, embolic fragments were seen extending through the filter pores (Fig 3B). To prevent or avoid this, gentle, slow, and partial filter recapturing into the retrieval catheter is recommended.6
In terms of management, direct intra-arterial fibrinolytics may be helpful in restoring ICA flow because fibrin appears to be the key material for filter occlusion. However, the present study shows that withdrawal of the filter quickly re-establishes normal flow. Diffusion MR imaging, which was performed 1 day after CAS, did not show more areas with restricted diffusion in the filter-occlusion group compared with the non-filter-occlusion group. In addition, filter occlusion does not seem to predispose to subsequent ischemic events during the early or late period after CAS. None of 6 patients with ICA flow arrest from filter occlusion developed recurrent TIA or stroke after the procedure and follow-up of >12 months.
We did not observe a direct relationship between the filter-occlusion and anticoagulation level. Although the aPTT, instead of the ACT, was monitored, so that quantitative analysis could not be performed, it is believed that all patients with filter occlusion were under full heparinization during the procedures because the aPTT was at least 3 times the baseline in the filter-occlusion group. However, there have been reports of a relationship between inadequate anticoagulation and filter occlusion. Castellan et al4 suggested that filter occlusion is associated with a low anticoagulation level. In their series of 29 CASs, the ACT of 9 patients with filter occlusion was 367 seconds (range, 320–450 seconds), while it was 423 seconds (range, 360–550 seconds) in the non-filter-occlusion group.4 Bonaldi et al3 also found that filter occlusion is related to an insufficient anticoagulation level and suggested more aggressive anticoagulation (at least 3 times the ACT baseline), but they failed to eliminate filter occlusion even with the aggressive anticoagulation and reported hemorrhagic complications. Further studies with large series are probably necessary to clarify the impact of anticoagulation level on filter occlusion.
The present study shows that fibrin predominates in the debris retrieved following filter occlusion. The exact origin of the fibrin is still obscure. It is possible that new fibrin could be formed locally on the filter membrane if thrombogenic plaque materials are captured. However, the present study and prior studies3,4 have demonstrated that the debris captured by the EPD mainly consists of fibrin and plaque fragments that are often scanty or nonexistent. Flow arrest during balloon inflation might initiate stasis-induced thrombosis within the filters,3 but in practice, the balloon-inflation time is short (5–10 seconds in our experience). Moreover, procedures are performed with the patient under heparinization. The polyurethane filter membrane has been widely used as a biocompatible material.7 Nevertheless, it is possible that fibrin formation occurred on the filter membrane.
Because filter occlusion abruptly occurred after stent deployment or balloon inflation, we believe that another possible source is the plaque itself. Thrombotically active plaques are defined by the presence of an acute thrombus composed of platelets or fibrin on the plaque surface and are frequently found in symptomatic carotid stenosis.8 Preformed fibrin from thrombotically active plaques may be detached with stent deployment or balloon inflation. In addition, mechanical injuries associated with balloon angioplasty, such as gross and microdissection of the plaque, also lead to explosive exposure of procoagulants from vulnerable plaque and promote thrombus formation.9⇓–11 Plaque vulnerability was not evaluated in the present study, and we did not identify statistically significant variables that correlated to filter occlusion, possibly due to the small number of patients.
However, we believe that our data suggest some possible insights. Filter occlusion developed mainly in cases of severe stenosis, which could be associated with more plaque injury with balloon angioplasty. In 5 of 6 cases of filter occlusion, the patient had severe stenosis (≥90%). Filter occlusion occurred in 18% of the 28 cases of severe stenosis (≥90%), while it only occurred in 3% of the 33 cases of less severe stenosis. Moreover, though it did not reach a statistical significance, the presence of plaque ulceration also shows similar relations in terms of filter occlusion, with 5 of 6 patients in the filter-occlusion group having ulceration. This suggests to us that preformed or newly formed fibrin on plaque may be a major source of the filter occlusion.
The basic CAS technique used in this study was prestent dilation with relatively large-sized balloons, allowing the postdilation step to be skipped. This was done because poststent dilation has been known as a process in which the most emboli are released.12 We presumed that balloon inflation inside a stent would make the stent struts expand and lead to plaque shedding and, consequently, increased embolic risks. However, agreement on the best procedural technique is still lacking, and different sequences of the procedure may have different embolic risks. In a series of 53 cases, Bonaldi et al3 performed poststent dilation with 4.5–6 mm balloons and no predilation in most cases, and they reported approximately a 30% incidence of ICA flow arrest or stagnation. However, a controlled postmortem study suggests that the ballooning–stent placement sequence may not have critical importance in debris generation.13 Nevertheless, transcranial Doppler studies of microemboli suggest that ballooning generates frequent emboli.14,15
Comparison of different filters is beyond the scope of this study, but it is obvious that different designs of the porous and nonporous portions of the device would result in different filter action. For example, unlike membrane-type filters, the wire mesh–type filter has various porous regions. In an experimental study, Hendriks et al,16 observed that membrane filter devices caused a pressure gradient, which was not the case with the wire mesh filter.
Fibrin does not have a prefixed shape and size. It is gelatinous and semisolid. It can be chemically dissolved (thrombolysis), mechanically divided into fragments, or enlarged by fusion and squeezed out by force. Because fibrin is major embolic material,2⇓–4 its characteristics should be considered in developing more effective and safe filter devices. The surface area of the membrane, which has direct contact with blood flow, might need to be increased to reduce the risk of filter occlusion. For instance, the cone-shaped distal part of the filter, which collects embolic debris centrally, could be changed to taper more gradually.
The detection rate of visible debris in filters during CAS varies.2,17,18 Of course, the empty filter does not necessarily mean that no embolic event occurred.19 Very small emboli could pass through the filter pores, or filter apposition to the ICA lumen may not be perfect. Two filters in our series that caused ICA flow impairment were found to be empty. No other obvious cause that could produce ICA flow impairment except filter occlusion was seen. ICA spasm or dissections were not visualized. In addition, ICA flow arrest disappeared immediately after filter withdrawal. However, various filter-manipulation processes could affect the presence of debris in the filter. For example, encapsulating the filter into the retrieval catheter makes the filter collapse, so necessarily, debris gets mixed and moved and some could be squeezed out through the filter pores. In addition, some debris could be lost during the processes in which contaminants such as blood components are removed for better visualization. Manipulation for this procedure often includes washing, irrigating, shaking, squeezing, or dipping the filters in saline. To reduce the loss of debris, we adopted a technique that emphasized gentle and meticulous filter manipulation for inspection. Contaminants were removed from the inside of the filters with sharp forceps without saline irrigation or dipping, to minimize loss of the debris.
There are several limitations in this study. Technical inhomogeneities including types and sizes of balloons and stents, the lack of poststent dilation in the filter-occlusion group, and slightly different methods of filter manipulation after the procedures, could affect the results. In addition, variables that we examined such as stenosis severity, presence of ulceration, and timing of CAS after the last attack may not correctly categorize plaque vulnerability, which we think may be a factor for fibrin formation on the plaque surface during manipulation. Therefore, there may be missing variables that relate to filter occlusion. Finally, quantitative analysis of debris within filters was not performed.
Conclusions
ICA flow arrest due to filter occlusion during CAS is a significant technical drawback, which eliminates the advantage of preserving ICA flow with EPD use and could be an additional source of unexpected technical complications. The present study shows that filter occlusion during CAS is not rare. It occurred more frequently in cases of severe stenosis and despite full heparinization and antiplatelet therapy. Filter removal usually provides immediate and complete resolution of ICA flow arrest. Gross and microscopic examination demonstrated that pores of the filters were occluded mainly by fibrin. The occurrence of filter occlusion was not a risk factor for subsequent cerebral ischemia.
Footnotes
Disclosures: Michael Marks—UNRELATED: Consultancy: Cordis.
References
- Received May 4, 2011.
- Accepted after revision June 22, 2011.
- © 2012 by American Journal of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.