
Abstract
SUMMARY: Ipilimumab is a promising new immunotherapeutic antineoplastic agent with clinical activity in the treatment of metastatic melanoma and renal cell carcinoma. With advances in immunotherapy, however, a host of new side effects related to the mechanism of action of these drugs has appeared. At our institution, 3 patients presented with hypophysitis, which was attributed to an autoimmune process based on the documented relationship of the drug to other autoimmune phenomena and significant and rapid improvement with discontinuation of the drug and addition of steroids. We present the imaging findings in 3 patients with presumed ipilimumab-induced hypophysitis.
Ipilimumab, also known as MDX-010, is a human monoclonal antibody that has been shown to overcome the suppressive effects of cytotoxic T-lymphocyte antigen 4 expression, thereby enhancing the immune response against tumors.1 This drug has been shown in trials to have clinical activity against metastatic melanoma.2 Side effects are related to its mechanism of action, including development of immune-related adverse events such as hypophysitis, colitis, uveitis, dermatitis, and arthritis, among others.3 We describe 3 cases in which patients treated with ipilimumab developed both MR imaging and clinical findings characteristic of hypophysitis. We will describe these findings and provide a brief discussion of the causes and imaging characteristics of hypophysitis.
Case Reports
Case 1
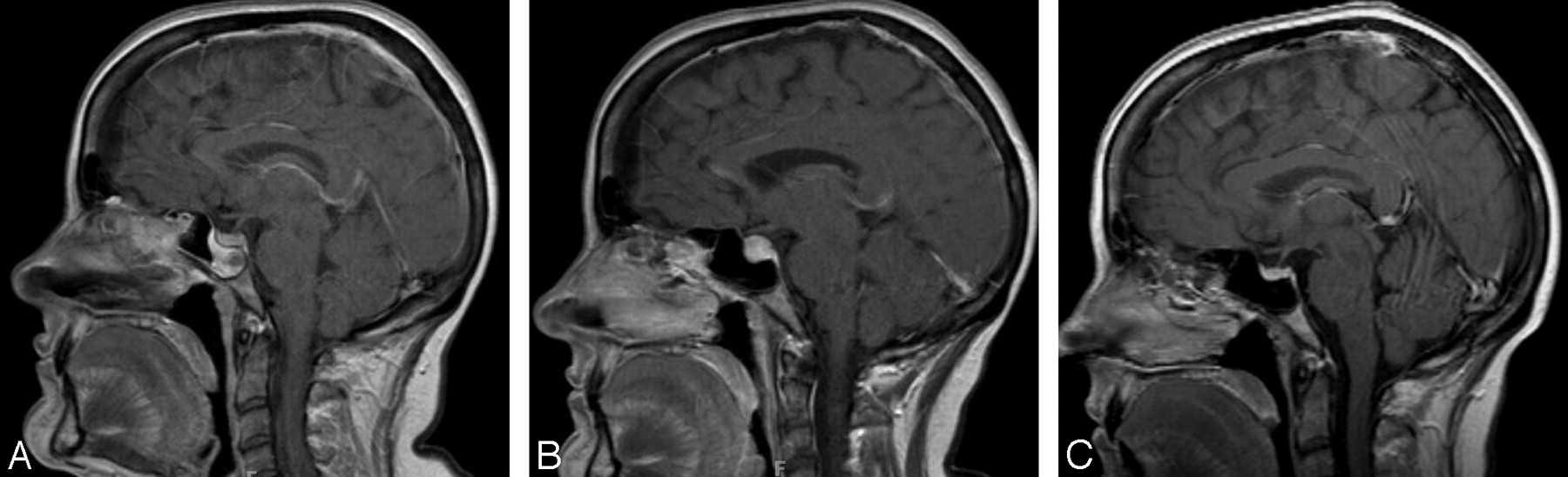
Patient 1 was a 70-year-old man originally diagnosed with a Clark level IV melanoma of the right shoulder, and later found to have cervical nodal metastasis. He was enrolled in an ipilimumab study and received 3 doses of antibody at 10 mg/kg for 6 weeks. Shortly after his third dose, he presented with complaints of visual hallucinations, lack of energy, dizziness on erect position, and anorexia. MR imaging revealed no evidence of metastatic disease but instead showed enlargement of the pituitary gland from the original baseline (from 5 mm craniocaudally to 12 mm). Laboratory studies disclosed the following values: a total T4 of 3.6 μg/dL (normal, 5.5–11.0 μg/dL) and a drop in adrenocorticotropic hormone (ACTH) from 21 to 9 pg/mL, thyroid-stimulating hormone (TSH) from 1.99 to 0.005 μL, and cortisol from 9.04 to 2.31 μg/dL compared with laboratory values obtained before initiation of therapy. He also had a total testosterone level <20 ng/dL with a decrease in luteinizing hormone and follicle-stimulating hormone (FSH). He received tapering doses of prednisone starting at 60 mg daily as well as levothyroxine (Synthroid) 50 mcg daily. Follow-up laboratory values and imaging showed improvement for several weeks following discontinuation of ipilimumab, along with corresponding improvement in symptoms on replacement therapy (Fig 1).

A, Postcontrast T1-weighted MR image of the brain during metastatic work-up demonstrates no metastatic disease. B, Postcontrast T1-weighted MR image of the brain obtained when the patient presented with visual hallucinations reveals diffuse enlargement of the pituitary gland. C, MR image shows resolution after discontinuation of the drug and initiation of hormone replacement.
Case 2
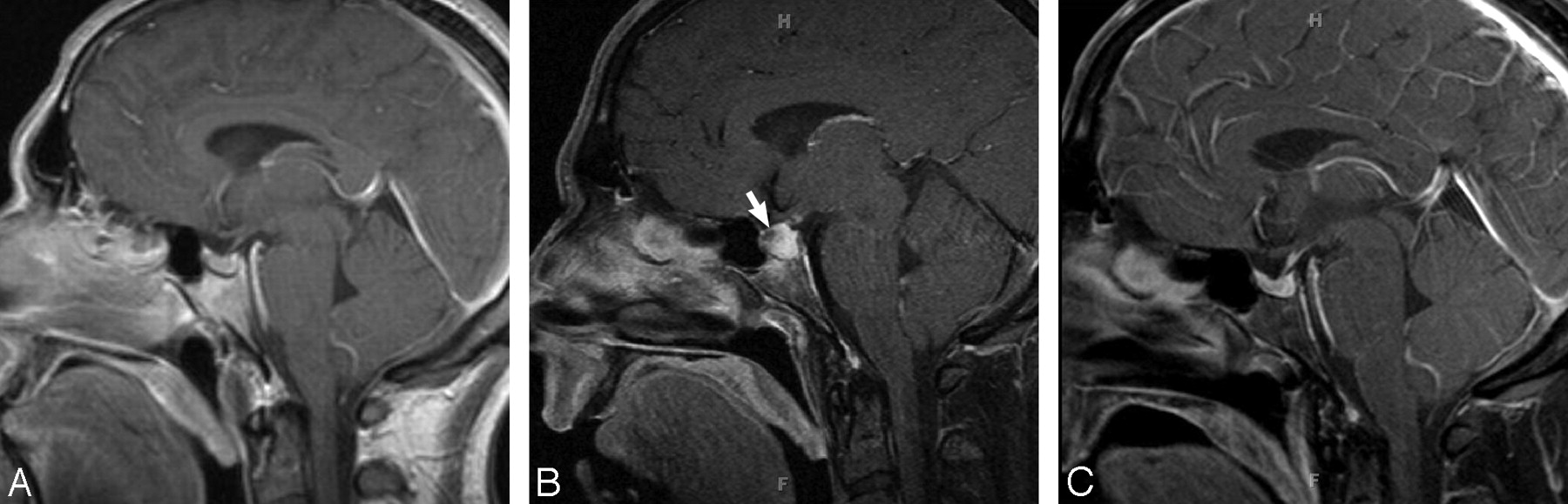
Patient 2 was a 44-year-old man with stage IV desmoplastic neurotropic melanoma found in the lower lip. He initially underwent excision and radiation therapy but was later found to have neurotropic spread along the maxillary division of the trigeminal nerve (V2). He was subsequently enrolled in an ipilimumab trial, receiving 10 mg/kg of the antibody every 3 weeks. Shortly after his third dose, he presented to the clinic with increased pain, nausea, alternating chills and hot spells, anorexia, and insomnia. MR imaging of the brain was performed for metastatic work-up, and he was found to have marked enlargement of the pituitary gland. Laboratory studies revealed the following values: ACTH of 26 pg/mL, cortisol of 5.2 μg/day, testosterone <20 ng/dL, and TSH of 0.060 μL. Ipilimumab was discontinued, and he was started on levothyroxine and a prednisone taper. At 1-month follow-up, he had both clinical and radiographic improvement but with persistent pituitary gland dysfunction (Fig 2).

A, Postcontrast T1-weighted MR image of the brain at initial metastatic work-up demonstrates a normal pituitary gland and stalk. B, Postcontrast T1-weighted MR image of the brain after several doses of ipilimumab reveals diffuse enlargement of the pituitary gland and superior displacement of the infundibulum. Note the area of heterogeneous enhancement (arrow). C, Postcontrast T1-weighted MR image after discontinuation of ipilimumab and initiation of steroid replacement shows that the pituitary gland has returned to baseline.
Case 3
Patient 3 was a 46-year-old woman with a history of stage IV melanoma with lesions in the gastrointestinal tract, subcutaneous tissue, and lungs. She also had a remote history of papillary thyroid cancer status post thyroid lobectomy. She was started on an ipilimubab protocol, receiving antibody at 10 mg/kg every 3 weeks. She presented to the clinic shortly after the third dose, complaining of severe headache and nausea. MR imaging of the brain revealed diffuse enlargement of the pituitary gland. Her cortisol level was found to be 12.0 μg/dL with a TSH level <0.003 μL and an FSH level of 18.7 MIU. Repeat laboratory values obtained 2 months later demonstrated a random cortisol level of <1 μg/dL. She was started on a prednisone taper and reported complete resolution of symptoms on a follow-up visit (Fig 3).

Postcontrast T1-weighted MR images at initial metastatic work-up (A), after the patient became symptomatic (B) and after discontinuation of the drug and appropriate hormone replacement (C).
Discussion
“Primary hypophysitis” is, by definition, of unknown etiology and is, therefore, classified on a histopathologic basis as lymphocytic, granulomatous, or xanthogranulomatous hypophysitis, whereas “secondary hypophysitis” is as a direct result of a systemic infectious or inflammatory processes or as a result of local processes such as a ruptured Rathke cleft cyst, craniopharyngioma, adenoma, or germinoma.4–6
MR imaging features of hypophysitis are nonspecific and are typically characterized by diffuse enlargement of the pituitary gland with loss of normal posterior pituitary signal intensity on the precontrast images and variable enlargement of the infundibulum. Enhancement is typically uniform but can be heterogeneous, as was shown in 3 of 5 patients by Ahmadi et al7 and 2 of 5 patients by Sato et al.8 Enhancement of the involved portions of the pituitary can be delayed as was shown originally in 1993 by Sato et al.9 This study showed lack of normal early enhancement of the posterior pituitary gland in patients with diabetes insipidus, thereby demonstrating a relationship between the function of the affected portion of the pituitary gland and its vascularity.
A similar study by Maghie et al10 showed delayed enhancement of both the anterior and posterior lobes of the pituitary gland in patients with hypopituitarism. Sato et al8 later studied this phenomenon in 1998, this time using dynamic contrast-enhanced imaging. In 5 patients with lymphocytic hypophysitis or lymphocytic infundibuloneurohypophysitis, they revealed a progressive decrease in enhancement with time, suggesting that the progressive decrease in vascularity was more likely secondary to chronic inflammatory changes with secondary vascular destruction, as opposed to a congenital process as was originally hypothesized.
We present 3 cases of presumed ipilimumab-induced secondary hypophysitis, supported by both clinical and radiographic findings. Symptoms in our patients were variable and included fatigue, insomnia, anorexia, hallucinations, and temperature intolerance. In 2 patients, symptoms of nausea and vomiting necessitated visits to the emergency department. Patients demonstrated laboratory findings consistent with panhypopituitarism, with significant decline in values of TSH, cortisol, and sex hormones from normal ranges. Contrast-enhanced MR imaging of the brain showed a marked increase in the size of the pituitary gland with respect to baseline studies. In 2 cases, the pituitary gland enhanced homogeneously, whereas in a third, there was heterogeneous enhancement. Follow-up imaging showed complete resolution of the abnormal findings, thereby supporting a diagnosis of a secondary immune-mediated process over metastasis to the pituitary gland. Clinically, all patients showed resolution of acute symptoms after discontinuation of the study drug and appropriate therapy with steroids, thyroid hormone, and sex hormone replacement. It remains to be seen how many will have persistent panhypopituitarism and require long-term hormone replacement.
Conclusions
Immunotherapy with antibodies that stimulate T-cell responses is a promising new treatment for patients with cancer. It is important that the radiologist be aware of the new and unique complement of side effects that are associated with these treatments. The imaging characteristics of hypophysitis are nonspecific and, on the basis of the imaging alone, often cannot be differentiated from other causes, including metastasis. Further investigation by the radiologist and the identification of characteristic clinical and laboratory findings can aid in making a confident diagnosis of autoimmune hypophysitis.
References
- Received February 19, 2009.
- Accepted after revision March 19, 2009.
- Copyright © American Society of Neuroradiology
In this issue









{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- MRI Findings of Immune Checkpoint Inhibitor-Induced Hypophysitis: Possible Association with Fibrosis
- Adrenal Insufficiency Related to Anti-Programmed Death-1 Therapy
- Ipilimumab Therapy for Melanoma: A Mimic of Leptomeningeal Metastases
- Long-term follow-up of ipilimumab-induced hypophysitis, a common adverse event of the anti-CTLA-4 antibody in melanoma
- ENDOCRINE SIDE-EFFECTS OF ANTI-CANCER DRUGS: mAbs and pituitary dysfunction: clinical evidence and pathogenic hypotheses
- Neurological immune-related adverse events of ipilimumab
- Ipilimumab and Its Toxicities: A Multidisciplinary Approach
- MECHANISMS IN ENDOCRINOLOGY: Ipilimumab: a novel immunomodulating therapy causing autoimmune hypophysitis: a case report and review