
Abstract
BACKGROUND AND PURPOSE: In progressive supranuclear palsy (PSP) and corticobasal degeneration (CBD), postmortem studies show different topographic involvement of the thalamus, basal ganglia, and their cortical connections. Diffusion tensor imaging (DTI) is an MR imaging technique sensitive to gray and white matter microstructure integrity. This study was performed to determine whether DTI may demonstrate microstructural differences between PSP and CBD, particularly within the thalamus and its cortical connections.
MATERIALS AND METHODS: Nine patients with probable PSP, 11 with probable CBD, and 7 controls formed the study group. Apparent diffusion coefficient average (ADCave) and fractional anisotropy (FA) values were measured in regions of interest positioned in the ventrolateral (motor), medial, anterior, and posterior regions of the thalami, basal ganglia, fronto-orbital white matter, cingulum, supplementary motor area (SMA), and precentral and postcentral gyri in patients and controls.
RESULTS: In PSP, ADCave values were increased in several areas: the thalamus, particularly in its anterior and medial nuclei; cingulum; motor area; and SMA. FA values were particularly decreased in the fronto-orbital white matter, anterior cingulum, and motor area. In CBD, ADCave was increased in the motor thalamus, in the precentral and postcentral gyri, ipsilateral to the affected frontoparietal cortex, and in the bilateral SMA. FA was mainly decreased in the precentral gyrus and SMA, followed by the postcentral gyrus and cingulum.
CONCLUSIONS: In patients with PSP, thalamic involvement was diffuse and prevalent in its anterior part, whereas in CBD involvement was asymmetric and confined to the motor thalamus. DTI may be useful in the differential diagnosis of these 2 parkinsonian disorders.
Progressive supranuclear palsy (PSP) and corticobasal degeneration (CBD) are pathologically distinct causes of progressive atypical parkinsonism poorly or not responsive to levodopa. Both disorders are characterized by τ protein (4R isoform) deposits in neurons and glia.1 However, the brain areas involved in the 2 conditions differ,2 mainly the cortex in CBD and the subcortical areas in PSP.3 Although diagnostic criteria are based on motor impairment, the clinical hallmarks of these conditions,4,5 in both disorders cognitive decline and behavioral abnormalities are always present and dementia is frequent.6,7
In PSP, anterior frontal lobe dysfunction is the most disabling cognitive deficit, partly due to marked deafferentation of the prefrontal areas, resulting from degeneration of striatothalamocortical pathways.8,9 The circuits implicated in behavioral control involve the thalamus, mainly the medial thalamus connected to the fronto-orbital cortex and the anterior thalamus connected to the cingulate gyrus.10
In CBD, cognitive and motor dysfunctions are frequent, and the most characteristic higher cortical disorders are limb-kinetic apraxia, ideomotor apraxia, and alien limb phenomenon, probably related to damage to the perirolandic regions.11 These cortical areas are functionally connected to the motor thalamus, a group of nuclei in the lateral part of the thalamus.
Conventional MR imaging in PSP shows midbrain atrophy, particularly the dorsal midbrain; signal intensity changes in the tegmentum and periaqueductal gray matter,12 and marked enlargement of the third ventricle, suggesting thalamic tissue loss.13 Recent studies with voxel-based morphometry (VBM) have confirmed thalamic atrophy and additionally report symmetric tissue loss in the orbitofrontal cortex and anterior cingulate cortex.14,15
Conventional MR imaging in CBD shows asymmetric cortical atrophy in the frontoparietal regions, which is worse contralateral to the clinically affected side; basal ganglia and thalamic involvement is rarely visible.7
Diffusion tensor imaging (DTI) measures the translational movement of water molecules in biologic tissues. It measures fractional anisotropy (FA), an index of white matter coherence and axonal packing, and apparent diffusion coefficient average (ADCave), an index of the average magnitude of the rate of diffusion within each voxel. A reduction in the linear organization of white matter pathways will determine a decrease in FA. White and gray matter damage, even at the microstructural level, will determine an increase in ADCave.
Postmortem pathologic studies have shown loss of neurons, with τ protein aggregates in the thalamus of both tauopathies; however, the topographic distribution of lesions differs between PSP and CBD.2
The aim of this study was to determine whether, in these diseases, DTI can detect a different distribution of microstructural tissue damage occurring in the thalamus, the basal ganglia, and their connections with cortical areas. Thus DTI metrics in the thalami could be used in the differential diagnosis of the 2 parkinsonian disorders.
Materials and Methods
Nine patients with PSP (5 women, 4 men; mean age, 66.5 years; range, 51–73 years), 11 patients with CBD (7 women and 4 men; mean age, 66.4 years; range, 51–77 years), and 7 healthy volunteer controls of an age as similar as possible to that of the patients (2 women and 5 men; mean age, 60.4 years; range, 55–66 years) were enrolled in this study. The controls had no history or signs of neurologic disease or cognitive disturbance and had normal brain MR imaging findings. For the MR imaging examinations, written informed consent was obtained from all participants.
Patients were diagnosed according to accepted clinical criteria4,5 and displayed typical features of the diseases. The Unified Parkinson's Disease Rating Scale (UPDRS III) was used to assess motor disability; the Mini-Mental State Examination (MMSE), to assess mental state. In patients with CBD, akinetic rigid syndrome and limb apraxia were more marked on the side contralateral to MR imaging–detected hemispheric atrophy and signal-intensity abnormalities (6 clinically worse on the right side, 5 on the left).
Imaging
A 1.5T MR imaging system (Avanto; Siemens, Erlangen, Germany) was used. Axial proton attenuation/T2-weighted images (TR = 3500 ms; TE = 17 and 84 ms; 5-mm thickness), coronal turbo spin-echo T2-weighted images (TR = 4100 ms, TE = 143 ms, 5-mm thickness), and axial gradient-echo T2 * -weighted images (TR = 700 ms, TE = 26 ms, 5-mm thickness) were obtained. Volumetric T1-weighted images were acquired by using a magnetization-prepared rapid acquisition of gradient echo sequence (160 sagittal sections, TR = 1640 ms, TE = 2.0 ms, TI = 552 ms, voxel size = 1 mm3, flip angle = 12°).
DTI was performed by using twice-refocused single-shot spin-echo echo-planar sequences in axial sections with the following settings: TR = 7500 ms, TE = 80 ms, NEX = 10, matrix = 192 × 256, FOV = 180 × 240 mm, section thickness = 2.5 mm, and no intersection gap. DTI was performed along 12 directions with a b = 1000 s/mm2. In addition, images without diffusion weighting were acquired corresponding to b = 0 s/mm2. Diffusion-weighted images were corrected for eddy current and then corrected for head motion by using the Linear Image Registration Tool software of the Centre for Functional Magnetic Resonance Imaging of the Brain (University of Oxford, Oxford, UK) with 12 df. The acquisitions were repeated 5 times to improve the signal intensity-to-noise ratio and subsequently averaged.
The conventional images were assessed jointly by 2 senior neuroradiologists (A.E., M.G.) for supratentorial and infratentorial atrophy and signal-intensity changes. Particular attention was paid to the presence/absence of bilateral/unilateral frontoparietal atrophy, ipsilateral ventricular dilation, third ventricle enlargement, cortical or subcortical signal-intensity abnormalities, basal ganglia atrophy, midbrain atrophy (with anteroposterior diameter measurement), and tegmental signal-intensity abnormalities. MR images of controls were assessed similarly.
Image Analysis
The tensor was estimated statistically by using a multivariate linear regression model assuming a monoexponential relationship between signal intensity and the product of the b matrix and diffusion tensor matrix components.16 ADCave and FA maps were calculated by using DTIStudio software17 (Johns Hopkins University, Baltimore, Md) and were measured within several regions of interest. Circular regions of interest were identified independently by the same 2 neuroradiologists on DTI color maps and on DTI echo-planar images with b = 0 s/mm2. The regions of interest were transferred to ADCave and FA maps. To minimize partial volume effects, we chose 2- to 4-mm-diameter regions of interest. In the deep gray nuclei, regions of interest were positioned bilaterally in the head of the caudate nucleus; in the central part of the globus pallidus and putamen; and in the anterior, medial, lateral (motor), and posterior thalamus, identified according to the Stereotactic Atlas of the Human Thalamus and Basal Ganglia by Anne Morel.18,19 More specifically, the region of interest placed in the anterior thalamus was positioned in the forward part of the nucleus close to the genu of the internal capsule, posterolateral to the anterior column of the fornix. The regions of interest in the medial and the motor thalamus were positioned in the same coronal plane of the corticospinal tract in the posterior limb of the internal capsule, close to the third ventricle and to the posterior limb of the internal capsule, respectively. The region of interest in the posterior thalamus was positioned 8–10 mm posterolateral to the motor thalamus.
White matter regions of interest were positioned in the superior cerebellar peduncle, lateral prefrontal and fronto-orbital regions, cingulum, white matter in proximity to the supplementary motor area (SMA), and white matter of the precentral (hand knob region) and postcentral gyri at the same distance off the midline. The following are more detailed positions: 1) In the prefrontal lateral region, regions of interest were located in the white matter of the frontal operculum in the inferior frontal gyrus; 2) in the fronto-orbital region, regions of interest were positioned in the white matter of the medial supraorbital gyrus; 3) the cingulum was evaluated in its anterior segment (in front of the genu of the corpus callosum) and posterior segment (behind the splenium), where the bundles run caudocranially and appear blue on the color map; 4) the SMA was identified as the parasagittal gyrus bounded posteriorly by the primary motor cortex and anteriorly by a coronal plane containing the vertical line intersecting the anterior commissure and perpendicular to the anteroposterior commissure plane.20 ADC values were measured in all the regions of interest, both in white matter and gray matter areas. FA measurements were obtained in the white matter and in the thalami because of their high content of white matter fibers. All region-of-interest positions are illustrated in Figs 1 and 2.
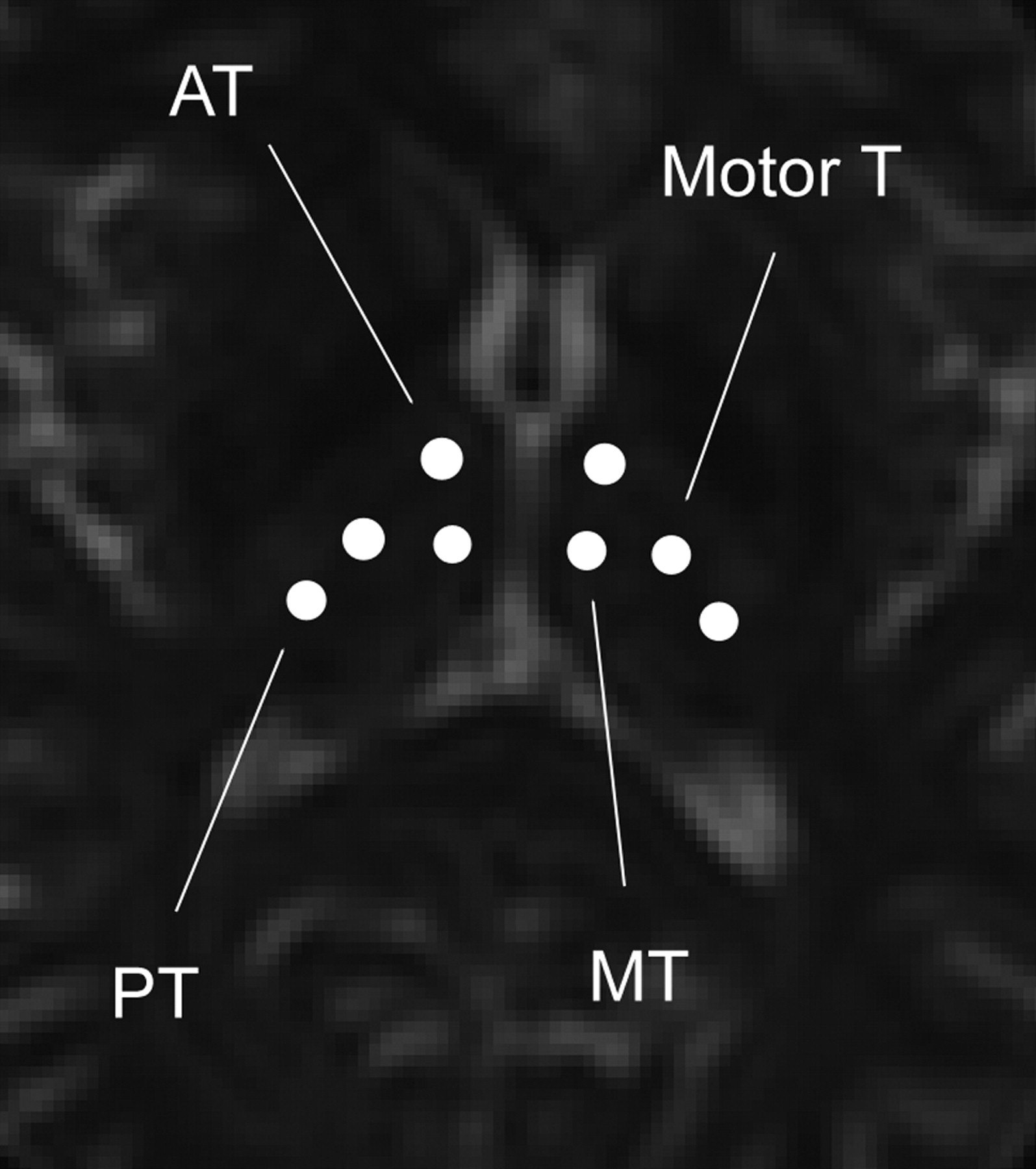
Positioning of regions of interest for ADC and FA measurement in the thalami. AT indicates anterior thalamus; motor T, motor thalamus; MT, medial thalamus; PT, posterior thalamus.

Positioning of regions of interest for ADC and FA measurement in the basal ganglia and white matter. CN indicates caudate nucleus; GP, globus pallidus; Pt, putamen; SCP, superior cerebellar peduncle; FO, fronto-orbital gyrus; IFG, inferior frontal gyrus; AC, anterior cingulum; PC, posterior cingulum; SMA, supplementary motor area.
Statistical Analysis
The difference in sex distribution between groups was evaluated by the χ2 test. Age differences were investigated by 1-way analysis of variance (ANOVA) followed by the Tukey correction. Differences in disease duration and UPDRS and MMSE scores were assessed by the nonparametric Mann-Whitney U test because of the small sample size. The inter-rater and intrarater reliability of ADCave and FA measurements was determined by intraclass correlation coefficients derived by using a 1-way random-effects ANOVA model. The inter-rater reliability was estimated on all scans. The intrarater reliability was estimated on 10 scans evaluated by the first rater. The values were then averaged, and the mean was used.
After confirming the absence of lateralization of ADCave and FA changes in patients with PSP and controls by a paired t test, we averaged measurements from the 2 hemispheres. For patients with CBD, measurements from each side were averaged for regions for which no differences between the 2 sides were found; otherwise the value of the most affected side (ie, the higher ADC ave and the lower FA value) was used.
One-way ANOVA with group as a factor, followed by the Tukey test for multiple comparisons, was used to assess differences in ADCave and FA measurements among the 3 groups after determining that the distributions of values were normal by the Shapiro-Wilk normality test. Differences were considered significant for P < .05. Results are reported as means and SDs. The analyses were performed with the Statistical Package for the Social Sciences, Version 13.0 for Windows (SPSS, Chicago, Ill).
Results
Demographics and clinical data of patients and controls are reported in On-line Table 1. The ANOVA did not show any significant difference in age between groups. The inter-rater and intrarater reliability analysis showed good agreement (r > 0.85, r > 0.83, respectively). The results of the statistical analyses of the selected brain regions for ADCave are reported in On-line Table 2 and for FA, in On-line Table 3.
Apparent Diffusion Coefficients
ANOVA showed significant differences among groups for ADCave in the caudate nucleus (F = 5.343, P = .012), globus pallidus (F = 3.952, P = .033), anterior (F = 7.433, P = .003), medial (F = 4.360, P = .024) and motor thalami (F = 7.713, P = .003), superior cerebellar peduncle (F = 4.503, P = .022), anterior (F = 3.542, P = .045) and posterior cingula (F = 4.085, P = .030), SMA (F = 7.416, P = .003), and precentral (F = 20.37, P < .001) and postcentral gyri (F = 12.51, P < .001).
In patients with PSP compared with controls, the Tukey test showed an ADCave increase in the head of the caudate nucleus (P = .015), globus pallidus (P = .026), anterior thalamus (P = .004), and medial (P = .049) and motor thalami (P = .015). The ADCave was also increased in the superior cerebellar peduncle (P = .04), anterior cingulum (P = .043), and posterior cingulum (P = .027), SMA (P = .045), and the precentral gyrus (P = .027).
In patients with CBD compared with controls, we found increased ADCave in the head of the caudate nucleus (P = .028), motor thalamus (P = .002), SMA (P = .002), precentral gyrus (P < .001), and postcentral gyrus (P < .001).
In the comparison between patients with PSP and CBD, we found higher ADCave values in patients with PSP in the anterior thalamus (P = .018), medial thalamus (P = .041), and the superior cerebellar peduncle (P = .042). Higher ADCave values were found in patients with CBD in the precentral (P = .004) and postcentral gyri (P = .021).
Fractional Anisotropy
ANOVA showed significant differences between groups for FA in the fronto-orbital area (F = 5.764, P = .009), anterior (F = 14.85, P < .001) and posterior (F = 5.263, P = .013) cingula, SMA (F = 7.19, P = .004), precentral gyrus (F = 29.032, P < .001), and postcentral gyrus (F = 4.760, P = .018). In patients with PSP compared with controls, the Tukey test showed that FA was lower in the fronto-orbital area (P = .007), anterior cingulum (P < .001), posterior cingulum (P = .012), SMA (P = .031), precentral gyrus (P < .001), and postcentral gyrus (P = .031). In patients with CBD compared with controls, we found that FA was lower in the anterior cingulum (P = .028), posterior cingulum (P = .047), SMA (P = .003), precentral gyrus (P < .001), and postcentral gyrus (P = .027). In the comparison between patients with PSP and CBD, we found that FA was lower in the anterior cingulum (P = .013) in patients with PSP.
Discussion
The most important finding of this study was that DTI metrics (ADCave) are sensitive enough to detect lesion topography differences in the thalamus between patients with PSP and CBD. The anterior and medial thalamic nuclei were involved only in patients with PSP. The motor thalamus was involved in both tauopathies, but abnormalities were asymmetric in CBD and symmetric in PSP.
Significant differences in ADCave and FA abnormalities were found also in other brain regions. The anterior cingulum—functionally connected to the anterior thalamus—was characterized by high ADCave and low FA in patients with PSP. The fronto-orbital region—functionally connected to the medial thalamus—was characterized by abnormally low FA in patients with PSP. Abnormal ADCave and FA values were measured in the primary motor cortex and SMA, which are functionally connected to the motor thalamus in both tauopathies. In the postcentral gyrus, FA was abnormal in both, whereas ADCave was increased only in patients with CBD. This study shows that DTI detects microstructural changes in vulnerable gray and white matter regions of patients with tauopathies, despite the absence of signal-intensity abnormalities on conventional MR imaging. Peculiar to this study was the demonstration that significant FA and ADCave abnormalities are found in anatomic brain regions that are known a priori to be functionally connected.
This study implies that pathologic changes such as the formation of τ protein aggregates and neuronal loss in the gray matter of patients with PSP and CBD result in elevation of the ADCave, probably due to diminished tissue organization, which represents microstructural barriers to diffusion of water in the interstitium. Decreased FA in white matter connecting affected gray matter regions may imply that loss of coherence, reduction of axonal packing, and demyelination have occurred, probably secondary to wallerian degeneration. In neurodegenerative diseases, decreasing FA has often been associated with elevation of ADCave, even though the 2 metrics measure different physical phenomena. Although in neurodegenerative diseases the ADCave is essentially related to the structure of the tissue and the amplitude of the extracellular spaces that limit the movements of the water molecules (and is therefore suitable to study both gray and white matter), FA depends on the limitation of the water motion in a certain direction because it occurs in anisotropic tissue, in which the white matter fibers have a prevalent orientation.
This study was the first to investigate regional analysis in the thalamus with DTI parameters. Two previous studies21,22 also demonstrated abnormally increased ADCave in the thalamus in comparison with that in healthy subjects but with a single large region of interest. Padovani et al21 found abnormally decreased FA in the bilateral posterior thalamic radiations and anterior thalamus.
In the 1990s, few detailed neuropathologic studies had examined the topographic distribution and density of neurofibrillary tangles in the thalamus of patients with PSP.23–25 Subsequently, the presence of large numbers of intracellular neurofibrillary tangles was demonstrated in the medial thalamus of patients with PSP, with similar but less pervasive involvement of the anterior thalamus.26 The anterior thalamic nuclei are connected to the cingulate gyrus, and the medial thalamic nuclei are connected to the fronto-orbital gyrus. These connections are part of the limbic circuits involved in behavioral control.10 Abnormalities in these circuits in patients with PSP may explain the apathy, reduced verbal fluency, and motor inhibition. Our findings of abnormal ADCave or FA values in the anterior and medial thalami and anterior cingulate gyrus and fronto-orbital regions are also consistent with morphometric abnormalities identified by VBM.14 Furthermore, they correlate well with the functional-anatomic models of the behavioral disturbances that characterize PSP.7
In accordance with Seppi et al,27 abnormally high ADCave in the head of the caudate nucleus was documented. The head of the caudate is connected to dorsolateral prefrontal areas and is a component of the striatothalamocortical circuits involved in executive functions, which are also compromised in PSP. We found, however, that ADCave and FA were normal in the inferior frontal gyrus, part of the dorsolateral prefrontal area, possibly due to the small size of the regions of interest compared with the region under analysis.
The globus pallidus is severely affected in PSP, mainly in its external part.28 Together with the ventrolateral and ventroanterior nuclei of the thalamus (motor thalamus), the globus pallidus participates in the motor circuit linking the basal ganglia to the motor cortex, premotor cortex, and SMA.28–31 Our findings, of abnormally high ADCave in the globus pallidus and lateral part of the thalamus, together with low FA in the primary motor cortex and SMA, are consistent with postmortem studies.32 Our findings in the primary motor area are also consistent with the results of other imaging studies.21,22,27,33 These abnormalities in multiple areas of the motor circuit may help explain motor dysfunctions such as kinetic apraxia, frequently observed in patients with PSP.34
ADCave abnormalities were not found in the putamen, despite its involvement in PSP. The anatomic architecture of the putamen and its connections are complex, and multiple region-of-interest analysis, such as that performed in the thalamus, may be necessary to identify selected topographic abnormalities.
As expected, we found abnormally high ADCave in the superior cerebellar peduncle only in patients with PSP, in line with imaging and postmortem studies showing atrophy.35 However, FA was not abnormal in this structure, suggesting that coherence and packaging of the bundles were preserved.
In this study, in CBD, abnormally elevated ADCave in the motor thalamus, precentral and postcentral gyri of the atrophic hemisphere and bilaterally in the caudate and SMA was shown. Abnormally low FA in the primary motor area, SMA, postcentral gyrus, and anterior and posterior cingulate gyri were shown. These findings are consistent with those in postmortem studies. Gross examination of the brain usually shows asymmetric atrophy of gyri most marked in pre- and postcentral regions, where swollen and vacuolated cortical neurons (ballooned neurons) and neurofibrillary tangles are found.36,37 Neuronal loss, gliosis, and neurofibrillary tangles also characterize lesions in the motor thalamus.38 Conventional MR imaging demonstrates asymmetric pericentral cortical atrophy in most cases, and hyperintensity of the atrophic cortex and underlying white matter may be seen on fluid-attenuated inversion recovery images.39 VBM studies have confirmed that cortical atrophy in the pericentral regions is clearly asymmetric in CBD and, in this respect, differs from that in PSP.40
Although conventional MR imaging investigations do not reveal thalamic involvement in CBD, fluorodeoxyglucose–positron-emission tomography and hexamethylpropyleneamine oxime–single-photon emission CT have shown asymmetric hypometabolism in the thalamus, precentral and postcentral gyri, and striatum.41 Our data delineate thalamic involvement in CBD in greater spatial detail, demonstrating abnormally high ADCave in the motor thalamus contralateral to the clinically affected side. We also found increased ADCave in the head of the caudate nucleus, but not in the putamen or in the globus pallidus. In view of abnormal ADCave and FA in the postcentral gyrus, we noted that ADCave was normal in the functionally connected ipsilateral posterior thalamus.
The distribution of the abnormalities observed in our patients with CBD is consistent with the clinical presentation characterized by cortical sensory disturbances, motor clumsiness, and limb-kinetic apraxia. Our results are also consistent with a DTI study42 in CBD that showed decreased FA in dorsolateral frontoparietal association tracts and in intraparietal (arcuate) bundles, despite substantial methodologic differences in data analysis. This study did not specifically evaluate DTI parameters in subregions of the thalamus, except for the pulvinar. A more recent diffusion study that evaluated only ADCave values demonstrated that hemispheric asymmetry was able to discriminate patients with CBD from those with PSP and Parkinson disease. However differences in the thalami did not reach statistical significance.43
Limitations
There are a few limitations in this study. Confirmation of clinical diagnoses with postmortem examinations was not available. The number of patients was small as expected in relatively rare diseases. Some of the regions that we evaluated, such as the inferior frontal gyrus, have significant crossing fibers. In future studies, more optimized DTI methodologies such as diffusion spectrum imaging may help to solve this problem.44 The use of greater magnet field strength (3T) and a greater than 12-direction protocol would also be of further advantage in future studies.
Conclusions
Despite these limitations, our study showed that DTI parameters are sensitive to selected tissue microscopic degeneration in distinct areas of the thalami and their white matter connections to the cortex. The spatial distribution of diffusivity alterations in the thalamus was different between patients with PSP and CBD. Thus DTI metrics may be useful in the differential diagnosis of these 2 parkinsonian disorders. However, evaluations of cognitive and behavioral disorders in a larger series of patients with PSP and CBD studied with DTI are necessary to establish more precise correlations between specific cognitive and motor dysfunctions and anatomic areas in which microstructural abnormalities are demonstrated.
Footnotes
-
indicates article with supplemental on-line table.
References
- Received January 13, 2009.
- Accepted after revision March 20, 2009.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- A Fully Automated, Atlas-Based Approach for Superior Cerebellar Peduncle Evaluation in Progressive Supranuclear Palsy Phenotypes
- The Role of Functional Dopamine-Transporter SPECT Imaging in Parkinsonian Syndromes, Part 2
- The Thalamus: A Small but Precious Window on {tau}-Related Neurodegeneration?
- Changes in the Thalamus in Atypical Parkinsonism Detected Using Shape Analysis and Diffusion Tensor Imaging
- Diffusion tensor imaging in parkinsonian syndromes: A systematic review and meta-analysis
- Abnormal Microstructure of the Atrophic Thalamus in Preterm Survivors with Periventricular Leukomalacia
- Gray and white matter water diffusion in the syndromic variants of frontotemporal dementia