
Abstract
BACKGROUND AND PURPOSE: Absolute ethanol was reported as an effective embolization of arteriovenous malformations (AVMs), but its use to treat AVMs in the mandible is not yet well established. Here, we present our clinical experience on treatment of mandibular AVMs with absolute ethanol.
MATERIALS AND METHODS: Eight consecutive patients with symptomatic AVMs of the mandible between August 2007 and September 2008 were enrolled in this study group. Among them, 6 patients underwent direct puncture embolization with absolute ethanol combined with coils, 1 patient underwent direct puncture embolization with absolute ethanol only, and the last patient had transarterial embolization with absolute ethanol alone. The use of coils decreased the flow and volume of the nidus, and then absolute ethanol embolization was directed against and obliterated the nidus completely. The procedure was performed with the patients under general anesthesia with nasal intubation, and the vital signs of the patients were constantly monitored during the injection of absolute ethanol. The total amount of absolute ethanol used per session was less than 1 mL/kg of body weight.
RESULTS: A total of 11 ethanol embolizations were performed on 8 patients, including 3 sessions with transarterial microcatheterization and 8 with direct puncture embolization. A venogram and control arteriogram performed immediately after the procedure were both obtained, which documented a significant thrombosis of the lesion in all patients. Follow-up examinations revealed that oral bleeding was controlled, the expansion of the external jugular vein in 5 cases was obliterated, and satisfactory shrinkage of the facial swelling was achieved. Follow-up angiography (mean, 4.2 months) was available in 4 patients, and there was no angiographic recurrence of the lesions. There were 3 cases with minor complications.
CONCLUSIONS: On the basis of our experience, treatment of AVMs in the mandible with absolute ethanol is a feasible, safe, and highly effective method.
Arteriovenous malformations (AVMs) of the mandible are very rare and may present a life-threatening hemorrhage spontaneously or after a tooth extraction. Transvenous embolization has been advocated either by direct transosseous venous puncture or transfemoral catheterization or through the mental foramen with permanent embolic agents such as coils and n-butyl-2-cyanoacrylate (n-BCA),1–5 but it has been reported that lesions treated with n-BCA and coils can recanalize,6 and rehemorrhage after recurrence and inflammation from extrinsic body is frequently encountered.1,4 In June 2007, W.F. Yakes was invited to present his clinical experience in management of craniofacial AVMs with absolute ethanol at the Chinese National Conference on Oral and Maxillofacial Vascular Anomalies held in Hanzhou, Zhejiang Province. On the basis of the reported experience of Dr. Yakes,6 we began to embolize mandibular AVMs with absolute ethanol. Here, we report 8 cases of intraosseous mandibular AVMs that were successfully embolized with absolute ethanol.
Materials and Methods
Patients
We obtained approval from the institutional review board of our hospital for a review and utilization of patient medical and imaging records. All patients provided written consent for the procedure after a discussion about the advantages and risks for the procedure. From August 2007 to September 2008, a total of 8 consecutive patients with symptomatic AVMs of the mandible were treated with absolute ethanol embolization (4 female patients and 4 male patients) in our department. The mean age was 23.5 years (age range, 13–43 years). Three patients had a history of unsuccessful operations and were no longer considered candidates for the procedure, 2 of whom also had undergone unsuccessful feeding artery embolization and ligation of the external carotid artery. In the remaining 5 patients, ethanol embolization was used as the primary treatment technique. Diagnoses of AVMs of the mandible were made on findings from clinical and imaging examinations. Oral bleeding was the main complaint in 6 of 8 patients, and paresthesia of the lower lip was recorded in 2 of 8 patients. The onset of the symptoms varied from childhood to adulthood. Prominent involvement of adjacent soft tissues was noted in 7 patients, and expansion of the external jugular vein in 6 patients. Five patients were treated electively, and the remaining 3 patients were treated on an emergent basis in which hemorrhage was brought under control by occlusion pressure. Patient 1 had recurrent lesions after embolization with coils and was given n-BCA 2 years ago and progressed bilaterally. The data of CT scan and panorama were available before embolization. The patients’ clinical and imaging data are summarized in Table 1.
Clinical and imaging data of 8 patients with AVMs in the mandible
Embolization Technique
All procedures that involved the use of absolute ethanol were performed with the patients under general anesthesia with nasal intubation. The placement of a Swan-Ganz catheter was not used to monitor the pulmonary arterial pressure during the ethanol injection because of the aggressive procedure and high cost. The blood pressure, electrocardiogram, oxygen saturation, and end-tidal carbon dioxide level were constantly monitored during the injection of absolute ethanol. Foley catheters were inserted after induction of anesthesia to monitor the state of hydration and the presence of hematuria. Baseline digital subtraction angiography was done in the same fashion as embolization. The high-flow vascular lesion was confirmed on the angiogram for each patient. Selective digital subtraction angiographic images were obtained to delineate the anatomy of the nidus and the timing of blood flow through the nidus. Ethanol embolization was directed against the nidus itself, not against the vascular feeders; the goal was to embolize all or part of the nidus until the desired clinical results were achieved. Transarterial embolization with the use of a coaxial catheter and/or direct-puncture embolization was required to reach the nidus for embolization. Routes of vascular access to attack the nidus were chosen according to the initial angiogram and CT scan. Direct-puncture embolization was indicated in patients with both unilocular radiolucency on CT scan and varix formation on the angiogram, and in those patients who had a history of a ligated external carotid artery. Transarterial embolization through the inferior alveolar artery with absolute ethanol was performed in 1 patient, direct puncture embolization with absolute ethanol was applied in 1 patient, and direct-puncture embolization with absolute ethanol combined with coils was used in 6 patients. The venous pouch was directly punctured with a 16G needle (Lichtwitz antrum needle; MEDICON, Tuttlingen, Germany). Stainless-steel coils with attached synthetic fiber coils (Cook, Bloomington, Ind) were released first, resulting in a decrease of arteriovenous shunt surgery flow, and then absolute ethanol was injected through this needle to occlude the AVM completely.
In 5 patients without ligation of the external carotid artery, the remaining filling of the mandibular vein was evident on the control arteriogram after direct-puncture embolization; additional ethanol embolization through the inferior alveolar artery was also given to obliterate AVM shunts. Patient 5 had multilocular radiolucency on CT scan and diffuse capillary blush with expansion of the jugular vein on the arteriogram; therefore, direct-puncture embolization could not be performed. The maxillary artery was catheterized with a 5F guiding catheter (Envoy; Cordis Endovascular, Miami Lakes, Fla), and a 3F microcatheter (Masstransit; Cordis Endovascular) was navigated into the distal end of the inferior alveolar artery. When AVM shunts were verified in the arteriogram, repeated injection of absolute ethanol was performed. Once any increase in blood pressure was found, ethanol injection was stopped until the monitored parameters returned to baseline levels. The amount of ethanol used during embolization was based on the amount required to fill the portion of AVMs being treated. Ethanol was manually injected after several test injections with contrast material to determine the hand pressure required and the amount of ethanol to inject. After ethanol injections, we waited for 10 minutes and then acquired an arteriogram to determine whether the therapy was successful. The total amount of absolute ethanol used per session was less than 1 mL/kg of body weight.
To minimize swelling and accompanying pain, all patients received an intravenous injection of dexamethasone before the procedure, usually 10 mg for adults and 3 to 10 mg for children, depending on their body weight. Postoperative management consisted of use of dexamethasone and intravenous infusion. Patients with gastrointestinal tract sensitivity to steroids can also be given ranitidine (Zantac) to protect against development of gastric or duodenal ulcer. Patients were usually observed in the intensive care unit overnight. The following medications usually include a tapering dose of corticosteroids for 7 days and ranitidine management to prevent ulcer development, if required.
Evaluation of Clinical Data and Follow-up Results
Two radiologists analyzed by consensus the therapeutic responses to ethanol embolization by comparing the degree of AVM devascularization (ie, 100%, 76%–99%, 50%–75%, or < 50%) between baseline and final angiography. Two oral and maxillofacial surgeons and 1 interventional radiologist evaluated by consensus the clinical outcome of symptoms and signs (ie, resolved completely, improved, no change, or aggravated) and complication. Complications were classified as either major or minor. Major complications included death, permanent adverse sequelae, and requirement of major therapy. Minor complications included any nonpermanent adverse sequelae, such as transient nerve injuries or spontaneously healed skin injury. Patients were physically and neurologically examined before and after embolization to assess complications. When complications were observed, we reviewed the angiograms again to find the possible cause of the complications.7
Periodic (1–3 months) follow-up evaluation was performed on the basis of physical examination, panorama, and enhanced CT scan. Results of the follow-up evaluation were analyzed by consensus. As a rule, additional embolization was recommended if the symptoms and signs remained or if the AVMs were still present at follow-up imaging. Clinical follow-up after the last treatment session was performed in all patients and ranged from 1 to 8 months. Results from imaging follow-up were available from the last treatment session in only 7 patients.
We established therapeutic outcomes by evaluating the clinical outcome of symptoms and signs and the degree of devascularization at angiography. Cure was defined as the resolution of oral bleeding, shrinkage of soft tissue with involvement, and obliteration of the expanded external jugular vein, with 100% devascularization of the AVMs at angiography. Partial remission was defined as complete resolution or improvement of the clinical symptoms and signs, with 50% to 99% devascularization of the AVMs at angiography. No remission was defined as improvement or no change of the clinical symptoms and signs, with less than 50% devascularization of AVMs at angiography. Aggravation was defined as an aggravation of the clinical symptoms and signs, regardless of the degree of devascularization of AVMs at angiography. Cure and partial remission were considered effective therapeutic outcomes of ethanol embolization of mandibular AVMs.
Results
Limited blood loss occurred during this procedure. The needle was removed, and manual pressure on the puncture site was performed for 5 minutes until there was no more oozing or bleeding. The acute oral bleeding was controlled just after embolization. The patients’ postoperative recovery was uneventful. Patients exhibited focal swelling in the area of the AVMs after the procedure, which resolved within 2 weeks.
During the 11 ethanol embolizations performed, the amount of ethanol that was used ranged from 28 to 50 mL in a single embolization session. When maximal amounts of ethanol were used, the total dose did not exceed 1 mL/kg of body weight. No patients experienced ethanol toxicity. Hemoglobinuria occurred in 6 of 8 patients of a total of 9 of 11 procedures and disappeared 5 to 6 hours later after continuous intravenous infusion; no patients showed an elevation in creatinine and urea levels.
With regard to the therapeutic outcome of ethanol embolizations, 6 of 8 patients were cured, and 2 had partial remission and were waiting for additional sessions of ethanol embolization to treat residual AVMs in the adjacent soft tissue. The number of required embolization procedures varied from patient to patient depending on the volume, behavior of the lesion, and whether there was involvement of adjacent soft tissue. A single embolization was usually sufficient to achieve cure of intraosseous AVMs, and the involvement of adjacent soft tissue required multistage embolizations. In the patients who needed 2 or more procedures, the interval between the procedures ranged from 2 to 3 months. The immediate venogram and control arteriogram after the procedure were both obtained and documented a significant thrombosis of the lesion in all patients. In high-flow AVMs, ethanol can quickly wash through toward the venous side and lose its thrombogenic properties. The follow-up arteriography study of 4 patients revealed occlusion of the nidus inside the mandible. Obvious expansion of the external jugular vein in 5 patients was obliterated after 1 session of ethanol embolization. Satisfactory shrinkage of facial swelling and improvement and/or loss of the pseudo-port-wine stain of the skin were obtained in 5 patients with involvement of adjacent soft tissues. The amount of ethanol used and results of treatment in 8 patients with AVMs of the mandible are summarized in Table 2.
Amount of ethanol used and results of treatment in 8 patients with AVM of the mandible
Complications
There were 3 of 8 patients who had minor complications, and there was no procedure-related mortality. Minor complications included skin necrosis, pyogenic granulomas from the puncture point, and localized necrosis of alveolar bone. A case of skin necrosis was healed with a wound dressing, and a skin graft was not required; the pyogenic granuloma from the puncture point in the buccal skin shrunk spontaneously after more sessions of embolization. In the last patient with minor complications, dehiscence of oral mucosa and exposure loosening alveolar bone with localized necrosis were noted 5 weeks after ethanol embolization. The necrotic alveolar bone was extirpated, and the mucosa was closed primarily with 3–0 chromic suture. The subsequent postoperative course was uneventful.
Illustrative Cases
Case 1.
A 16-year-old boy was admitted with repeated oral bleeding. He presented with a pulsatile swelling face and obvious expansion of the external jugular vein in the left side. CT scan demonstrated unilocular radiolucency in the body and ramus of the left mandible (Fig 1). An angiogram of the left external carotid artery showed varix formation in the mandible, and the inferior alveolar artery fed the lesion predominantly (Fig 2). The venous pouch was punctured directly with a 16G needle (Lichtwitz antrum needle; MEDICON) transosseously, after verification of placement of the needle through a venogram (Fig 3), 0.038–8–15 × 10 and 0.035–5–8 × 18 stainless-steel coils with attached synthetic fibers were released and resulted in a decrease of arteriovenous shunt surgery flow, and then absolute ethanol was injected through this needle to occlude the AVMs (Fig 4). In the later control arteriogram of the external carotid artery, the remaining filling of the mandibular nidus was found, and another 8 mL of absolute ethanol through the inferior alveolar artery was injected via a transcatheter approach to obliterate the AVM shunts completely (Fig 5). The total amount of absolute ethanol used was 50 mL. Follow-up angiograms after 10 weeks showed complete occlusion of the nidus in the mandible (Fig 6).

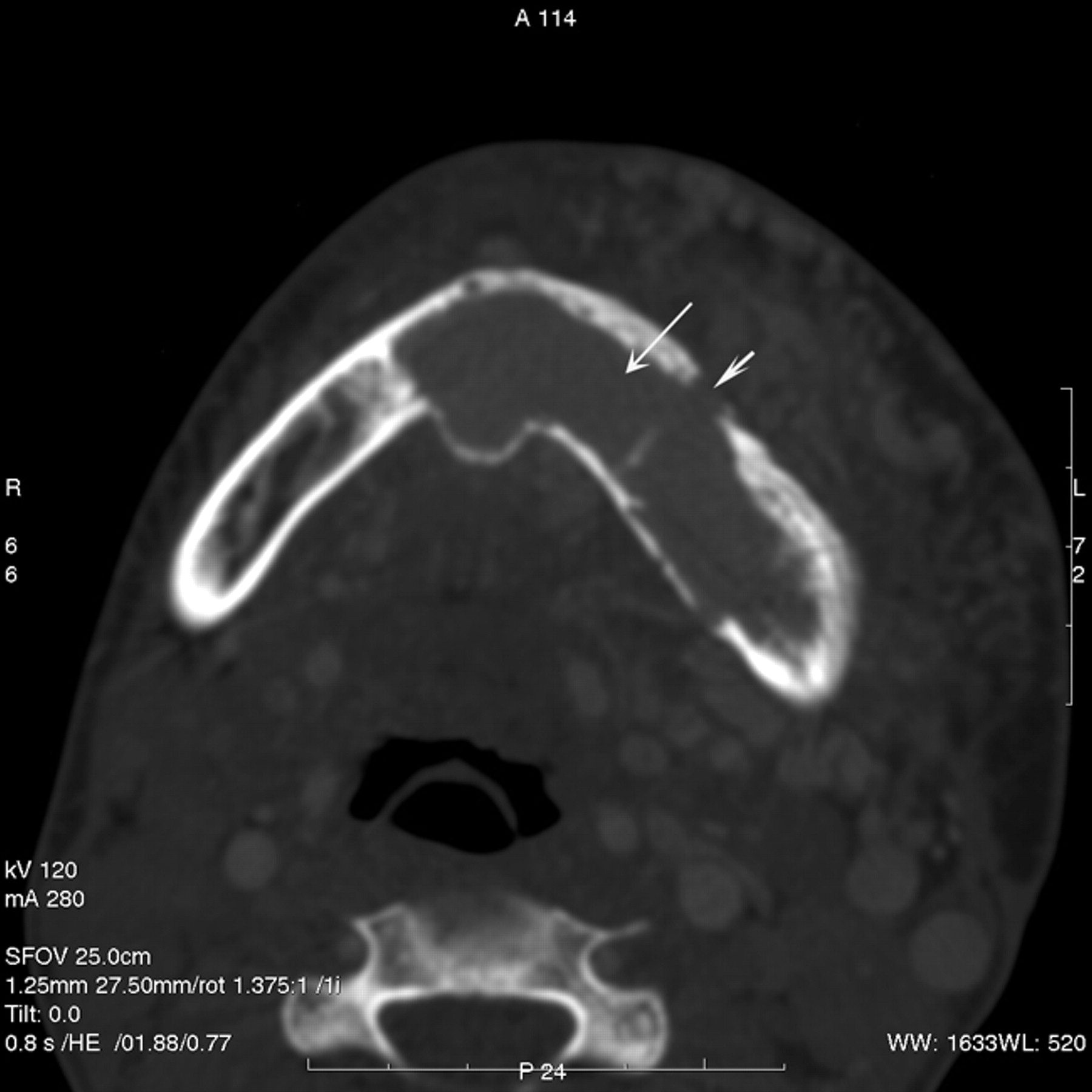
Axial CT scan demonstrated unilocular radiolucency (arrow) in the mandible with an expanded mental foramen (arrowhead).
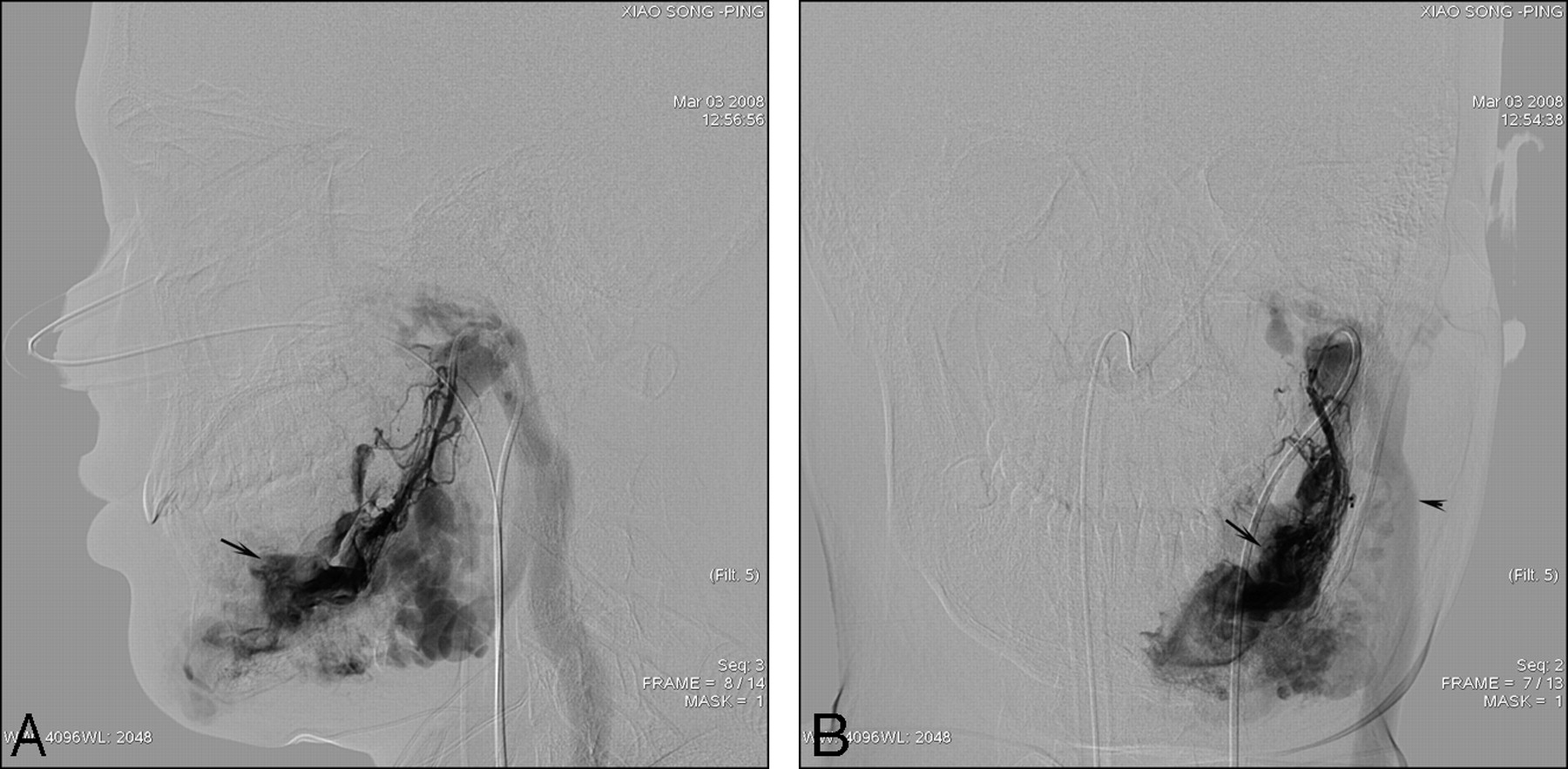
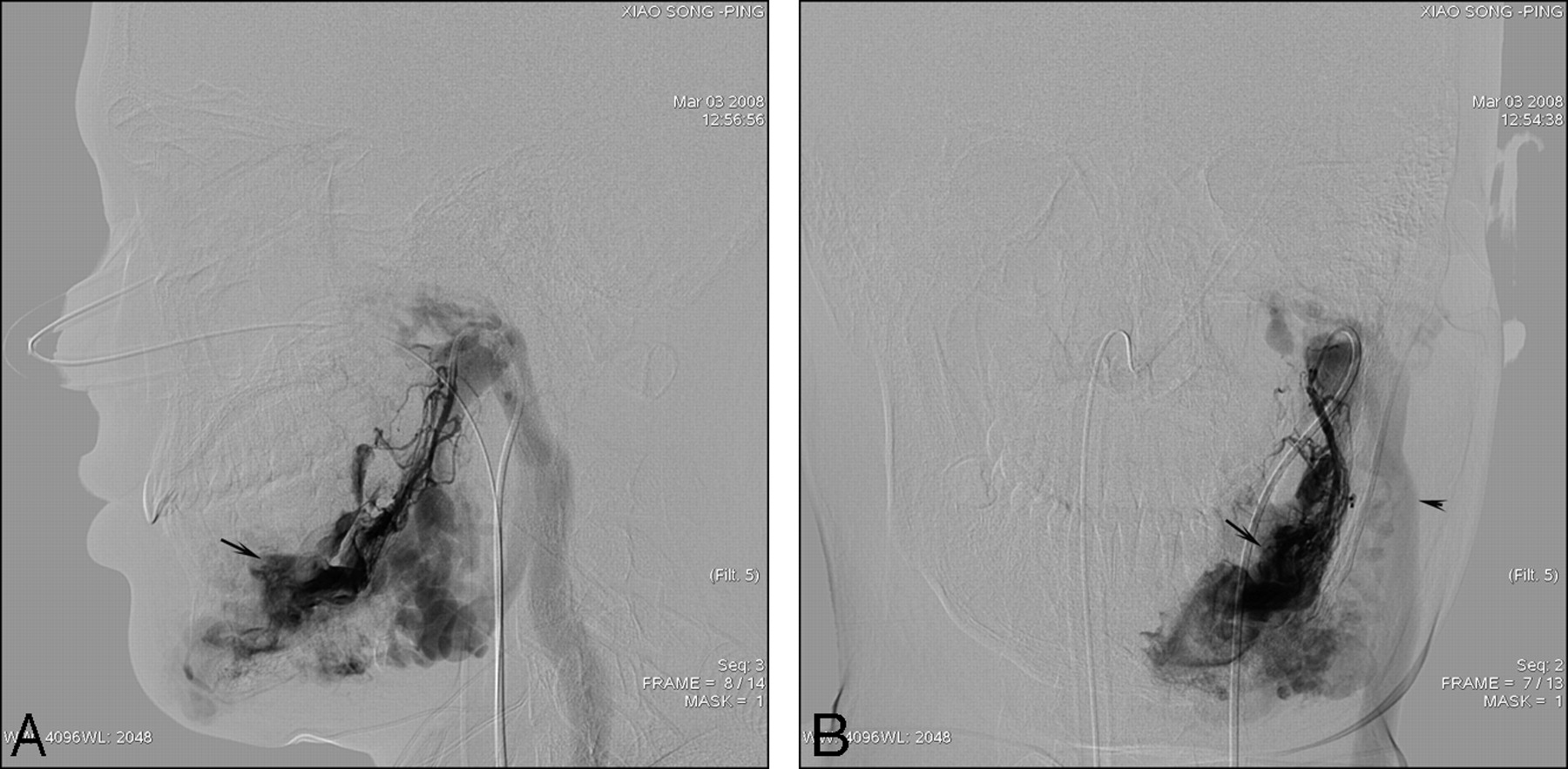
A, The lateral view of the angiogram of the inferior alveolar artery in the left side demonstrated varix formation (arrow) and expansion of the jugular vein (arrowhead). B, The varix (arrow) and expansion of the jugular vein (arrowhead) were noted on the posteroanterior view of the angiogram of the inferior alveolar artery.

The position of the 16G needle into the varix (arrow) was verified on the venogram as the demonstration of the drainage vein (arrowhead).

Venogram through the needle revealed some residual arteriovenous shunt surgery around the coils (arrow), and absolute ethanol was injected to obliterate the residual AVMs through the needle after release of the coils.

The control arteriogram of the inferior alveolar artery demonstrated the remaining filling of the mandibular nidus, and additional absolute ethanol was injected via a transcatheter approach.

Follow-up angiogram after 10 weeks showed complete occlusion of the nidus (arrow) in the mandible.
Case 2.
A 17-year-old girl was referred to the emergency department because of serious oral bleeding. Multilocular radiolucency of the left mandible was noted on CT scan (Fig 7). Left angiograms of the external carotid artery revealed diffuse capillary blush with early drainage vein within the mandible (Fig 8). Direct-puncture embolization could not be performed. The external carotid artery was catheterized with a 5F guiding catheter (Envoy; Cordis Endovascular), and a 3F microcatheter (Masstransit; Cordis Endovascular) was navigated into the distal end of the inferior alveolar artery (Fig 9). When AVM shunts were verified in the arteriogram, repeated injection of absolute ethanol was carried out until the drainage vein was obliterated. The total amount of absolute ethanol used was 50 mL. Follow-up angiograms after 3 months showed complete occlusion of the AVM shunts in the mandible (Fig 10).

Axial CT scan of the mandible demonstrated multilocular radiolucency (arrow).

The diffuse capillary blush in the mandible with expansion of the jugular vein was demonstrated on the angiogram of the inferior alveolar artery.

A 3F microcatheter was navigated into the distal end of the inferior alveolar artery, and ethanol injection was given via a transcatheter approach.

The control arteriogram after the procedure documented a significant thrombosis of the lesion.
Discussion
AVMs of the mandible are rare and challenging entities. Occlusion of the varix of the AVM with coil packing or n-BCA injection has been successful in some cases, but rehemorrhage after recurrence and inflammation from the extrinsic body is frequently encountered.1,4 The action of embolic agents provided by particles, coils, and n-BCA seem to be a simple vascular occlusion, but these agents cannot completely destroy the endothelial cells of the AVMs.8 The endothelial cell, when intact during thrombosis, senses decreased oxygen tension and sends out an angiogenesis factor that stimulates neovascular formation. Moreover, it sends out chemotactic factors that cause a cellular infiltration to carry debris from the vascular channels. Once this mechanism occurs, the endothelial cell is re-endothelialized and recanalization occurs.9 With the use of absolute ethanol, the endothelial cell is denuded from the vascular wall, its protoplasm is precipitated, and there is a fracture in the vascular wall to the level of the internal elastic lamina. In AVMs, these changes are desirable and account for the curative effects and permanence of ethanol embolization.10
It was usually believed that intravascular ethanol therapy would be far too hazardous for general use. However, in 1996, Yakes et al9 described curative treatment of an extremity AVM with absolute ethanol. Nontarget embolization with ethanol will lead to tissue necrosis as capillary beds are entirely destroyed. Being a fluid agent, ethanol penetrates to the capillary level, devitalizing normal tissues.11 Although the adverse effect of ethanol on the jaw bone is minimal, as seen in the numerous reports with use of ethanol injection via the foramen in management of trigeminal neuralgia,12 it was noted in our study group that the overdose injection of ethanol at one point may cause localized necrosis of alveolar bone. The total maximal dose that can be given in an embolization procedure in 1 day to a patient is 1 mL/kg body weight.13 Technical intraprocedural requirements for the use of ethanol include superselective catheter placement or direct deposition of ethanol within the nidus of the vascular lesion so as to avoid injection of ethanol into healthy vessels and tissues, use of general anesthesia with appropriate intraprocedural monitoring, good immediate postoperative care including appropriate use of medication to reduce any postoperative adverse effects, and careful clinical follow-up with appropriate re-do therapy when necessary to produce maximal benefit for the patients.
Fiber coils were preferred in our experience because of the safety and more efficient induction of clotting, but there are also some disadvantages, such as difficulty in filling the nidus completely and inability to destroy the endothelial cells of the lesion. When fiber coils were combined with additional injection of absolute ethanol, the volume and flow of the nidus in the mandible was decreased immediately, and then the endothelial cells of the lesion were destroyed. The decreased volume of the nidus with coils makes it possible to treat the AVMs of the mandible in 1 embolization session within the limit of the maximal amount of ethanol used. The involved adjacent soft tissues by the AVM of the mandible were also improved to a great extent after ethanol embolization, including reduced facial swelling and improvement and/or loss of the pseudo-port-wine stain of the skin.
On the basis of a comparative study of clinical manifestation, conventional radiology, and CT scan of AVMs of the jaw, we found that AVM of the mandible can be divided into 2 subgroups, which is of clinical significance.14 The first group demonstrated unilocular radiolucency on CT scan and obvious varix on arteriography, which can be well treated by direct puncture embolization of the varix. On the contrary, the second group had multilocular radiolucency on CT scan and diffuse capillary blush in arteriography, so direct puncture embolization was difficult to undertake (because of lack of varix); therefore, transarterial embolization was the preferred treatment option.
Conclusions
Despite some potential problems with ethanol embolization, we are now confident about ethanol use in the management of AVM of the mandible. Through transarterial embolization or direct puncture embolization, the varix within the mandible can be reached and completely obliterated in 1 or several sessions by controlled delivery of absolute ethanol.
Footnotes
Drs. Xin Dong Fan and Li Xin Su contributed equally to this work.
References
- Received September 30, 2008.
- Accepted after revision December 31, 2008.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Interventional management of high-flow craniofacial vascular malformations: a database analysis and review of the literature
- Head and Neck Arteriovenous Malformations: Results of Ethanol Sclerotherapy
- Hemostasis and obliteration of mandibular arteriovenous malformation through direct hydroxyapatite cement injection into the molar cavity