
Abstract
SUMMARY: A patient with suspected giant cell arteritis and prior negative findings on superficial temporal artery biopsy was evaluated with 320-detector row CT angiography (CTA) and whole-brain perfusion. Corticosteroid treatment was initiated on the basis of CT angiography findings of arteritis and a cortical perfusion deficit. The patient's symptoms and perfusion imaging findings resolved following therapy. Whole-brain CTA and imaging was helpful in the diagnosis and monitoring this patient with suspected vasculitis.
Large vessel cerebral vasculitis (LVCV) represents involvement of the internal carotid artery (ICA); intracranial vertebral arteries; the basilar artery; and the M1, A1, and P1 segments of the middle, anterior, and posterior cerebral arteries (MCA, ACA, and PCA, respectively).1 There is a wide range of diagnostic imaging strategies for patients with clinically suspected LVCV, including multidetector CT (MDCT), MR imaging, positron-emission tomography (PET), and Doppler sonography.2 Three-hundred-twenty−detector row CT enables whole-brain perfusion CT (PCT) and quantitative measurements of regional cerebral blood flow and volume (rCBF and rCBV). Such perfusion imaging potentially allows rapid reliable visualization of the effects of cerebral autoregulation mechanisms in parenchymal ischemia.
Combined with CT angiography (CTA), PCT has demonstrated clinical utility in acute ischemia.3,4 The major drawback of PCT to date has been the limited volume coverage achieved with 64-section CT imaging.3 The 320 × 0.5 mm detector configuration overcomes this limitation and enables assessment of the entire brain using iodinated contrast opacification for a period of time, so-called “dynamic volume CT.” The specific advantage in vasculitis is that abnormalities may not follow vascular distributions, requiring whole-brain PCT to identify all findings. We report a patient who underwent dynamic volume CT before and after treatment for suspected LVCV.
Case Report
A 39-year-old right-handed man presented with a left temporal headache, which did not have specific aggregating or relieving factors. The physical examination findings were normal, with the exception of absent reflexes in the right biceps. Pertinent signs included an elevated erythrocyte sedimentation rate (ESR) of 106 mm/h, a C-reactive protein level of 8 mg/L, and a borderline white blood cell count of 11,000 cellsμL/ mm3. The patient had normal findings on CSF analysis. The medical history was significant for left-sided headaches and a negative prior biopsy of the left superficial temporal artery (STA) for suspected giant cell arteritis (GCA). The differential diagnosis included primary headaches, vasculitis, transient ischemic attack, and impending stroke.
Dynamic volume CT (AquilionONE; Toshiba, Tochigi-ken, Japan) was performed during infusion of 70-mL iodinated contrast media (ioversol, Optiray 350; Mallinckrodt, St. Louis, Mo) at 5 mL/s. Single-rotation whole-brain volume datasets were acquired (80 kV, 100 mA, 1-second rotation) intermittently in 2 stages (Fig 1).
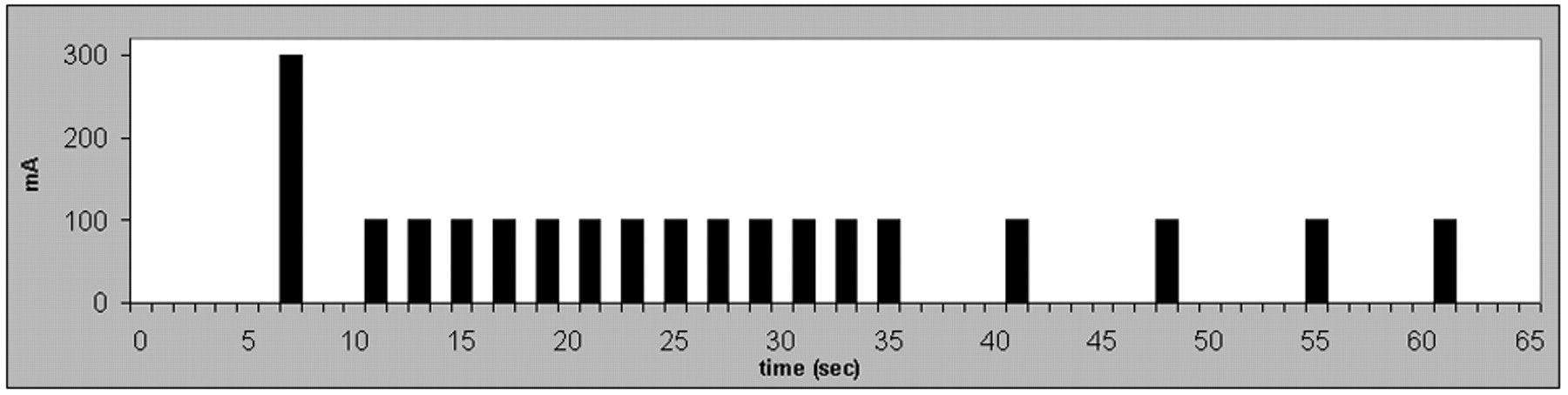
Timing diagram of 320-detector row whole-brain imaging. Each acquisition, represented by a black bar, has a 1-second duration. Time 0 refers to the initiation of iodinated contrast. The 300-mA “noncontrast” acquisition at 7 seconds, while contrast is in the central veins, is for a high signal intensity–to-noise subtraction mask. The subsequent 13 acquisitions have a 1-second interspacing to measure the contrast arrival time, the upslope, and the shape of the contrast peak. The last 5 acquisitions have 5 seconds of separation as contrast washes out of the brain parenchyma.
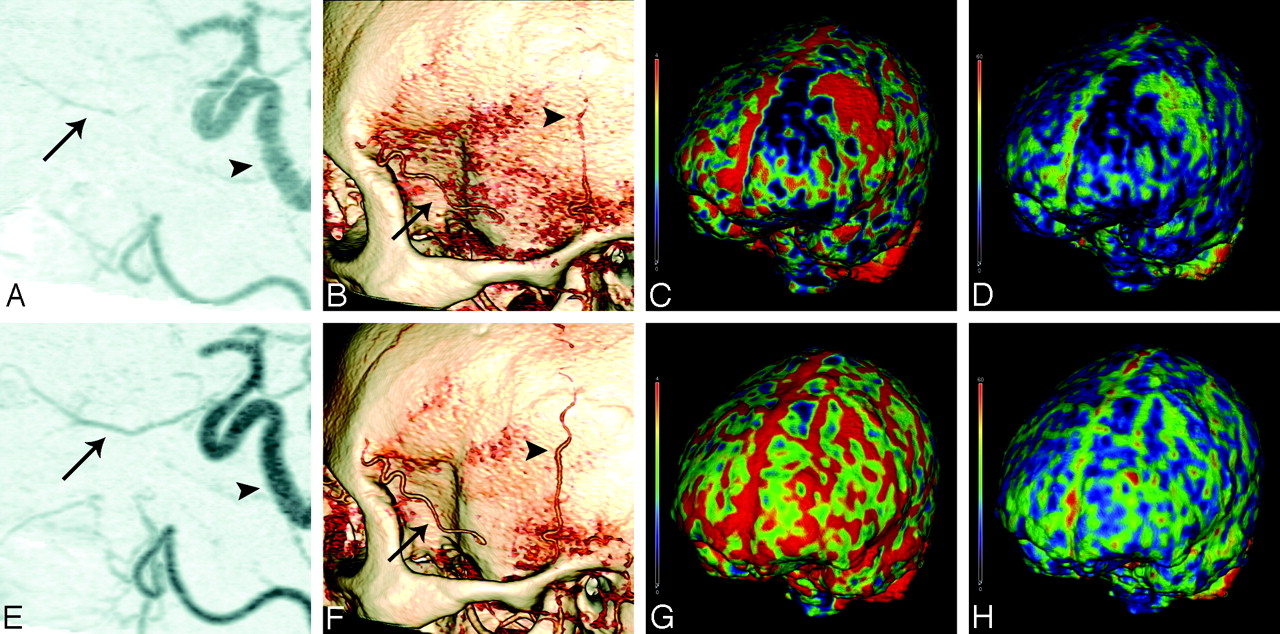
CT demonstrated tortuosity and beading of the ICA and narrowing and beading of the ophthalmic artery (Fig 2A) and STA (Fig 2B). Perfusion images illustrated reduced rCBV and rCBF, consistent with large vessel arteritis (Fig 2C, -D). Corticosteroid therapy was initiated. After 2 weeks of treatment, the patient reported resolution of symptoms, and the CTA and PCT findings dramatically improved (Fig 2E−H).
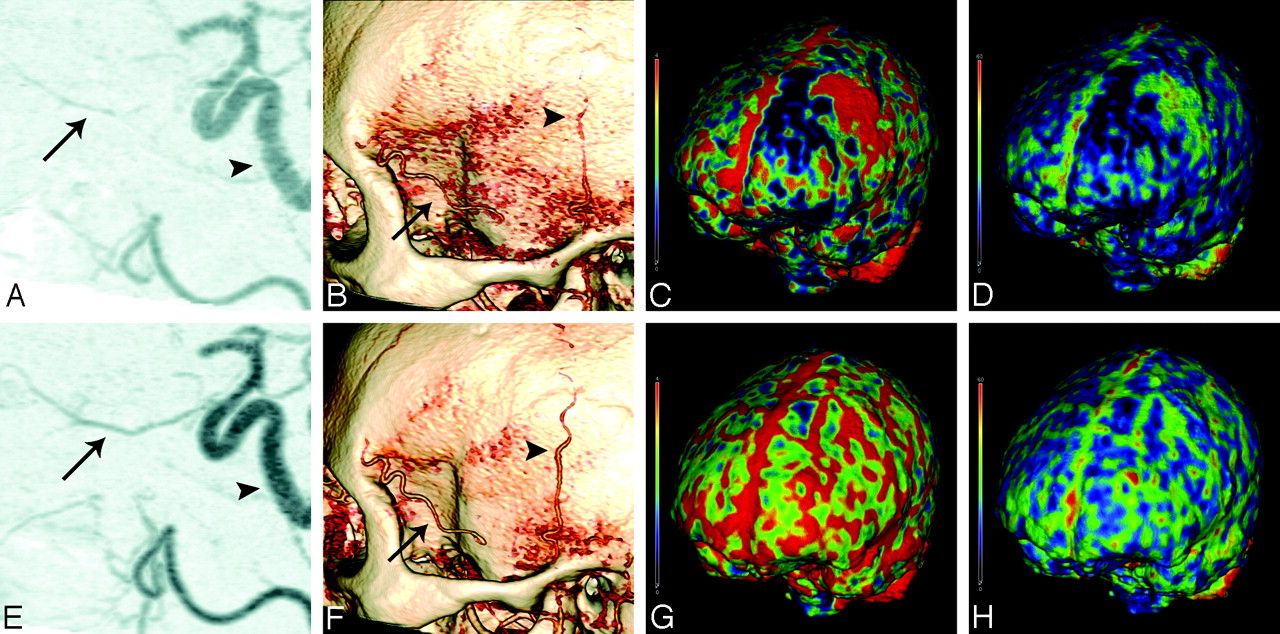
Three hundred twenty−detector row CT images obtained before (top row) and after (bottom row) corticosteroid therapy. A, CTA shows beading and stenosis of the precavernous, cavernous, and supraclinoid portions of the ICA (arrowhead). There is narrowing and irregularity of the ophthalmic artery (arrow), that is resolved after treatment as seen in E. B, 3D volume rendering shows narrowing and beading of parietal branch of the left STA (arrowhead) and irregularity of the remaining frontal branch (arrow), which are improved after therapy as seen in F. Note that the patient had a prior biopsy of the frontal branch. C and G, rCBV, and D and H, rCBF maps illustrate a region of decreased perfusion in the left frontal parasagittal region with adjacent hyperperfusion that returned to normal symmetric perfusion after therapy.
Discussion
The differential diagnosis of LVCV includes GCA, Takayasu arteritis, primary CNS angiitis, rheumatologic diseases, sarcoidosis, and numerous infections.5 The patient's age and sex were atypical for GCA; however, the diagnostic criteria for classification were met with new-onset headache, elevated ESR, and decreased pulsation of STA (sensitivity and specificity of 93.5% and 91.2%, respectively).6 The suspected diagnosis of GCA in this patient was strongly supported by the resolution of both symptoms and imaging findings following corticosteroid therapy.
The decision to reduce the dose of corticosteroids is a therapeutic challenge in GCA and is generally based on frequent assessment of clinical and laboratory findings, which are neither good indicators of acute-phase response nor sensitive predictors of disease flare.2 Application of PCT and CTA is a promising approach to follow-up treatment, facilitating corticosteroid tapering.2 Perfusion imaging has been advocated for the diagnosis of CNS vasculitis because it may detect regions of benign oligemia or reversible ischemia in the absence of a diffusion abnormality.7
The 320-detector row CT protocol provides CTA plus the following brain perfusion measurements: rCBV, rCBF, mean transit time (MTT), and time-to-peak (TTP). The advantage of the 16-cm craniocaudal coverage in comparison with 64-section imaging is that the later subvolume scanning focuses on the basal ganglia because ACA, MCA, and PCA territories are all represented on these sections.3,4 This can be especially limiting in vasculitis because important pathology such as regions of low CBV may not be associated with a specific vascular territory. In cases such as this one with regions of very low CBV, calculations of MTT and TTP (not shown) will be largely influenced by noise, and these maps, when obtained, should be used with caution.
The effective radiation dose (including noncontrast head CT, CTA, and PCT) was estimated by using an adaptation of the standard CT dose index methods used for conventional MDCT scanners.8 Each 80-kV 100-mA rotation delivers approximately 0.22 mSv, and the initial 300-mA dataset delivers 0.66 mSv. The total radiation for this protocol is approximately 4.6 mSv; this is on the lower end of the spectrum of previously reported doses for noncontrast head CT, CTA, and PCT.9 Dynamic volume CT in this patient demonstrated rapid high-quality imaging, including whole-brain perfusion, with relatively low radiation and iodinated contrast doses.
Large vessel vasculitis is a diagnostic challenge because of the complex and varied clinical presentations. Although conventional angiography clearly depicts vessel luminal changes, early vessel wall changes are not visualized. Moreover, this technique is invasive, with the risk of an ischemic complication.10 Duplex sonography may assist in the diagnosis of early vasculitis, providing information on vessel wall and blood flow; however, it is observer-dependent.10,11 PET is very sensitive in showing extracranial involvement of LVCV but provides no information regarding wall structure or luminal flow and has relatively low spatial resolution.10,11 Contrast-enhanced MR imaging can assess mural inflammation and vessel wall thickening and is used routinely.10,11 Comparison with MR imaging will be a critical step in the validation of 320-detector row brain CT. In addition to comparing imaging findings and longer term studies that include patient outcomes, factors such as radiation, ease of scanning, patient compliance and safety, radiation dose, and cost need to be considered.
To date, 320-detector row CT data have been reported for cardiac imaging,8,12 but brain perfusion studies are ongoing. CT can assess, to some degree, changes in the arterial wall thickness and enhancement, providing clinically useful tissue contrast between vascular and perivascular structures. CT has previously been shown to demonstrate vessel wall alterations in the setting of a normal vessel lumen in the diagnosis and follow-up of patients with early or advanced Takayasu arteritis.13
In conclusion, the combination of new 320-detector row CTA and PCT may evolve into a novel, noninvasive, fast, and relatively inexpensive method to diagnose early LVCV accurately. In this patient with clinically suspected LVCV, characteristic findings were very useful in evaluating disease severity and monitoring response to treatment.
References
- Received November 14, 2008.
- Accepted after revision January 5, 2009.
- American Society of Neuroradiology





{kind=link}
{kind=link}