
Abstract
BACKGROUND AND PURPOSE: Vascular endothelial growth factor is a well-known tumor-specific biomarker that mediates angiogenesis in glioblastoma via hypoxia-dependent mechanisms. Our aim was to investigate the correlation of clinical characteristics, radiologic features, and vascular endothelial growth factor expression with survival outcomes in patients with glioblastoma.
MATERIALS AND METHODS: Clinical and radiologic data of 185 patients with glioblastoma were retrospectively reviewed. Vascular endothelial growth factor expression was examined in all cases via immunohistochemical analysis. Univariate and multivariate analyses were performed to identify the prognostic factors of progression-free survival and overall survival.
RESULTS: Vascular endothelial growth factor expression levels were associated with the presence of ringlike tumor contrast enhancement. Age, preoperative Karnofsky Performance Scale score, gross total resection, and adjuvant therapy were identified as prognostic factors. Among patients undergoing gross total resection, high vascular endothelial growth factor expression was associated with longer progression-free survival (P = .011) and overall survival (P = .039). For tumors with high vascular endothelial growth factor expression, both the non-contrast-enhancing tumor component and peritumoral edema could stratify overall survival (P = .039 and .018, respectively), while only the presence of the non-contrast-enhancing tumor component predicted a longer progression-free survival (P = .024).
CONCLUSIONS: Vascular endothelial growth factor expression level was not an independent prognostic factor in glioblastoma. However, high vascular endothelial growth factor expression might predict longer survival in patients in whom gross total resection was achieved. Furthermore, peritumoral edema and the non-contrast-enhancing tumor component could stratify survival outcomes in patients with high vascular endothelial growth factor tumors.
ABBREVIATIONS:
- GTR
- gross total resection
- <GTR
- tumor residual
- HR
- hazard ratio
- KPS
- Karnofsky performance status scale
- nCET
- non-contrast-enhancing tumor component
- PFS
- progression-free survival
- OS
- overall survival
- VEGF
- vascular endothelial growth factor
Glioblastoma is a rapidly progressive and highly angiogenic tumor. The outcome of patients with glioblastoma is poor, owing to ineffective therapies. Even when surgical resection followed by adjuvant therapy is provided, the median progression-free survival (PFS) of these patients is only 6.9 months, and the median overall survival (OS) is 14.7 months.1 Clinical characteristics, including patient age, Karnofsky Performance Scale (KPS), and the extent of resection, have been investigated previously as prognostic factors for glioblastoma, while the prognostic role of radiologic features and potentially associated tumor-specific biomarkers remains unclear.
Vascular endothelial growth factor (VEGF) is a well-known tumor-specific biomarker that mediates angiogenesis in glioblastoma via hypoxia-dependent mechanisms, contributes to the generation of blood vessels with distinctive features, and promotes vascular permeability, resulting in the observation of the radiologic contrast enhancement in tumors, which should otherwise be prevented by an intact blood-brain barrier.2 The prognostic role of VEGF expression has been investigated in different types of malignancies, such as breast cancer,3 gastric track cancer,4⇓–6 and lung cancer.7,8 The levels of VEGF expression were found to be correlated with microvessel attenuation in human glioma.9 Moreover, the association of VEGF expression with survival outcome in patients with malignant tumor has been suggested.10,11 In a subsequent study, radiologic features (eg, edema) were introduced as a factor in the correlation between VEGF expression and prognostic outcome. This suggests that VEGF expression is predictive of survival in tumors with little or no edema.12
Further understanding of the role played by VEGF expression in predicting the survival of patients with glioblastoma is of clinical significance and is currently needed. Therefore, the present study aimed to identify the potential association of clinical and radiologic features and VEGF expression with survival outcome in patients with glioblastoma.
Materials and Methods
Patients
The medical records of 185 adult patients with glioblastoma who underwent surgical treatment at our institution between January 2007 and November 2008 were retrospectively reviewed. Inclusion criteria were as follows: 1) 18 years of age or older; 2) availability of presurgical MR imaging scans, including T1-weighted, T2-weighted, and postcontrast T1-weighted images; 3) pathologically confirmed glioblastoma; 4) no previous craniotomy or stereotactic biopsy; and 5) no previous diagnosis of any brain tumor. The histopathologic diagnosis of tumors was confirmed by 2 independent neuropathologists. This study was approved by our institutional review board, and written consent was obtained from all enrolled patients.
Treatment
In our study, “gross total resection” (GTR) was defined as no visible contrast-enhancing tumor on postoperative MR images obtained within 72 hours after surgery, according to an assessment comparing pre- and postoperative MR images.13 All cases in which GTR was not achieved were considered as having tumor residual (<GTR). Patients with severe edema who required corticosteroid treatment to alleviate intracranial hypertension were excluded to avoid a possible influence on radiologic evaluation results. The adjuvant treatment included radiation therapy or chemotherapy alone or concomitant temozolomide and fractionated radiation therapy followed by up to 6 cycles of adjuvant temozolomide.1
Image Acquisition
MR imaging was performed on a Trio 3T scanner (Siemens, Erlangen, Germany). It included axial T1-weighted (TR, 450 ms; TE, 15 ms; section thickness, 5 mm), T2-weighted fast spin-echo (TR, 6000 ms; TE, 140 ms; section thickness, 5 mm), and contrast-enhanced (gadopentetate dimeglumine, DTPA-Gd injection; Beilu Pharmaceutical Co., Beijing, China; 0.1 mmol/kg) axial T1-weighted images (TR, 450 ms; TE, 15 ms; section thickness, 5 mm). Postcontrast images were acquired immediately following injection of contrast agent. Postoperative MR images for determining the extent of resection were obtained within 72 hours after surgery.14
Identification of Imaging Features
Radiologic features of the tumor were assessed by 2 experienced neuroradiologists (Q. Chen and X. Chen, who have 14 and 12 years of experience, respectively, in brain disease diagnosis by using MR imaging) blinded to the patient clinical information. In cases in which imaging features identified by the 2 neuroradiologists were inconsistent, a third senior neuroradiologist (J.M., with 25 years of experience in brain disease diagnosis) examined the images for a final assessment. The patterns of tumor contrast enhancement were identified on the basis of the size and morphologic features of the largest enhanced area on contrast-enhanced MR images regardless of whether it was single- or multifocal and were categorized as ringlike or non-ringlike-enhanced patterns. Tumors displaying cystic necrosis with peripheral enhancement were defined by an enhanced ringlike pattern; tumors not displaying this pattern were classified as having non-ringlike-enhanced patterns. Limited (or no) edema (−) was defined as edema extending ≤1 cm from the margin of the tumor based on T2-weighted images; otherwise, edema was scored as moderate to severe (+).15 The non-contrast-enhancing tumor component (nCET) was defined as a region of hyperintensity on T2-weighted images (with corresponding hypointensity on contrast-enhanced T1-weighted images) that was associated with a mass effect and architectural distortion, including blurring of the gray-white interface (Fig 1).16

MR imaging features of patients with glioblastoma. The contrast-enhanced T1-weighted images showed ringlike contrast enhancement (A) and non-ringlike contrast enhancement (B). T2-weighted images show obvious peritumoral edema (+) (C) and little (or absent) peritumoral edema (−) (D). The non-contrast-enhancing tumor component refers to the tumor region of T2 hyperintensity (less than the intensity of CSF) (E) that was not enhanced on the contrast-enhanced T1-weighted image (white arrow) (F).
Immunohistochemistry
Immunohistochemical analysis of VEGF expression was performed for all patients. VEGF expression was scored by using 4-level grading criteria: (−) indicated <5% positive cells, (+) indicated mild expression with 6%–25% positive cells, (++) indicated moderate expression with 26%–50% positive cells, and (+++) indicated strong expression with >50% positive cells. Glioblastoma tumors were classified into 2 groups based on the level of VEGF expression as follows: low (−∼++) and high (+++) expression groups.
Statistical Analysis
The χ2 test was performed to detect the differences in clinical and radiologic features between patients with high and low VEGF expression. Consistency in the assessment of radiologic features by the 2 radiologists was evaluated by using the κ consistency test. Survival curves were generated by using the Kaplan-Meier method, and log-rank analysis was performed to compare PFS and OS. Significant prognostic factors (those with a P value < .05) identified by univariate analysis were entered into multivariate survival analysis by using the Cox proportional hazard ratio (HR) model.
Results
Patient Characteristics
A total of 185 patients with glioblastoma with post-T1 contrast enhancement were included in this study. Of these, tumors of 124 patients exhibited ringlike enhancement. Patient sex, preoperative KPS, enhancement pattern, and extent of resection were significantly different between the high and low VEGF expression groups (P < .001, χ2 test, On-line Table). On the basis of the postoperative contrast-enhanced T1-weighted images obtained <72 hours after the operation, 112 (60.5%, 112/185) had GTR, and 156 received adjuvant therapy following tumor resection. In addition, there was no significant difference in the expression of isocitrate dehydrogenase 1, O6-methylguanine DNA methyltransferase, and epidermal growth factor receptor between patients with high-versus-low VEGF expression.
Association of the Radiologic Features and Extent of Resection with VEGF Expression
All data regarding tumor volume and location are summarized in the On-line Table. The mean tumor volume of patients with high VEGF expression (+++) was significantly larger than that of patients with low VEGF expression (− ∼ ++) (P = .033). However, we observed no significant differences in the involvement of brain lobes between tumors with low and high VEGF expression.
The κ values for the consistency between the 2 evaluators for enhancement patterns, peritumoral edema, and nCET were 0.85 (P = .014), 0.81 (P = .008), and 0.76 (P = .021), respectively. Ringlike enhancement was more likely to be observed in glioblastomas with high VEGF expression than in those with low VEGF expression (75.6% versus 60.2%, P = .027, χ2 test).The prevalence of peritumoral edema and nCET in the low-versus-high VEGF expression groups was not significantly different (peritumoral edema: 66.0% versus 74.4%, P = .218; nCET: 35.0% versus 46.3%, P = .116; χ2 test). Moreover, GTR was significantly more likely to be achieved in glioblastomas with high VEGF expression than in those with low VEGF expression (72.0% versus 51.5%, P = .005).
Progression-Free Survival
Tumor recurrences were identified by MR images in 143 (77.3%) patients during the follow-up period. The median follow-up period for PFS analysis was 9.8 months (range, 1.0–53.1 months), and the median PFS was 7.6 months (range, 2.1–32.6 months). Univariate analysis revealed that age (P = .018), preoperative KPS (P = .015), extent of resection (P = .013), and adjuvant therapy (P = .021) were valuable prognostic factors for PFS (Table 1). These 4 factors remained significant in the multivariate Cox proportional hazards analysis. Age at diagnosis of 50 years or older (P = .032, HR = 1.642) and preoperative KPS of <80 (P = .024, HR = 2.215) were associated with shorter PFS, whereas GTR (P = .022, HR = 1.849) and adjuvant therapy (P = .038, HR = 0.652) indicated longer PFS (Table 2).
Univariate analysis of survival outcomes for patients with glioblastoma
Multivariate analysis of survival outcomes
Overall Survival
At the time of analysis, 23 patients with available follow-up data were alive. The median follow-up period for OS analysis was 13.8 months (range, 2.0–86.8 months), and the median OS was 15.1 months (range, 3.8–67.6 months). Univariate analysis identified age (P = .029), preoperative KPS (P = .038), extent of resection (P = .022), and adjuvant therapy (P = .032) as prognostic factors of OS (Table 1). In the multivariate Cox proportional hazards analysis, age at diagnosis of 50 years or older (P = .043, HR = 1.348) and preoperative KPS of <80 (P = .028, HR = 1.782) were identified as poor prognostic factors for OS, whereas GTR (P = .031, HR = 1.615) indicated longer OS. However, adjuvant therapy failed to show a predictive value for survival outcomes (Table 2).
Prognostic Value of VEGF Expression Levels in Patients with GTR
To examine the prognostic value of VEGF expression when the extent of resection was taken into account, we classified patients into 4 groups according to their VEGF expression levels and the extent of resection as follows: GTR and high VEGF expression, <GTR and high VEGF expression, GTR and low VEGF expression, and <GTR and low VEGF expression. Survival outcomes were compared among these groups by using the log-rank test. We found that patients with glioblastoma with high VEGF expression and GTR had significantly longer survival than others (P = .011 for PFS and P = .039 for OS) (Fig 2). However, there was no significant difference in survival outcomes among the other 3 groups.

Survival outcomes of patients with glioblastoma. Kaplan-Meier survival curves of patients classified by the extent of resection and vascular endothelial growth factor expression are shown. Patients who had high tumor VEGF expression (+++) and achieved gross total resection had significantly longer progression-free survival and overall survival than those with low tumor VEGF expression and residual tumor after surgery (P = .011 and .039, respectively).
Prognostic Value of Peritumoral Edema in Patients Stratified by VEGF Expression Levels
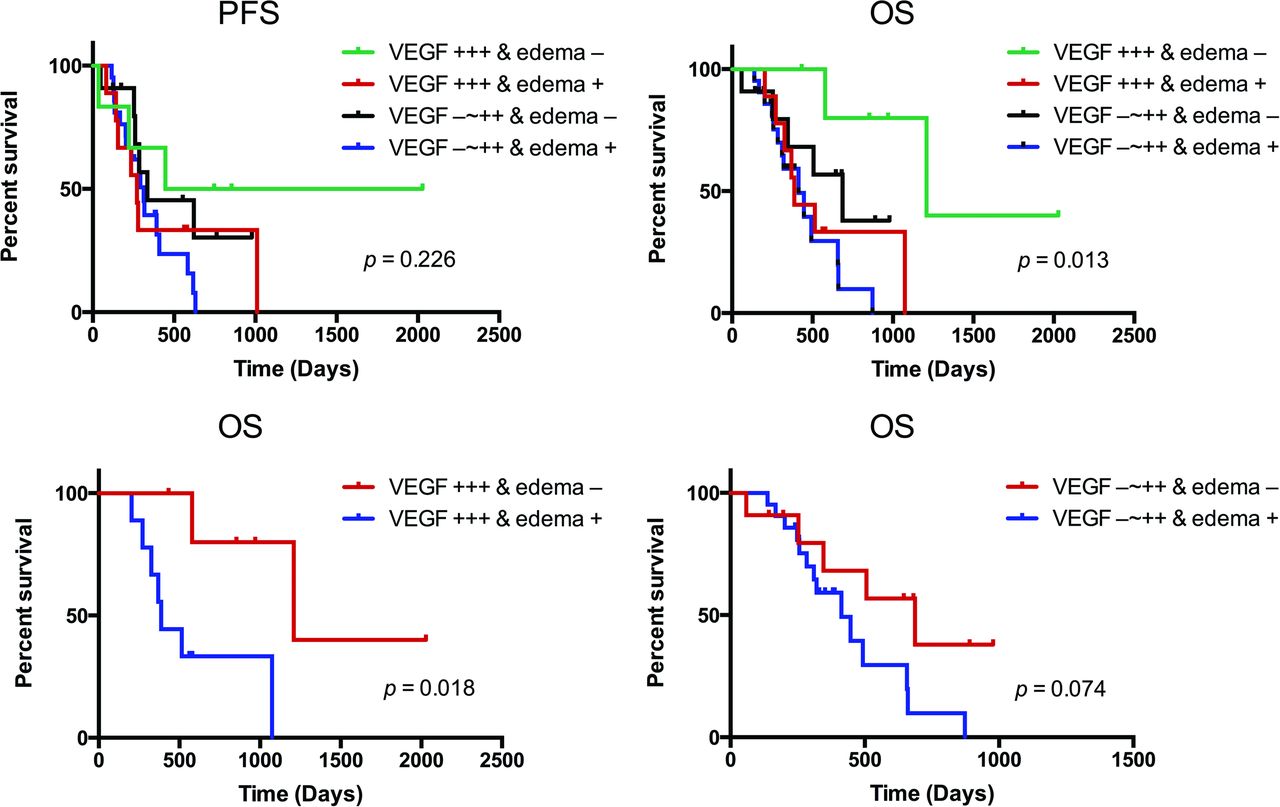
The potential interactive and synergistic roles of peritumoral edema and VEGF expression in predicting the survival of patients with glioblastoma were also investigated. Patients were subdivided into 4 groups according to the presence of peritumoral edema and VEGF expression levels. Survival outcomes were compared among these groups by using the log-rank test. For OS, tumors with VEGF expression (+++) and peritumoral edema (−) indicated a longer survival compared with the other 3 groups (P = .013, log-rank). Specifically, peritumoral edema could stratify OS for tumors with high VEGF expression (P = .018, log-rank), but not for those with low VEGF expression (P = .074, log-rank). For PFS, however, there was no significant difference among the 4 groups (P = .226, log-rank), and peritumoral edema could not stratify survival for different VEGF expression levels (Fig 3).

Kaplan-Meier plots of patients with glioblastoma showing the association between the progression-free survival and overall survival according to combined vascular endothelial growth factor expression levels and peritumoral edema. Tumors with high VEGF expression (+++) and without peritumoral edema correlated with better OS (P = .013, log-rank), but not PFS (P = .226, log-rank). Furthermore, peritumoral edema could stratify the OS for tumors with high VEGF expression (P = .018, log-rank), but not those with low VEGF expression (P = .074, log-rank).
Prognostic Value of the Non-Contrast-Enhancing Tumor Component in Patients Stratified by VEGF Expression Levels
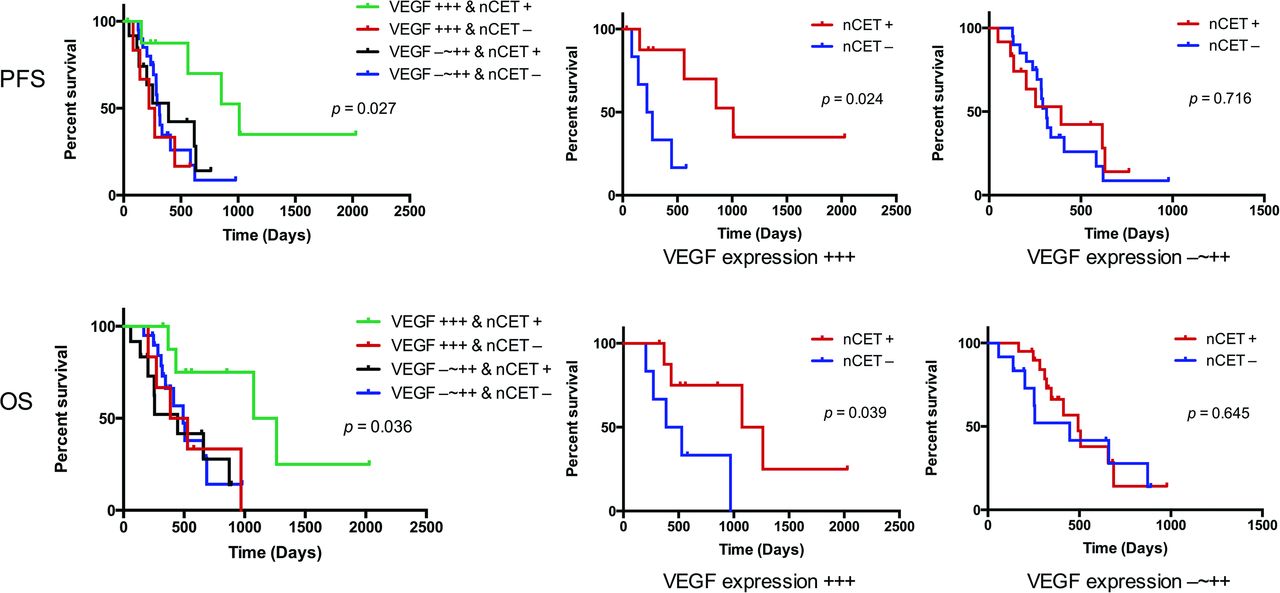
Kaplan-Meier curves according to the presence of nCET and VEGF expression levels showed that patients with high VEGF expression and nCET had a better survival (P = .027 for PFS and P = .036 for OS, log-rank). In the high VEGF expression group specifically, the presence of nCET predicted longer PFS (P = .024, log-rank) and OS (P = .039, log-rank). However, the prognostic value of nCET for PFS and OS was not observed in patients with low VEGF expression (P = .716 for PFS and P = .645 for OS, log-rank) (Fig 4).
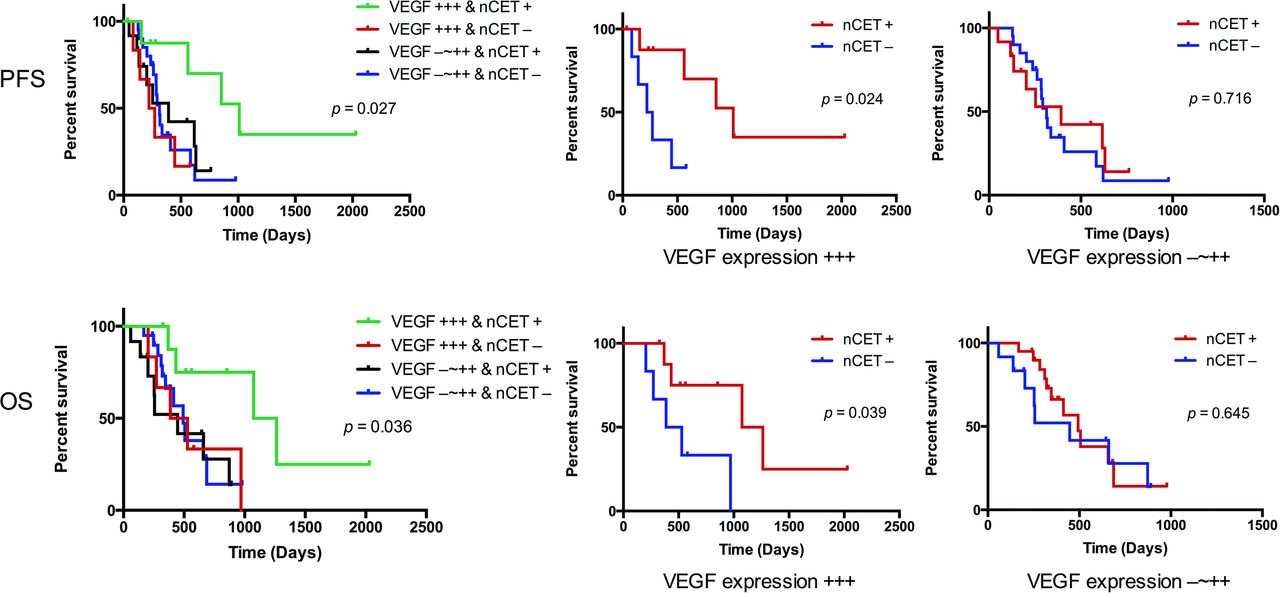
Kaplan-Meier survival curves show the progression-free survival and overall survival of patients with glioblastoma tumors with different vascular endothelial growth factor expression levels and non-contrast-enhancing tumor components. Tumors with high VEGF expression and the presence of nCET predict better survival (PFS, P = .027; OS, P = .036, log-rank). Moreover, nCET enables stratification of the PFS and OS of patients with high VEGF expression (PFS, P = .024; OS, P = .039, log-rank), but not of patients with low VEGF expression (PFS, P = .716; OS, P = .645, log-rank).
Discussion
In this study, we combined clinical, radiologic, and genetic characteristics in an investigation of prognostic factors for glioblastoma in a large cohort of patients. We found that peritumoral edema and nCET were of predictive value for survival in patients with a high expression level of VEGF. Notably, VEGF expression was a prognostic factor for patients achieving GTR, but not for those who did not.
Tumor-specific molecular markers have long been studied for their potential prognostic role in cancers. VEGF expression has been described as a valuable indicator of tumor recurrence in many types of malignancy.17 It was found that high expression levels of VEGF correlated with poor prognosis, while anti-VEGF therapy was shown to suppress tumor development and improve prognosis in glioblastoma.18,19 Glioblastoma is thought to exhibit abnormally high levels of VEGF.20,21 In this study, we found that VEGF expression alone was not a prognostic factor for patients with glioblastoma. However, VEGF might interact with other potential factors to determine survival outcomes.
VEGF regulates pathologic angiogenesis, resulting in the formation of new blood vessels to facilitate tumor growth.22 A previous study suggested that rapid tumor cell proliferation leads to oxygen shortage and necrosis in the center of a tumor, which is prone to present as a ringlike pattern of contrast enhancement. Consistent with these findings, we also observed that glioblastomas with high VEGF expression were more likely to present with a ringlike enhancement pattern than those with low VEGF expression. In addition, tumors with ringlike enhancement often exhibit a relatively clear radiologic border on postcontrast T1-weighted images and thus might more easily be localized during an operation for total resection. This might explain why GTR was more likely achieved in glioblastomas with high VEGF expression than in those with low VEGF expression.
Furthermore, we evaluated the interactive effects between the extent of resection and VEGF expression in predicting survival of patients with glioblastoma. Our results suggested that the prognostic value of VEGF expression was only valuable in patients who achieved GTR, thus implying a codependent effect of the 2 factors in predicting survival. Because lesions with high VEGF expression are prone to necrosis and, accordingly, exhibit ringlike enhancement patterns, tumors with ringlike enhancement patterns have relatively distinguishable margins that may facilitate resection. It was also reported that patients with cystic glioblastoma with thin-wall ringlike enhancement might also benefit from GTR,23 suggesting that cystic tumors might be circumscribed lesions with a distinct pattern of invasiveness or limited infiltration of the surrounding neutrophils. Therefore, patients with glioblastoma with high VEGF expression (+++) were more likely to benefit from GTR in terms of prolonging survival. Nevertheless, the inherent reason that VEGF expression might play a predictive role in the survival of patients with glioblastoma with GTR but not in those without GTR remains to be further investigated.
VEGF is known to be a potent permeability factor that causes edema,24,25 and the inhibition of VEGF reduces edema and tumor burden in patients with glioblastoma.26,27 It has been shown that VEGF expression is predictive of longer survival in cases of tumors with little or no edema, but not in those with extensive edema, indicating that edema could be the regulated by both VEGF-dependent and VEGF-independent pathways.12 Most interesting, the current study demonstrated that peritumoral edema could stratify the survival of patients with high VEGF expression (+++), but not of those with low VEGF expression (− ∼ ++). Although VEGF expression was correlated with edema and could promote peritumoral edema development, some tumors with high VEGF expression might not develop significant peritumoral edema.12 In addition, VEGF and neuronal pentraxin-2 may affect MR imaging features of edema and enhancement, suggesting that edema development might not be directly regulated by VEGF.28 For tumors with high VEGF expression (+++), the survival difference between patients with and without peritumoral edema might be partly attributed to the underlying mechanism of tumorigenesis, in which the angiogenic effect of VEGF may act differently in a manner that remains to be determined. Furthermore, as mentioned above, tumors with high VEGF expression are prone to necrosis and, accordingly, exhibit ringlike enhancement patterns, which may present relatively distinguishable margins and facilitate better resection. In tumors with no peritumoral edema, GTR would suggest less residual tumor cells and would thus predict longer PFS.
Previous studies have demonstrated that nCET is a valuable prognostic indicator in patients with glioblastoma; this finding was regarded as novel.16 In the current study, we showed that nCET was a prognostic factor for tumors with high VEGF expression (+++), but not for those with low (−∼++) VEGF expression. In general, hypoxia induces the increased expression of VEGF and leads to tumor necrosis, suggesting a rapid growth and more aggressive behavior.12 However, it was found that the nCET regions might lack necrosis and likely correspond to tumor areas with a lower pathologic grade and less aggressive behavior. A previous study showed that nCET was a valuable prognostic indicator.16 Although nCET did not show a prognostic value in the current study, it was more likely to be present in glioblastomas with high VEGF expression. Thus, we speculate that nCET and VEGF might play synergistic roles in affecting survival outcomes. In addition, the prognostic value of nCETs might be partly owing to their association with oligodendroglioma components. Genetic analysis may provide additional clues to explain why the prognostic value of nCET depends on VEGF expression levels.
The current study has some limitations. First, we retrospectively enrolled patients from a single institution. Second, the combined prognostic role of VEGF expression and clinical and radiologic features requires further confirmation by a prospective multicenter investigation. Finally, due to the relatively suboptimal timing of the postoperative scans, the potential presence of granulation tissue may confound MR imaging results. Future studies should also focus on the association between clinical and radiologic characteristics and the survival of patients with tumors exhibiting other molecular markers.
Conclusions
In summary, we showed that VEGF expression was a valuable prognostic factor in patients who achieved GTR, whereas peritumoral edema and nCET could stratify survival outcomes for tumors with high VEGF expression. Thus, our findings suggest synergistic roles for tumor-specific biomarkers, surgical resection, and preoperative MR imaging features in predicting survival outcomes.
Acknowledgments
We thank Drs Q. Chen and X. Chen for their efforts in tumor imaging evaluation.
Footnotes
Kai Wang and Yinyan Wang contributed equally to this study.
Disclosures: Tao Jiang—RELATED: Grant: This work was supported by the National Basic Research Program of China (No.2011CB707804 and No. 2015CB755500).* Jianping Dai—RELATED: Grant: This work was supported by the National Natural Science Foundation of China (No. 81271541).* *Money paid to the institution.
This work was supported by the National High Technology Research and Development Program (No.2011CB707804 and No. 2015CB755500) and the National Natural Science Foundation of China (No. 81271541).
The authors declare that they have no conflict of interest.
Indicates open access to non-subscribers at www.ajnr.org
REFERENCES
- Received May 30, 2015.
- Accepted after revision August 19, 2015.
- © 2016 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.