
We read with special interest the case report1 of a 50-year-old immunocompetent patient with neurosyphilis mimicking herpes encephalitis. The patient presented with a clinical syndrome of encephalitis and bilateral mesiotemporal hyperintensity on T2WI and FLAIR images. It is known that neurosyphilis can present with a variety of CNS manifestations, sometimes mimicking other diseases and making the differential diagnosis difficult. We present an additional case of a syphilitic gumma with CNS involvement, with MR imaging findings resembling a brain stem glioma.
A 26-year-old man presented with a 4-month history of fever, weight loss, dizziness, diarrhea, tremors, and paresthesia. Clinical examination revealed disorientation, pyramidal and extrapyramidal symptoms, and multiple cutaneous nonpruriginous cicatricial lesions affecting the chest and inferior limbs, suggestive of syphilitic roseola. A rapid human immunodeficiency virus test was positive, with a CD4+ lymphocyte count of 254 cells/mm3 and a viral load of 26,217 copies/mm3 (log 4.419). The syphilis serology was strongly positive for nontreponemal specific antibodies with a Venereal Disease Research Laboratory titer of 1:16. CSF examination revealed aseptic meningitis with lymphocytic pleocytosis, elevated protein, and normal glucose levels.
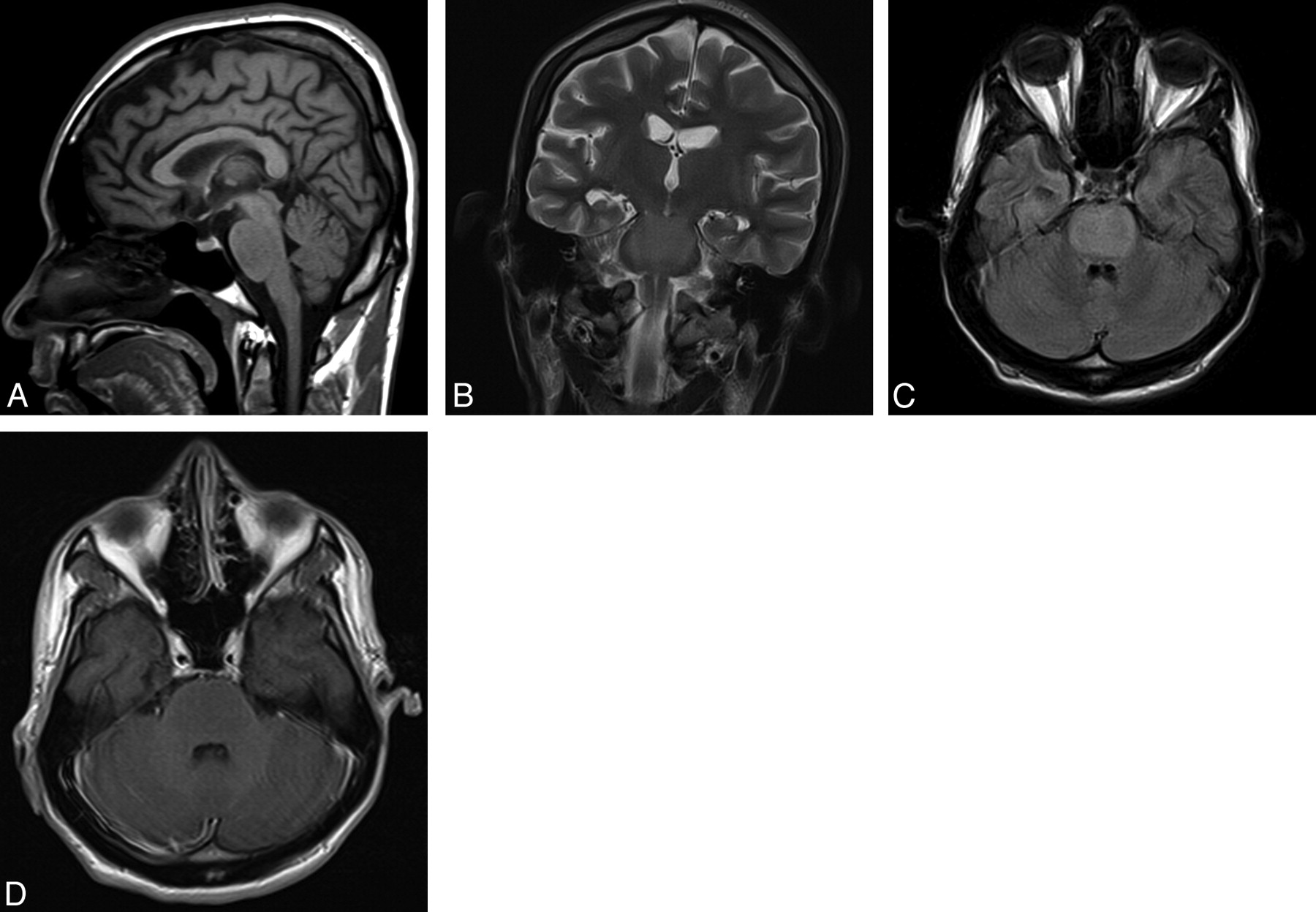
Brain MR imaging revealed a pontine lesion isointense to gray matter on T1WI sequences and hyperintense on T2WI and FLAIR sequences, without contrast enhancement, occupying almost the entire pons (Fig 1). The advanced MR imaging techniques showed no restricted diffusion, low relative CBV, and mild increase in the choline/N-acetylaspartate ratio. Although the diagnostic hypothesis of diffuse pontine glioma was considered, on the basis of the clinical data, the possibility of an infectious/inflammatory disease was also mentioned. The patient was treated with high-dose intravenous crystalline penicillin (24 × 106 units/day) for 14 days and showed significant clinical improvement. The findings of the follow-up brain MR imaging, 1 week after the end of the treatment, were completely normal and the patient was discharged for outpatient follow-up.

MR imaging revealed a pontine lesion occupying almost the entire pons, isointense to gray matter on sagittal T1WI (A), hyperintense on coronal T2WI (B) and axial FLAIR (C), without contrast enhancement on axial T1WI post-gadolinium (D).
To the best of our knowledge, there is only 1 previous report describing a syphilitic cerebral gumma manifesting as a brain stem mass.2 It is known that the diagnosis of syphilis infection is a challenge because most patients are asymptomatic and MR imaging findings can be normal or nonspecific. However, during the acquired immune deficiency syndrome era, there has been a dramatic rise in the number of cases of syphilis and a corresponding increase in the incidence of neurosyphilis.3 Thus, before starting therapy, it is necessary to make a precise differential diagnosis and include cerebral gumma in the differential of mass lesions in immunocompetent or immunocompromised patients. Early diagnosis of neurosyphilis and appropriate antibiotic treatment result in notable clinical improvement and can assist in avoiding unnecessary brain biopsy, surgery, or radiation therapy.
- © 2012 by American Journal of Neuroradiology





{kind=link}