
Abstract
BACKGROUND AND PURPOSE: Acute SAH is reportedly associated with rebleeding from aneurysms, and recent advances in imaging technology allow us to visualize active bleeding in SAH cases. This study aimed to retrospectively investigate the incidence and characteristics of active bleeding in patients with spontaneous SAH by using multiphase dynamic-enhanced CT.
MATERIALS AND METHODS: We retrospectively surveyed a series of patients with SAH who underwent CTP with 18-phase dynamic enhancement and confirmed the presence of extravasated contrast medium in the source image. We compared clinical features between 2 groups of patients with and without extravasation.
RESULTS: Active bleeding was observed with increasing enhancement in 25.5% (13/51) of patients. All patients with extravasation were in Claassen grade 3 or 4 and WFNS grades 3, 4, or 5. The other group without extravasation included patients in all grades. A significant difference was observed in Claassen grade, WFNS grade, and increase of hematomas in follow-up CT (P < .05, for each) between the 2 groups. All CTP results of patients with extravasation were obtained within 2 hours of the onset of symptoms of SAH (P < .05). There was no significant difference in mortality at 14 days between the 2 groups (P = .128).
CONCLUSIONS: A high incidence of active bleeding (25.5%) was detected by multiphase dynamic-enhanced CT in patients with acute SAH. These results indicate that an awareness of active bleeding in patients with SAH has the potential to affect the treatment strategy.
ABBREVIATIONS:
- ACA
- anterior cerebral artery
- BA
- basilar artery
- ICH
- intracerebral hemorrhage
- VA
- vertebral artery
- WFNS
- World Federation of Neurosurgical Societies
Bleeding from SAH is reportedly arrested immediately by increasing intracranial pressure.1 Active bleeding with ICH expansion has been evaluated by CT,2 and a few cases have been reported in which active bleeding from an aneurysm was observed on CT.3,4 Recent developments in imaging techniques have enabled us to obtain more information about the hemodynamics of cerebral vascular diseases, and active bleeding from aneurysms in patients with SAH has been demonstrated by time-resolved multiphase dynamic-enhanced CT.5 CTP analysis has been used to assess perfusion disturbances caused by increasing intracranial pressure, and these time-resolved image data from multidetector row CT can be used to observe active bleeding from aneurysms in patients with spontaneous SAH.
We retrospectively investigated the incidence of active bleeding in patients with SAH and correlated these findings with clinical characteristics. This is the first investigation, to our knowledge, of the incidence of active bleeding from aneurysms in patients with acute spontaneous SAH.
Materials and Methods
Patients and Ethics
We retrospectively reviewed all patients with acute cerebral stroke who underwent a brain CTP scan on admission to our hospital between July 2009 and March 2011 and identified 55 consecutive patients with spontaneous SAH. We excluded patients with no obvious hemorrhage on plain head CT, patients with ICH and not SAH, patients with traumatic SAH, and patients in whom CTP was not performed because of an unstable condition or renal deficiency. We recorded the age, sex, aneurysm location, clinical WFNS grade,6 Claassen grade for the amount of SAH,7 time elapsed from the onset of symptoms until examination, surgical management, increase in the amount of hematoma on follow-up plain CT scans, and mortality within 14 days from onset or admission. Our institutional ethics committee exempted this retrospective study from documented patient consent because patient identifiers were removed, and the study was conducted in accordance with the Declaration of Helsinki.
CT Procedures
Our routine protocol for acute SAH includes a plain head CT, a CTP scan to evaluate perfusion disturbance caused by increased intracranial pressure, and helical CTA to confirm the location of the aneurysm. We used a 64-row detector CT scanner (LightSpeed VCT XT; GE Healthcare, Milwaukee, Wisconsin) and the toggling-table CT technique to extend scan coverage to 80 mm in the z-axis for a perfusion scan with scanning parameters of 80 kVp, 180 mA, and 0.4 s/rotation. We intravenously administered 40 mL of iodine contrast medium (iopamidol, 370 mg iodine/mL) followed by a 20-mL saline push. Five seconds after injection, we performed 18 intermittent axial scans at 2.8-second intervals in each table position. The order of the procedures was plain CT, helical CTA, and CTP during the early period (from July 2009 to December 2009) and plain CT, CTP, and helical CTA during the later period (from January 2010 to March 2011). This protocol change was made to improve the reliability of the CTP data.
Image Processing
We reconstructed 18-phase CTP source images for perfusion analysis with a 5-mm thickness, 512 × 512 matrix, and a 25-cm FOV for 16 sequential locations, thus obtaining 288 images for each patient. To improve image noise and to reduce radiation exposure during the multiphase CTP scan, we used an adapted statistical iterative reconstruction algorithm (ASiR; GE Healthcare) that exclusively filtered back-projection reconstruction for perfusion source images. This process allowed us to achieve a low-volume CT dose index of 85 mGy, which is comparable with that required for plain head CT (55–95 mGy, depending on the patient), and a total dose-length product of 680 mGy cm, which is smaller than that used for plain head CT in our institution. Although time-resolving 4D CT volume data with a section thickness of 0.625 mm were reproduced from dynamic CTP scan data from multidetector row CT equipment, we did not always use these data in the present study because the number of source images reached 2304, which is cumbersome for analysis.
Image Interpretation
One radiologist (K.S.) and 1 neurosurgeon (N.T.) evaluated plain CT images to investigate hematomas by using the Claassen classification.7 They evaluated CTP source images to find extravasation by using a PACS system to display movie-like images of each section. When examining the CTP time-resolved sequential source images, we identified the presence of contrast extravasation with an increasing spindle-shaped or twisted ribbonlike enhancement or nebulous enhancement in the subarachnoid space as active bleeding. We used a 4D CT volume-rendered image or a multiplanar reconstructed image, if required, to confirm the existence of extravasation. However, the final judgment of extravasation was made by using an operator-independent 5-mm-thickness source image for perfusion analysis. We used neither perfusion variables nor a color map because the roles of these indices in CTP were not the focus of this study. We also reviewed helical CTA images to locate aneurysms and/or the origin of bleeding and follow-up plain CT scans to evaluate changes in hematomas.
Statistical Analysis
JMP8 (SAS Institute, Cary, North Carolina) was used for statistical analyses. Patients whose ruptured lesion was not within the scanning range of the perfusion scan were excluded from statistical analysis because the existence of active bleeding could not be confirmed in these patients. The patients were divided into 2 groups, with and without extravasation. The Pearson χ2 test was used for aneurysm location to evaluate correlation to the existence of extravasation between the groups; the Wilcoxon rank sum test, for age; and the Fisher exact test, for other factors.
Results
We identified 55 consecutive patients with acute SAH who met our inclusion criteria. Of these, 4 were excluded from statistical analysis because they had a ruptured aneurysm in the vertebral artery that was outside of the CTP scanning range. The results are summarized in the Table. Ultimately, 19 male and 32 female patients were reviewed.
Characteristics of patients with and without active bleeding
Extravasation of contrast medium on multiphase CTP scan source images was observed in 13 patients (25.5%). Active bleeding was more common in MCA and VA/BA aneurysms than in those involving the ICA and ACA territories. All patients with active bleeding had Claassen grades 3 and 4, and WFNS grades 3, 4, and 5. Among 39 patients whose time of onset of symptoms could be identified, all 11 with bleeding but only 15 of the 28 without bleeding underwent CTP scanning within 2 hours of the onset (P = .007). The incidence of active bleeding in the patients scanned within 2 hours of the onset was 42.3% (11/26).
Seven patients with active and 25 without active bleeding underwent surgical repair of the aneurysm. Among 7 patients with active bleeding who underwent surgical clipping or coil embolization, 3 had premature ruptures during the procedures. Increased amounts of hemorrhage on follow-up CT were observed in 7 patients with active bleeding and 5 without active bleeding (P = .002). Patient mortality in the first 14 days after the onset was 45.5% (23/51), with no significant difference in mortality between the 2 patient groups (P = .207).
Four representative cases are shown in the figures. Figure 1 demonstrates a case of severe SAH with active bleeding from a dissected vertebral artery. Figure 2 shows nebulous enhancement, which may be 1 of the characteristic findings of active bleeding in patients with SAH. Enhancement near the aneurysm is similar to the spot sign of intracerebral hemorrhage (Fig 3). String-shaped extravasation is seen in Fig 4.

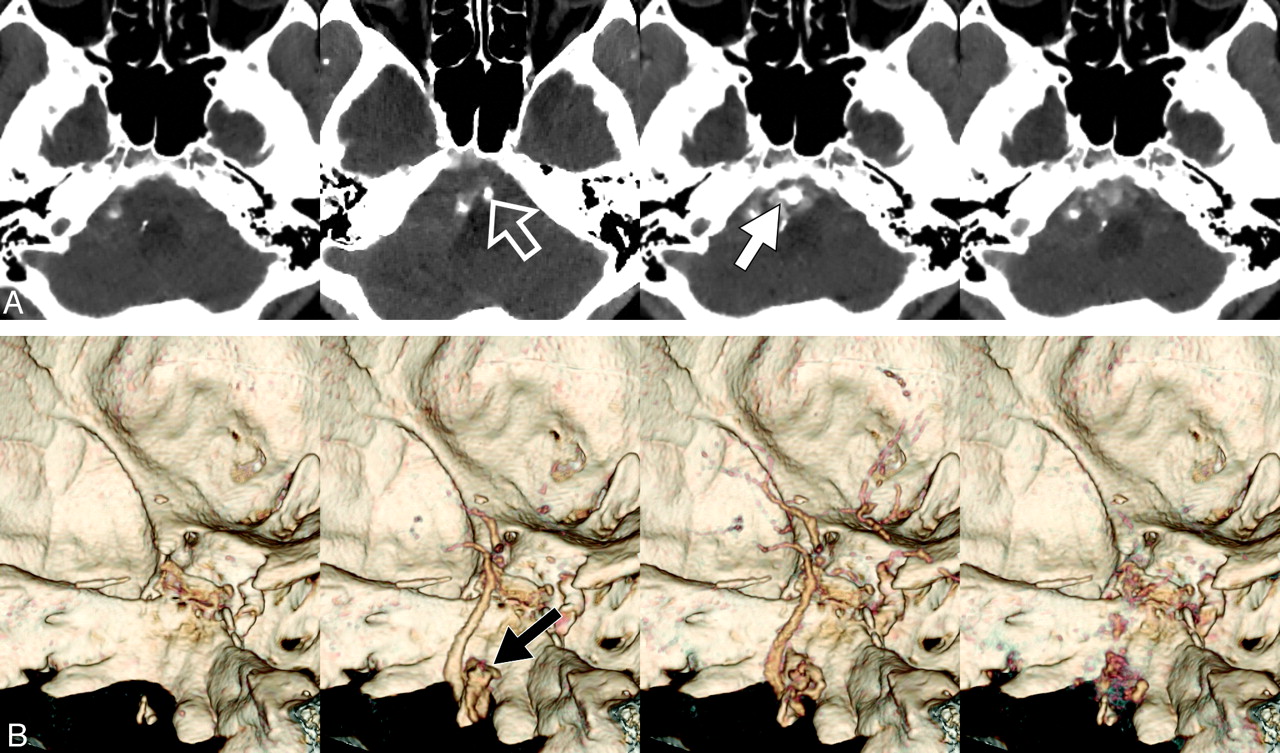
A 64-year-old man with Claassen grade 3 and WFNS grade 5. Extravasation from the right VA was observed on a multiphase enhanced source image. We selected 4 typical phases obtained at 5, 30.2, 38.6, and 52.6 seconds from among 18-phase scans taken at 2.8-second intervals on multiphase dynamic-enhanced CT. A portion of the right VA near the union was enhanced during the early phase (A, blank arrow), and lobulated extravasation was depicted as an irregularly shaped enhancement (A, white arrow). The premedullary cistern was enhanced in the late phase. Extravasation was well depicted as a wedge-shaped enhancement extending into the subarachnoid space on an additional 4D CT image (B, dark arrow). VA dissection with active bleeding was diagnosed.
Discussion
Bleeding from an aneurysm, often described as spontaneous bleeding with subsequent rebleeding, is typically observed on intra-arterial angiography8,9 in patients with marked changes in vital and neurologic signs. Rebleeding from an aneurysm is a prognostic factor.10 Nornes1 hypothesized that increasing intracranial pressure prevents continuous bleeding in patients with SAH. They described bleeding that intracranial pressure is increased by rebleeding to reach the level of systolic blood pressure immediately and then arrest bleeding. However, surprisingly, we found the incidence of active bleeding in patients scanned within 2 hours from onset of symptoms to be 42.3% (11/26). This result may reflect the inclusion of patients with continuous bleeding, as seen with other systematic injuries. The subarachnoid space is very large, and local intracranial pressure may not increase rapidly enough to arrest bleeding. Active bleeding was not seen beyond 2 hours after the onset of symptoms, indicating that most SAH stops within 2 hours. Ohkuma et al11 reported a high incidence of rebleeding during ambulance transfer or at the referring hospital before admission to their hospital. Some of their patients might have had active continuous bleeding.
The incidence of active bleeding in our study was higher than expected, and our findings may thus alter future treatment strategies. Although most active bleeding stops within 2 hours of onset, these patients may be at elevated risk of rerupture or premature rupture during surgery. Among 7 patients with active bleeding who underwent surgical clipping or coil embolization, 3 had premature rupture during the procedure. Early surgical intervention is reportedly a risk factor for rebleeding,12,13 though some authors have advocated early endovascular treatment.14⇓–16 Because ventricular drainage is often adopted for patients with severe symptoms before treatment of an aneurysm,17 rebleeding may be easily induced in patients with active bleeding. Nevertheless, given that 42.3% of our patients with SAH showed active bleeding within 2 hours of onset of symptoms, particularly those with high-grade severe SAH, it might be advisable to wait at least a few hours after the onset of symptoms for invasive examinations, treatments, and even transfer to a stroke center.
The spot sign of acute ICH is an indicator of hematoma expansion,18,19 but active bleeding signs in SAH are slightly different on dynamic-enhanced images. Our current observations suggest nebulous enhancement to be a characteristic finding of active bleeding in patients with SAH (Fig 2). This finding is attributable to the large area of the subarachnoid space, particularly when coagulated hematoma does not exist around the aneurysm.20 Thus, even slight enhancement in the subarachnoid space can be observed more easily on a thick-slab maximum-intensity-projection image than on a volume-rendered image (Fig 3), because volume-rendering is an operator-dependent technique. Although string-shaped extravasation in SAH often mimics vascular structures,20⇓⇓–23 multiphase CT imaging is superior to routine CTA, differentiating between extravasation and vascular structures, including aneurysms, because extravasated contrast medium is not washed out in the delayed phase (Fig 4).
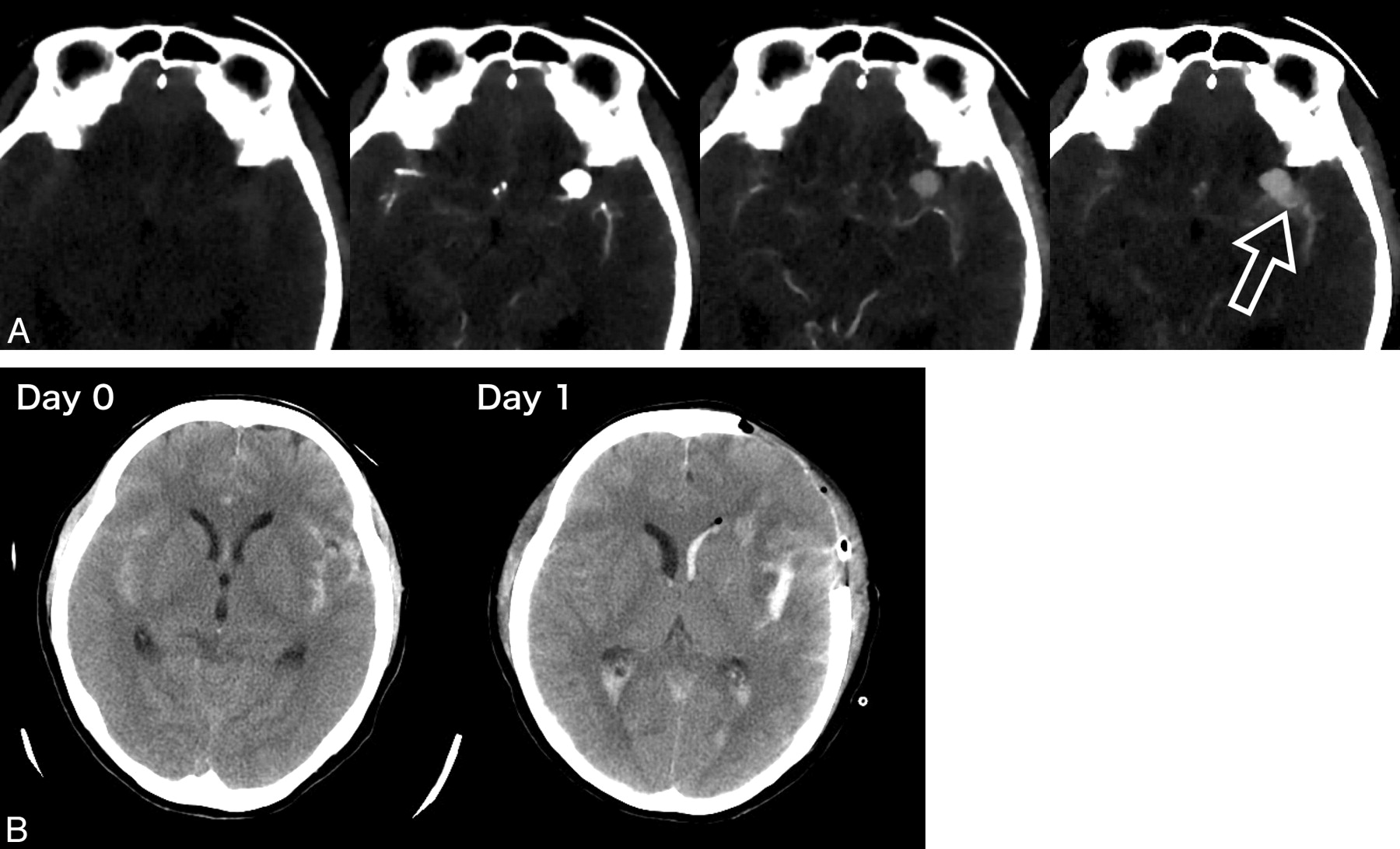
A 56-year-old woman with Claassen grade 3 and WFNS grade 4. There was a large aneurysm in the MCA. We selected scans obtained at 5, 24.6, 33, and 52.6 seconds, and this case showed typical findings of nebulous enhancement around an aneurysm that was associated with extravasation (A, blank arrow). Hematomas larger than those seen on plain CT were observed during the surgical clipping procedure, and premature rupture occurred intraoperatively. A follow-up plain CT obtained the following day showed increased hematoma (B).
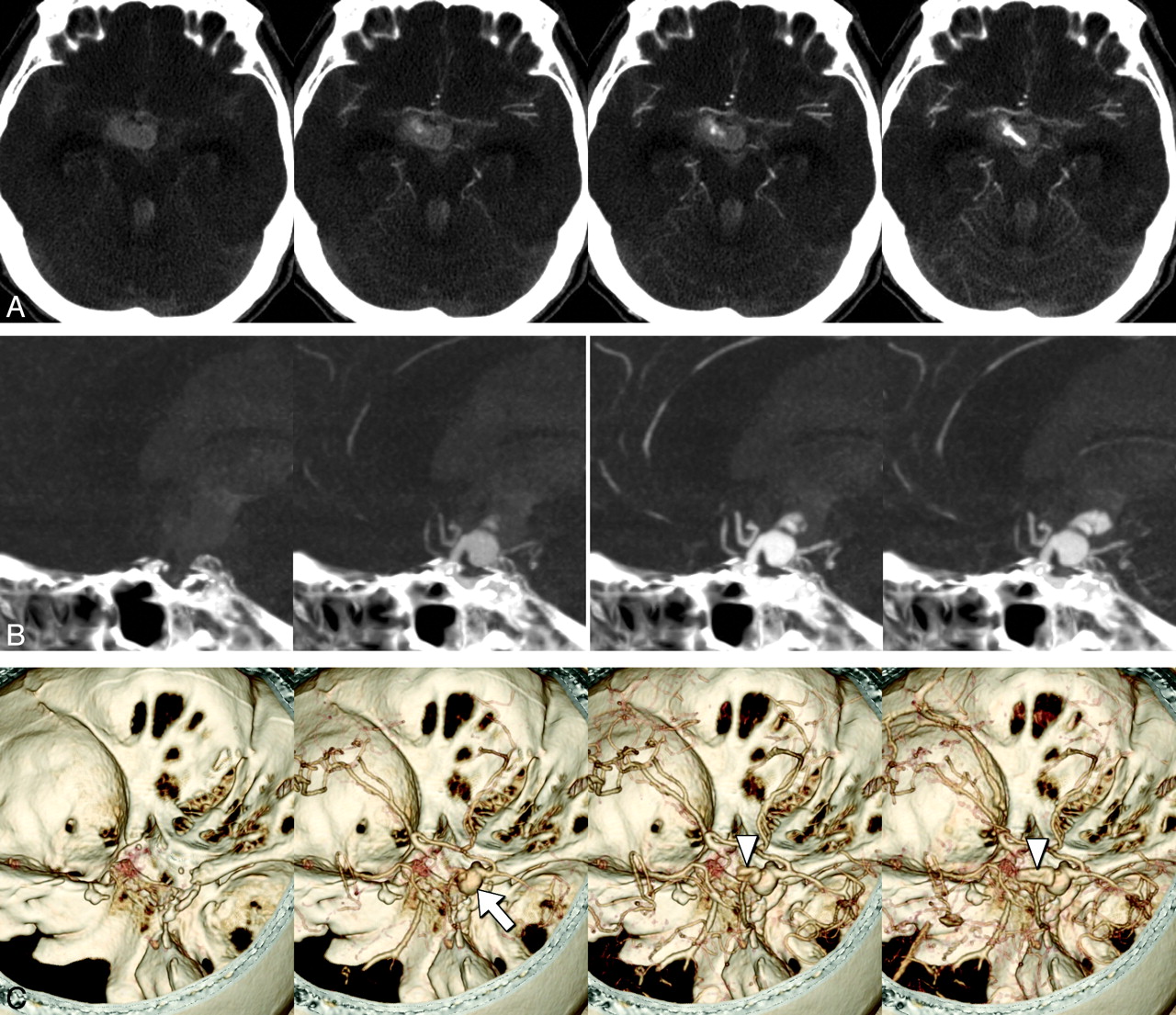
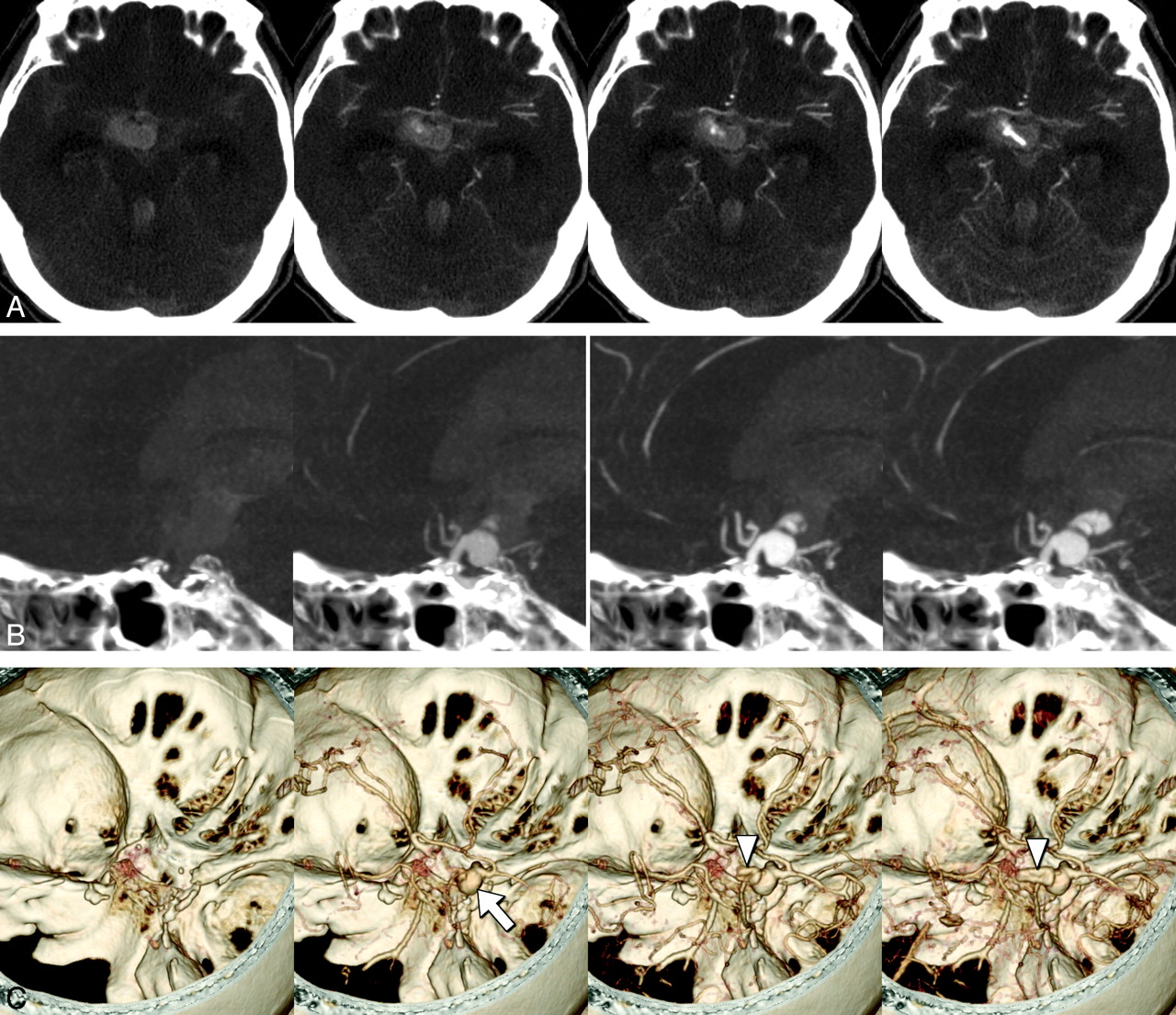
A 68-year-old woman with Claassen grade 4 and WFNS grade 5. A 9-mm aneurysm was identified in the right internal carotid posterior communicating portion by CTA. Contrast extravasation at the third ventricle was suspected on the basis of a CTP source image (A). Active bleeding from an aneurysm penetrating the third ventricle was confirmed with sagittal 20-mm-thickness-slab maximum-intensity-projection images (B), and a volume-rendered image was also useful for assessing the shape of the aneurysm (C, white arrow) and the extent of bleeding (C, arrowheads). Contrast medium in the aneurysm was washed out in the delayed phase, but extravasation was not.

A 52-year-old man with Claassen grade 4 and WFNS grade 5. An irregularly shaped aneurysm 2 cm in diameter was identified at the anterior communicating artery on CTA. Extravasation had a vessel-like shape at the interhemispheric cistern (A, arrow), and spreading contrast extravasation was observed in the left ventricle (B, arrow). On the reconstructed 4D CT images, the aneurysm showed early enhancement and delayed washout (C, arrow), and string-shaped extravasation from the aneurysm penetrated from the interhemispheric cistern into left lateral ventricle without washout (C, arrowheads). Extravasation of contrast medium was also observed on angiography performed in preparation for a coiling procedure. Follow-up CT after 6 hours indicated enlargement of the hematoma.
Extravasation of contrast medium from an aneurysm has been observed in several studies using helical CTA.21⇓⇓⇓–25 In addition, active bleeding from an aneurysm was recently visualized with 4D time-resolved CT angiography.5 Use of multiphase dynamic enhancement can increase the time window for hemodynamic observation, and the evolution of bleeding with time can be demonstrated with a single procedure. The procedure is simple and easy to perform because it requires neither test-injection nor bolus-tracking methods. However, the latest multidetector CT equipment is required to cover a wide scanning area and to suppress radiation exposure by using iterative reconstruction. When multiphase dynamic enhancement is not available, a delayed scan with a short interval after helical CTA takes only a few minutes and may be an alternative method for confirming active bleeding.18
Conclusion
The incidence of active bleeding in our study patients with SAH was 25.5%. Active bleeding was diagnosed by using multiphase dynamic-enhanced CT. All active bleeding events were observed within 2 hours of onset, and patients with SAH with active bleeding had larger hematomas and more severe clinical symptoms than those without active bleeding. These results indicate that awareness of active bleeding in patients with SAH leads to an accurate diagnosis, which, in turn, affects treatment strategies.
Acknowledgments
The authors thank Bierta Barfod, MD, for help in preparing the manuscript.
Footnotes
-
Disclosures: Hidetoshi Kasuya—UNRELATED: Grants/Grants Pending: grant-in-aid for scientific research from the Japanese Ministry of Education.
References
- Received October 4, 2011.
- Accepted after revision November 11, 2011.
- © 2012 by American Journal of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.