
Abstract
BACKGROUND AND PURPOSE: Iterative reconstruction of CT images is characterized by reduced image noise and may allow reduction in radiation exposure. We investigated the influence of an IRT technique on image quality and radiation dose savings when applied to temporal bone CT.
MATERIALS AND METHODS: Based on the typical image quality level of adult subjects using routine radiation dose and FBP, an exsomatized cadaveric head with CNR characteristics closest to the level of clinical subjects was identified. Cadaver acquisitions were performed at multiple levels of tube current exposure. Reconstructions were performed using FBP and IRT (iDose), with multiple iDose levels applied for each acquisition. Transverse and coronal reformations of all reconstructions were evaluated subjectively and objectively. Phantom tests were performed to validate the protocol optimizations with iDose, specifically the spatial resolution relative to routine dose acquisitions. Finally, the results of protocol optimization with iDose were clinically validated in 50 patients.
RESULTS: At the same radiation dose, the image CNR of iDose reconstructions was higher than that of FBP and progressively increased with higher iDose levels. The combination of 100 mAs/section and iDoseL5 was the lowest dose that met the requirements for diagnostic acceptability, with CNR slightly higher than our routine institution protocol of 200 mAs/section with FBP reconstruction. Spatial resolution characteristics were similar between FBP and iDose at all different strengths. The findings were consistent among the cadaver, phantom, and clinical acquisitions.
CONCLUSIONS: The iDose IRT can help reduce radiation dose of temporal bone CT by 50% relative to routine institution protocols with FBP, while maintaining diagnostic image quality.
ABBREVIATIONS:
- CNR
- contrast-to-noise ratio
- CTDIvol
- volume CT dose index
- DLP
- dose-length product
- FBP
- filtered back-projection
- HU
- Hounsfield unit
- IRT
- iterative reconstruction technique
In recent years, the development of multisection CT technology has significantly expanded the diagnostic applications of CT, resulting in an increase in the number of CT examinations performed.1 Because the benefits of CT may exceed the harmful effects of radiation exposure in patients, increasing radiation doses to the population have created a compelling case for reduction of radiation exposure from CT.2 Various methods and strategies based on individual patient attributes and CT technology have been explored for dose optimization. CT manufacturers have implemented improvements in hardware and software,3 such as automatic current exposure control technology. For certain body parts, however, such as the temporal bone, some of these dose-reduction techniques may not apply, due to the limited volume (z-axis) and the need for very high resolution. The use of conventional FBP algorithms poses additional challenges, as these are prone to increased image noise when using lower doses and sharper reconstruction kernels. Iterative reconstruction is an image reconstruction method that has potential benefits over the conventionally used FBP, especially in relation to image noise.4 By making fewer assumptions regarding the noise distribution within an image, noise can be reduced within an image without reducing spatial resolution or image quality and without increasing radiation dose.5 A noise reduction method based on iterative reconstruction, iDose, has been recently developed. With significant improvements in software and hardware design, iDose's reconstruction speed reaches clinically acceptable levels. The purpose of our study was to assess at which dose level an image quality of temporal bone CT, equal to routine dose acquisition with FBP, could be obtained using an IRT.
iDose IRT
iDose (Philips Healthcare, Cleveland, Ohio) is a hybrid IRT that identifies measurements in the projection domain and voxels in the image domain that are likely to cause noise-related artifacts in the image volume, such as low signal intensity streaks and pixel-to-pixel noise. The noisy data are treated in a 2-stage process. First, in the projection domain, only the noisiest projections are processed in an iterative algorithm, which is responsible for streak removal and correction of CT bias errors due to the photon starvation phenomenon. Reconstruction steps that follow produce an image volume with most of the correlated noise removed. Second, the remaining noise, now mostly pixel-to-pixel noise, is further corrected by an image domain noise-reduction process. The process removes noise uniformly at the entire frequency band while preserving the underlying edges associated with the anatomy of the scanned object (Fig 1).

iDose IRT algorithmic description. In the projection space, the iterations remove artifacts through an iterative diffusion process. In the image domain, through the use of noise and structural models, the quantum mottle noise is iteratively removed.
The iDose level is selectable. It reflects a scale (range 1–7) of how aggressively the noise reduction is performed (range 11%–55%) relative to noise that would be obtained if reconstructed with FBP.5
Materials and Methods
Study Design
Institutional review board approval was obtained for this study. The study protocol was performed in compliance with the Health Insurance Portability and Accountability Act. The reference image quality for temporal bone CT acquisitions was established on a set of 50 patients, scanned using routine institutional protocols for radiation dose and conventional FBP reconstruction. Protocol optimizations were then performed through cadaver and phantom experiments. The cadaveric experiments were targeted at identifying the minimum radiation dose at which the iDose reconstructions provided equivalent subjective and objective image quality relative to reference image quality for temporal bone CT. The phantom scans were performed to validate the protocol optimizations determined in the cadaveric studies, particularly the spatial resolution. Finally, the optimization was applied to a second set of 50 patients, and the clinical acceptability was assessed through subjective and objective evaluations.
I. Routine Temporal Bone CT Clinical Image Quality Reference
Fifty consecutive adult patients (age >18 years old; no false teeth; 13 men, 37 women; mean age 42.88 ± 15.03 years) referred for temporal bone CT examination were scanned on a 64-section CT scanner (Brilliance 64; Philips Healthcare) using our routine institutional protocol (140 kVp, 200 mAs/section, pitch 0.685, collimation 16 × 0.625 mm). The approximate CTDIvol indicated by the scanner was 46.9 mGy. All reconstructions were performed using conventional FBP. Axial and coronal images were reformatted according to the standard clinical practice.6 Image quality assessments were performed on a CT postprocessing workstation (Extended Brilliance Workspace; Philips Healthcare). Circular regions of interest of 50 mm2 were placed in the brain stem region and air space lateral to the external auditory canal (Fig 2). Density values (CT#), calculated in HUs, were documented. Noise was measured as the standard deviation in HU within the region of interest selected. Measurements were performed on axial and coronal reformatted images for all 50 patients. The baseline image quality was obtained as the mean CNR value, with CNR computed using the following equation7:
 where CT#brain stem is the mean attenuation measured in the brain stem, CT#air is the mean attenuation measured in the area outside of external auditory meatus, SDbrain stem is the mean noise in the brain stem, and SDair is the mean noise in the area outside of external auditory meatus.
where CT#brain stem is the mean attenuation measured in the brain stem, CT#air is the mean attenuation measured in the area outside of external auditory meatus, SDbrain stem is the mean noise in the brain stem, and SDair is the mean noise in the area outside of external auditory meatus.

Circular regions of interest of 50 mm2 placed in the brain stem region, and air space lateral to the external auditory canal.
II. Optimization of Protocols on Cadaveric Heads
Eight exsomatized cadaveric heads were scanned on the 64-section CT scanner using the routine clinical temporal bone protocol (140 kVp, 200 mAs/section, pitch 0.685, collimation 16 × 0.625 mm). The cadaveric head presenting CNR characteristics closest to the clinical reference was chosen for the protocol optimization experimental study.
With other parameters unchanged, the specimen temporal bone was scanned using 180, 160, 140, 120, 100, 80, 60, and 40 mAs/section. Reconstructions of all acquisitions were performed with FBP and with 7 different noise strengths/levels of the iDose IRT (iDoseL1, iDoseL2, iDoseL3, iDoseL4, iDoseL5, IDoseL6, and iDoseL7). Axial and coronal reformations were created for all reconstructions, resulting in a total of 144 datasets (9 dose levels × 8 reconstructions × 2 reformats). Region-of-interest measurements and CNR computations in the selected similar sections from all of the described image series were performed similar to the technique used in establishing the clinical reference image quality.
All datasets were arranged in random order and subjectively evaluated by 5 experienced radiologists using a 3-point ordinal scale based primarily on noise level, ossicular visualization, mastoid honeycomb structures, osseous spiral lamina of the cochlea, and cortical bone edge. An image quality of grade I was considered to be excellent (5 elements satisfied), with no diagnostic limitations; grade II was of lower quality (at least 3–4 elements satisfied) but did not affect the diagnosis; grade III was very low quality (less than 3 elements satisfied) and may influence the diagnosis. Grade I and grade II images were considered to be of diagnostic image quality.
III. Validation of Optimized Protocols on Phantom
A 3D spatial resolution test phantom (IBA Dosimetry, Schwarzenbruck, Germany) was scanned on the 64-section CT scanner using the optimized protocol determined from the cadaver study (140 kVp, 100 mAs/section, pitch 0.685, collimation 16 × 0.625 mm). Reconstructions were performed with FBP and 7 different noise strengths/levels of the iDose IRT (iDoseL1, iDoseL2, iDoseL3, iDoseL4, iDoseL5, IDoseL6, and iDoseL7). Visual assessment of the spatial resolution was performed on all reconstructions.
IV. Clinical Validation
Fifty consecutive adult patients (older than 18 years; no false teeth; 13 men, 37 women; age 38.94 ± 14.26 years) were scanned on the 64-section CT scanner using the optimized scan and reconstruction (iDose) parameters combination determined from the cadaver and phantom studies. Axial and coronal reformations were created, and CNR measurements consistent with the technique used previously in the study were performed. Three experienced radiologists, using the 3-point ordinal scale previously used, subjectively evaluated the image quality.
V. Radiation Dose
The DLP for each scan was calculated using the indicated CTDIvol by the CT system and the scan length. The effective dose, E, is related to the DLP as follows:
 where the unit of DLP is mGy/cm and k is the region-specific normalized effective dose conversion factor of 0.0031 (mSv mGy−1 cm−1) for the head and neck (including the temporal bone).
where the unit of DLP is mGy/cm and k is the region-specific normalized effective dose conversion factor of 0.0031 (mSv mGy−1 cm−1) for the head and neck (including the temporal bone).
Results
Cadaver Test: Influence of iDose Reconstruction on CT Attenuation and Noise
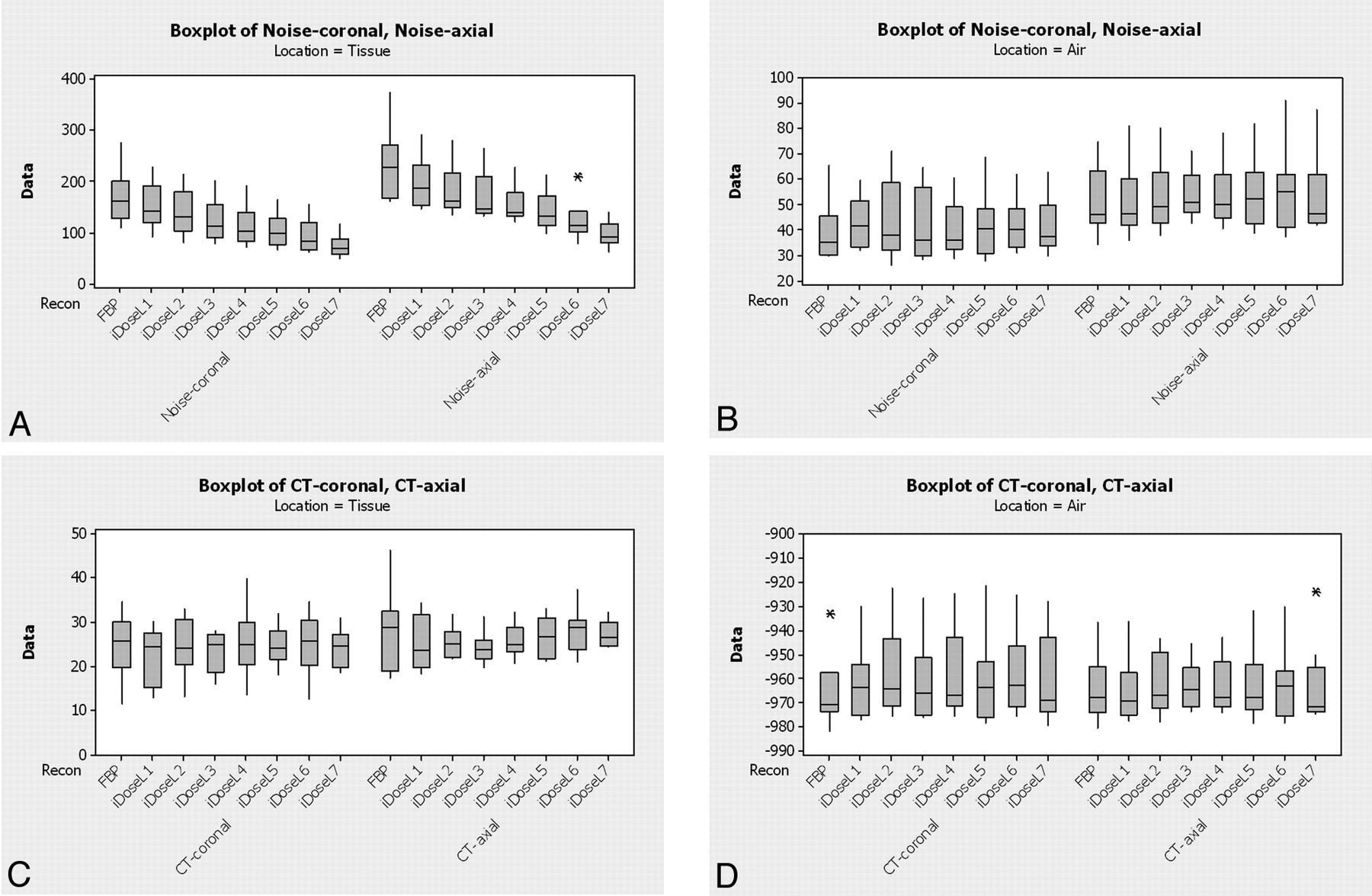
Comparison of the pooled noise (across all radiation doses) between the FBP algorithm and the different iDose strengths/levels demonstrated that iDose images had lower overall tissue noise (SDbrain stem) relative to FBP, and the noise progressively reduced with increasing strengths/levels of iDose (Fig 3A). There was no noticeable trend in influence of reconstruction technique on noise in air (SDair), attenuation of tissue (CTbrain stem), and attenuation of air (CTair) (Fig 3B–D). The overall image noise was relatively higher on the axial images compared with coronal images. However, the trend in influence of reconstruction technique was similar between axial and coronal images.
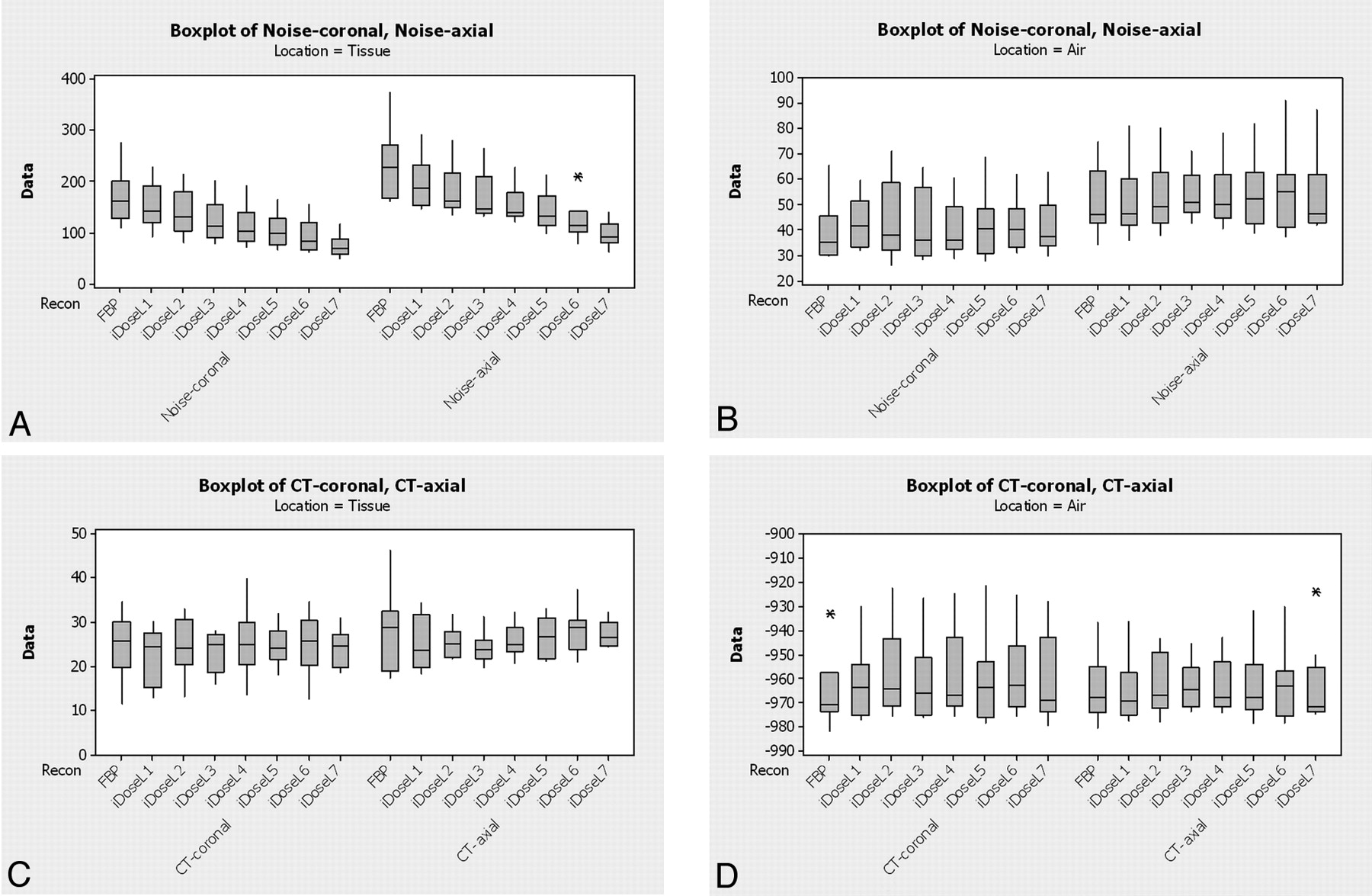
Influence of reconstruction technique on the pooled measurements (attenuation and noise) across all radiation doses.
Cadaver Test: Influence of iDose Reconstruction on CNR
For a given radiation dose (mAs/section), iDose datasets had higher CNR than FBP, and the CNR progressively increased with increasing strengths/levels of iDose. When changing the effective mAs, CNR generally increased with increasing radiation dose (Fig 4). The reference image quality (CNR of 10 when 200 mAs with FBP) can be obtained at all dose levels using at least 1 iDose strength/level except the 40mAs acquisition.
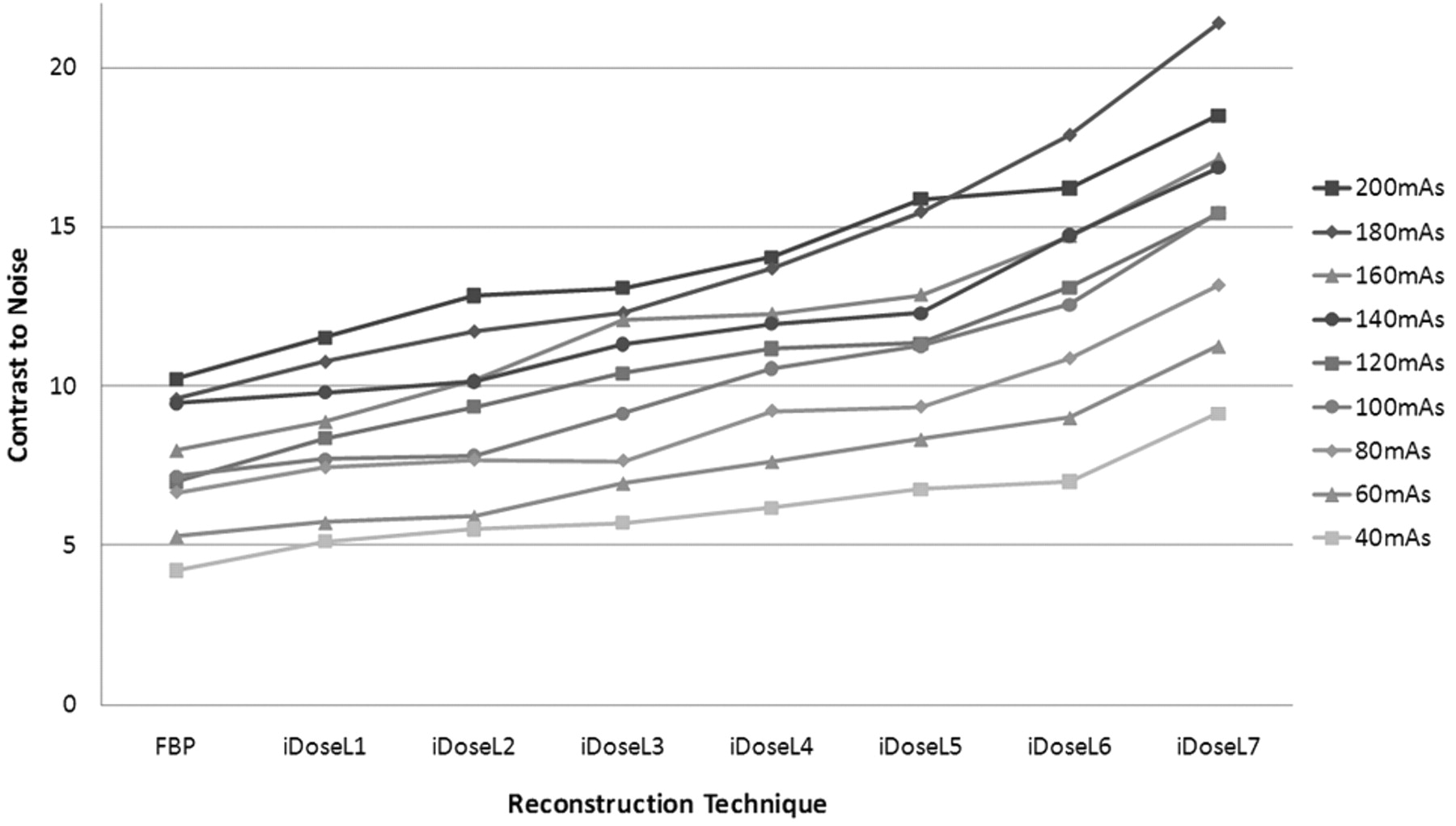
The relationship between reconstruction technique and the average CNR (CNR[axial + coronal])/2) in temporal bone CT on cadaver heads with different dose.
Cadaver Test: Subjective Evaluation by Readers
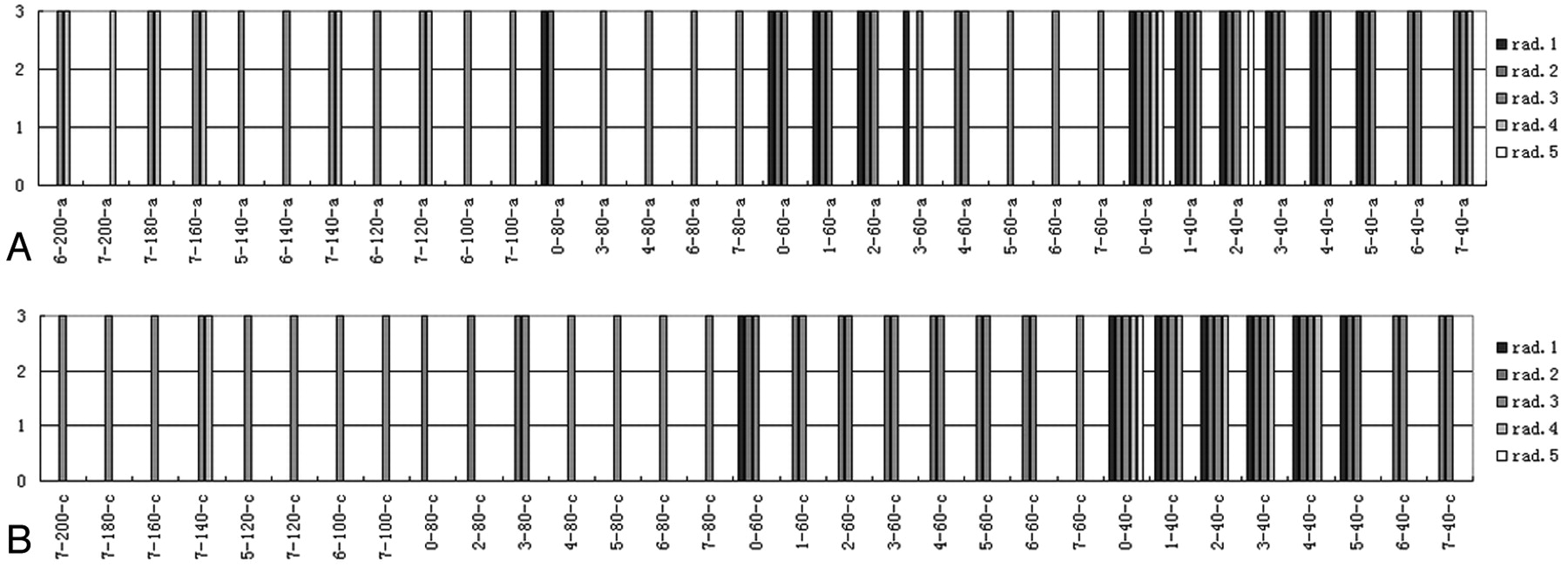
When the effective mAs were 80, 60, or 40 mAs/section, observers generally agreed that the images with various reconstruction algorithms were not suitable for diagnosis and graded them as III (Fig 5). For all dose levels, even using 180 or 200 mAs/section, the reconstructed images using iDoseL6 or iDoseL7 were not preferred, and some readers considered them not suitable for diagnosis.

Distribution of cadaver scans graded as III by 5 radiologists for different dose levels and reconstructions. Vertical axis of the coordinate is the subjective score and horizontal axis is image series. Every image dataset is titled with components of algorithm-effective mAs–section. Numbers from 1–7 are for iDose levels, 0 for FBP algorithm, “a” for the axial section, and “c” for the coronal section. Image quality grade of I is considered to be excellent, with no diagnostic limitations; grade II was of lower quality but did not affect the diagnosis; grade III was very low quality and may influence the diagnosis.
Optimized Protocol
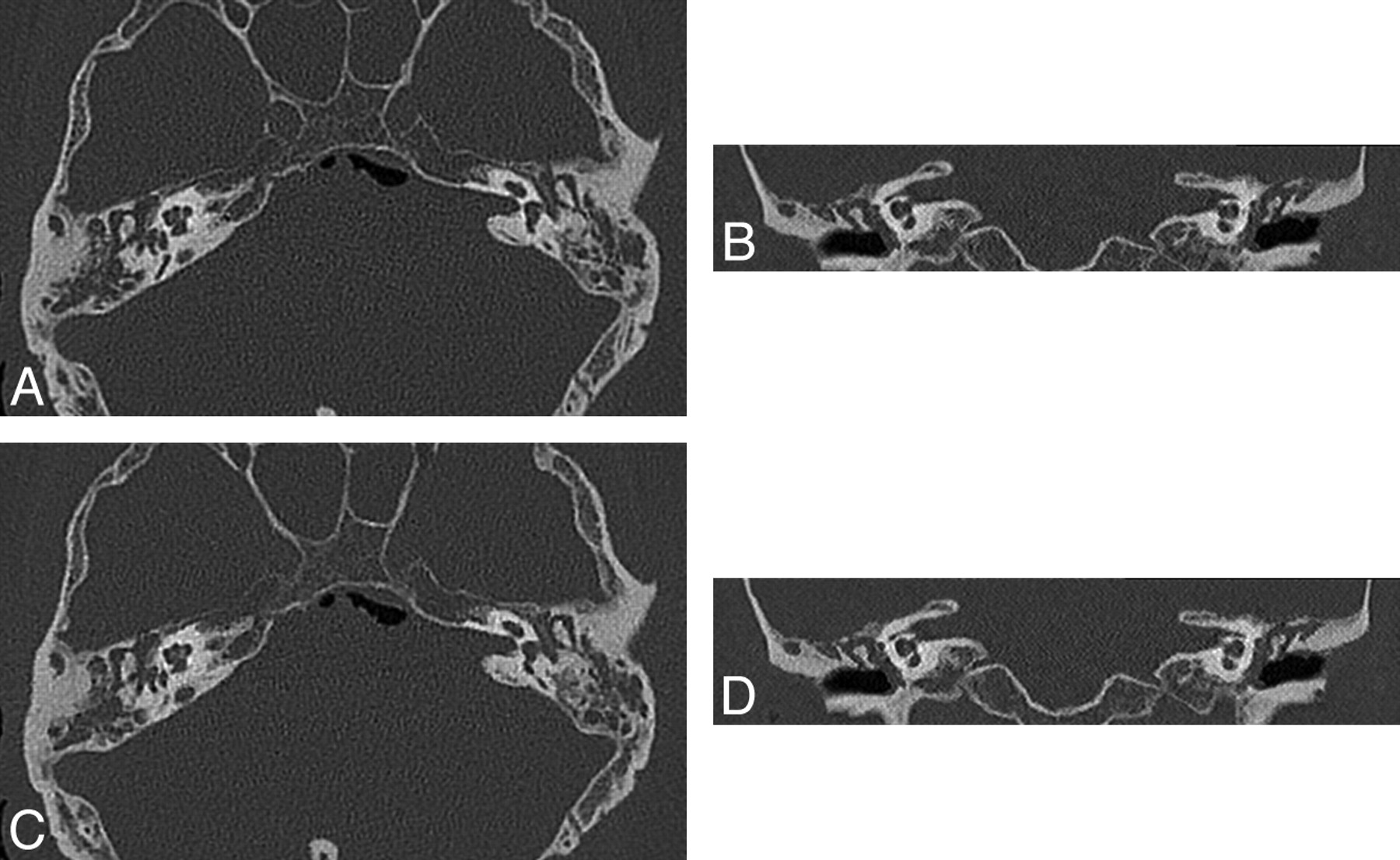
Cadaver acquisitions at 100 mAs/section with iDoseL5 were considered to have diagnostically equivalent image quality relative to the reference institution protocol of 200 mAs/section with FBP, based on the reader scores for image acceptability (Fig 6). Further dose reduction resulted in nondiagnostic image quality. Quantitative CNR measurements on the axial and coronal images demonstrated relatively higher CNR on the optimized protocol relative to reference (Table).
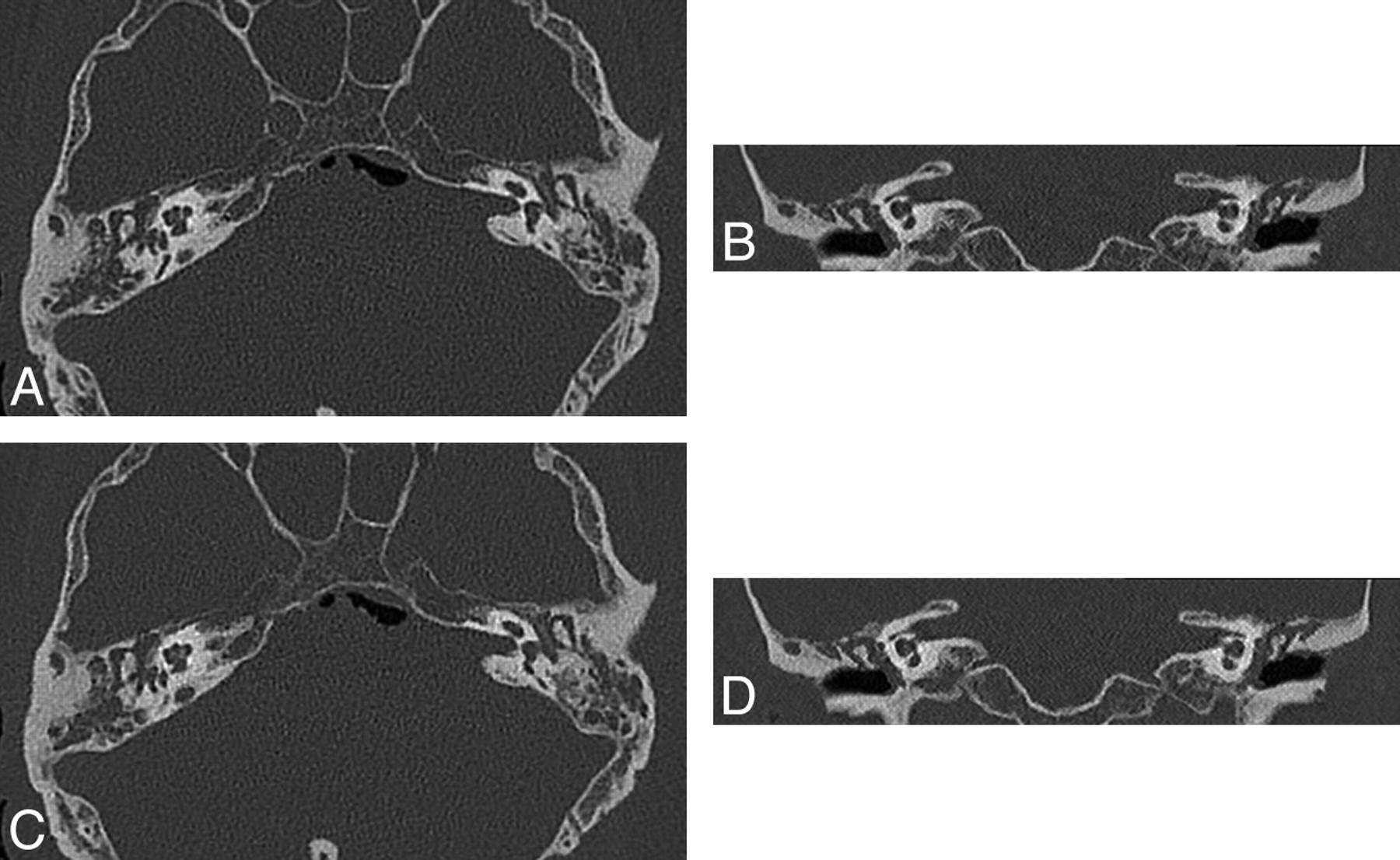
Axial and coronal reformatted images of cadaver head (A, B) reference protocol of 200 mAs/section with FBP (C, D) optimized protocol of 100 mAs/section with iDoseL5.
CNR and dose comparison between reference (FBP) and optimized (iDoseL5) protocol groups
Phantom Test: Image Quality
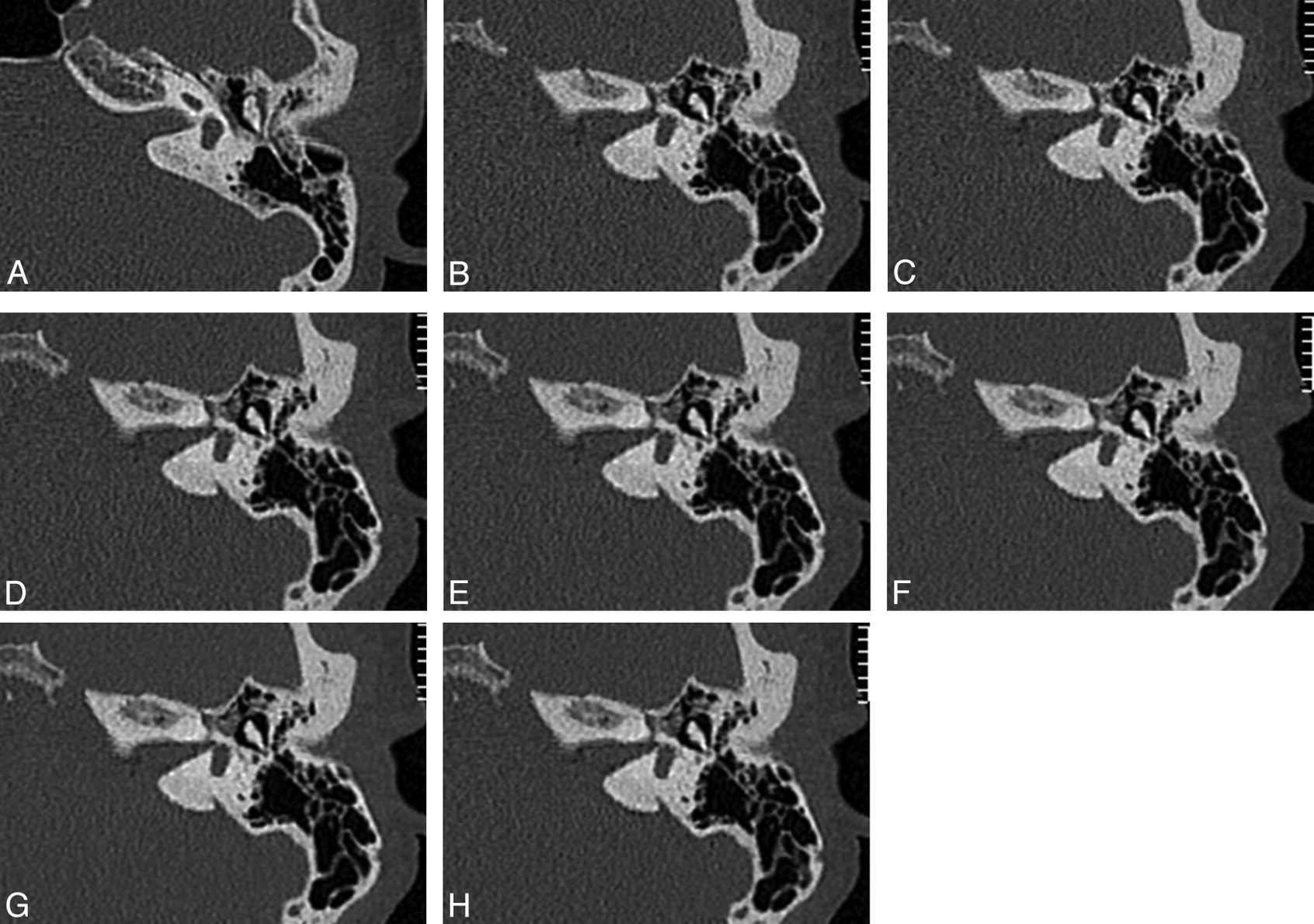
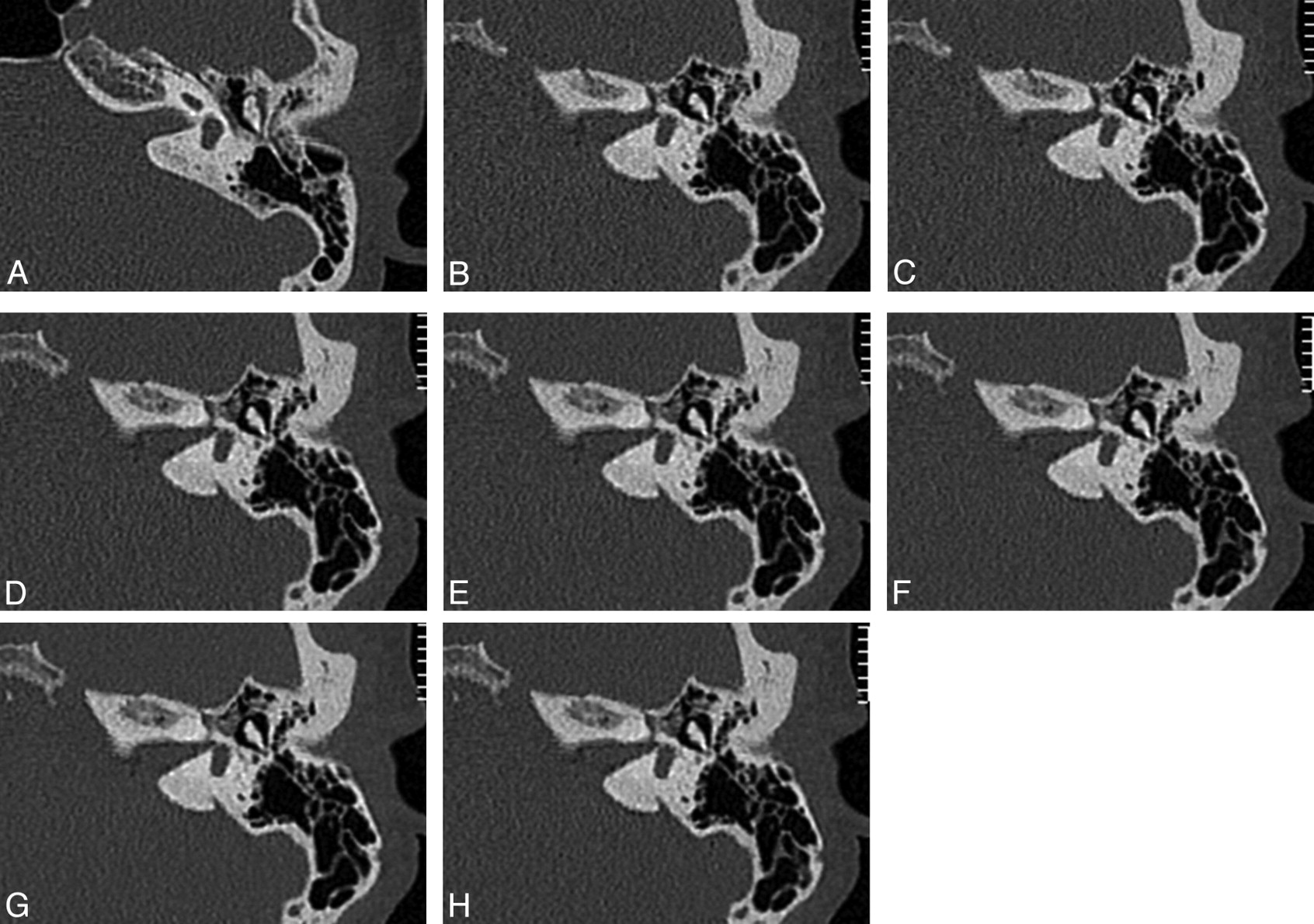
Consistent with findings from cadaver studies, the iDose images had lower noise relative to FBP, and the noise progressively reduced with increasing strengths/levels of iDose (Fig 7). Minimum distinguishable hole size was 0.6 mm on all axial reconstructions, demonstrating that spatial resolution did not change between FBP and the different iDose levels. Findings were similar for coronal images. At higher iDose levels, due to the lower image noise, the spatial resolution boost (white hyperenhancement) around the holes was more apparent.
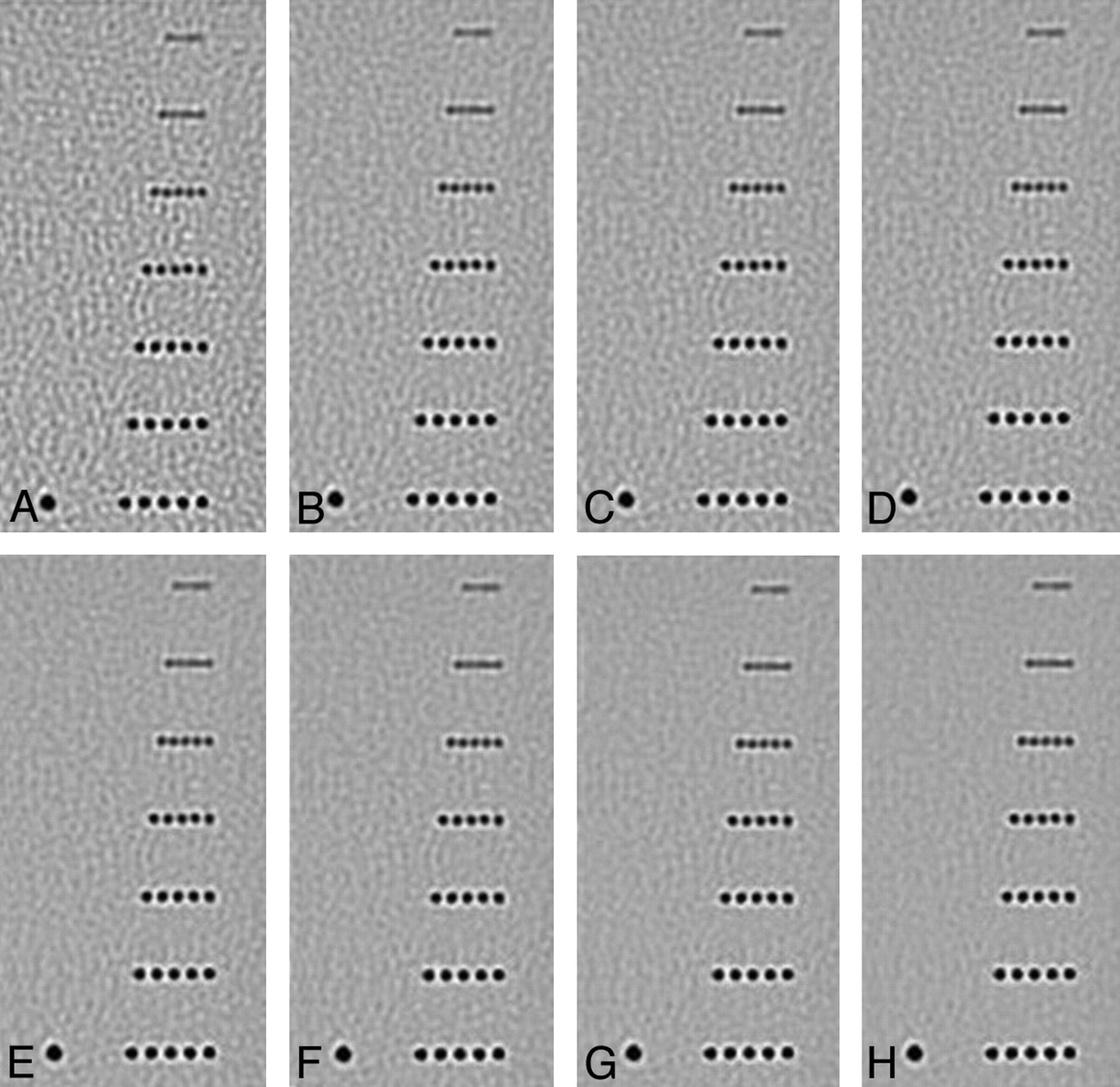
Axial reformatted images of 3D spatial resolution phantom with different reconstruction algorithms. (A) FBP; (B–H) iDose levels 1 to 7, in increasing order.
Clinical Acquisitions with Optimized Protocol
The clinical acquisitions with optimized protocol (100 mAs/section with iDoseL5) were graded as diagnostically equivalent to routine institution protocols (200 mAs/section with FBP) when rated by 3 independent readers (Fig 8). Quantitative CNR measurements between the 2 groups of patients demonstrated slightly higher CNR when using the optimized protocols (Table).
Comparison of axial temporal bone images of routine institution protocol and optimized protocol. A, Female, 42 years old, scanned with 200 mAs/section and FBP reconstructions; B–H, female, 45 years old, scanned with 100 mAs/section and iDose L1 to L7 reconstructions.
Discussion
FBP has been used as the algorithm of choice for CT image reconstruction over the past few decades,8 as this analytic method is a fairly robust and fast reconstruction technique. FBP reconstruction of an acquisition with low SNR, however, produces excessive noise and artifacts. IRTs are known to overcome this challenge through an optimization process whereby the noisiest measurements are weighted low in the iterative updates and therefore contribute very little to the final image, resulting in improved image quality independent of the dose. This benefit is most apparent in low-dose acquisitions, where noise obscures visualization of clinically relevant information. Its implementation into routine clinical practice has been limited, however, by the computationally intensive nature of the algorithm, which results in clinically unacceptable image reconstruction times. With increasing computational power, IRT is moving to the forefront of research in CT.9⇓–11 CT manufacturers have recently made IRT commercially available, and a broad range of clinical applications has been demonstrated.12,13
IRT has several advantages, including fewer projection data requirements and imaging using incomplete and low SNR (low-dose) data.14 In clinical studies by Hara et al,15 IRT was shown to help decrease radiation dose by 32%–65% relative to FBP, with no degradation in image quality. Heilbron and Leipsic16 used IRT to lower the radiation dose in coronary CTA to under 1mSv. Although there have been reports on the use of IRT to improve image quality and dose reduction in CT, this is, to our knowledge, the first investigation of the ability of IRT to reduce radiation dose for temporal bone CT. In our study, we found that the iDose reconstruction provided lower image noise relative to FBP, indicating that IRT had good CNR improvement capabilities. The extent of improvement depended largely on the iDose strength/level used in the reconstruction. With higher iDose level, for example, we found lower noise and higher CNR, but we also found unnatural image appearance, such as discontinuous cortical bone. A dose reduction of 50% was feasible for temporal bone CT, while still maintaining the subjective (Fig 5) and objective (Table) image quality metrics. An iDose level of 5 was considered to be optimal at this dose reduction level.
The noise and artifact characteristics of IRT are different from those of FBP. In the investigation by Prakash et al,17 IRT applied to abdomen and chest CTs helped reduce radiation dose by 25.1% and 27.6%, respectively, but 39% of the IRT images had mild speckle artifacts. In our study, use of iDose levels 6 and 7 (noise reduction ≥45%, relative to FBP) typically resulted in a shift in the appearance of the images. Because the use of these levels provided the most reduction in background noise, the temporal bone structures appeared unnatural, with discontinuous cortical bone or serration artifacts, and fuzzier small joints and fine structures; this degraded overall image quality and, to a certain extent, affected interpretation. Radiologists are accustomed to FBP image appearance and the associated image quality trade-offs. Consequently, IRT may give an impression of somewhat reduced diagnostic value in certain cases, especially when used aggressively. The appropriate IRT strength depends, to some extent, on the dose reduction that is being applied to the acquisition; lower strengths for lower dose reduction and higher strengths for higher dose reduction. The interobserver agreement on the acceptance levels of IRT strengths was somewhat low. Some readers considered the images of the 200 mAs/section and iDoseL6 combination to be unacceptable for clinical diagnosis, while some thought the images of 40 mAs/section and iDoseL7 combination could still be used (Fig 5). Radiologists will need time and experience to adapt to the appearance of images reconstructed with IRT.
Analysis of the reader image quality assessment showed that the scores for coronal reformatted images were better than for axial images, that is, the number of axial images graded as class III (nondiagnostic) was higher than that of coronal images. Further investigation showed that the primary reason for this was that the coronal images were reformatted from the original axial images, and in the process of reformatting, an interpolation was applied. The interpolation applied in the reformatting process resulted in difference in voxel resolution between the axial (0.35 × 0.35 × 0.35 mm) and coronal (0.35 × 0.35 × 0.67 mm) images. Hence, any changes caused by the reconstruction technique or dose reduction are more apparent on the axial images and are minimized on the coronal images. This also explains the relatively higher CNR on the coronal images compared with the axial images for the same acquisition and reconstruction parameters.
The temporal bone has fine anatomic structures that demand higher spatial resolution than most other clinical targets. Image noise and spatial resolution are 2 conflicting factors, because reconstruction typically treats all signal intensity (high resolution and noise) equally, hence increasing the noise proportional to the resolution of the reconstruction.18 IRT has been shown to have comparable spatial resolution compared with FBP,14 with the primary advantage being the lower noise. Our phantom experiments demonstrated that the minimum diameters of distinguishable holes in iDose reconstructions were the same as the FBP datasets. Because iDose level 6 and level 7 provide the maximum noise reduction, they give the perception of reduced spatial resolution on some structures, which is not desirable for temporal bone CT.
The main limitation of our study is that we were able to assess only the iDose (Philips) product. There are 3 other vendors offering similar technical solutions, and we have not investigated whether the other products are equally efficient or even more efficient than iDose. Nonetheless, the experimental methods described herein may be used as a means to select optimal scanning parameters and level of iterative algorithm for CT users of different manufacturers.
Conclusions
Our cadaver, phantom, and clinical experiments suggest that the use of IRTs can help reduce radiation dose from temporal bone CT by 50% relative to routine institution protocols with FBP, while maintaining diagnostic image quality.
Footnotes
Disclosures: Dhruv Mehta—UNRELATED: Employment: Philips Healthcare, Comments: Current employment as Research Scientist at Philips Healthcare. The extent of the work on the study was literature review, and providing information on the technology that is reported in the manuscript.
References
- Received July 15, 2011.
- Accepted after revision September 29, 2011.
- © 2012 by American Journal of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Full Dose-Reduction Potential of Statistical Iterative Reconstruction for Head CT Protocols in a Predominantly Pediatric Population
- Temporal Bone CT: Improved Image Quality and Potential for Decreased Radiation Dose Using an Ultra-High-Resolution Scan Mode with an Iterative Reconstruction Algorithm
- Six iterative reconstruction algorithms in brain CT: a phantom study on image quality at different radiation dose levels