
Abstract
SUMMARY: We report the unique CNS findings in a patient with a proximal chromosome 14q interstitial deletion. Conventional MR imaging allowed the clear delineation of agenesis of the corpus callosum, SOD, and diffuse lissencephaly. DTI tractography played a significant role in the evaluation of the proximal 14q deletion−associated abnormalities, delineating the extent of the dysmorphic connections of the Probst bundles and clarifying that apparent areas of heterotopias were the corticospinal tracts.
ABBREVIATIONS:
- FA
- fractional anisotropy
- SOD
- septo-optic dysplasia
The evaluation of congenital malformations of the CNS has markedly evolved in the past decade with the ability to evaluate the associated underlying chromosomal abnormalities and to use DTI to investigate the morphologic brain changes. These tools allow development of deeper insight into the potential genetic ictus of certain malformations and a clearer analysis of the resulting morphologic brain changes. We report a patient with chromosome 14q deletion who has SOD, agenesis of the corpus callosum, and extensive lissencephalic brain abnormalities. DTI tractography helped to delineate the underlying brain abnormalities by demonstrating the location of the white matter tracts.
Case Report
The patient is a 4-month-old boy born of a dizygotic twin pregnancy at 32 weeks' gestation. Prenatal sonography demonstrated cerebral ventriculomegaly. A prenatal MR imaging demonstrated absence of the corpus callosum, lack of development of the normal sulci, ventriculomegaly, and minimal hypoplasia of the inferior vermis. The mother was 25 years old with 2 previous early pregnancy losses and presented in labor; despite attempts to delay delivery, labor progressed. At birth, dysmorphic facial features and microcephaly were noted in the neonate. He had mild micrognathia, low-set ears, and a high narrow palate. Sonography of the head was performed after birth and showed absence of the corpus callosum. The patient had SOD presenting as decreased cortisol production, hypothyroidism, and optic nerve hypoplasia. He was also found to have anomalous innominate artery syndrome, tracheomalacia, bronchopulmonary dysplasia, hypospadias, difficulty with respiratory function, and seizure disorder. Karyotype showed an interstitial deletion of the proximal portion of the long arm of chromosome 14, with breakpoints at 14q11.2 and 14q21[46,XY,del(14)(q11.2q21.2)]. On 44K microarray, the deletion was confirmed to be 18.4 MB.
A brain MR imaging examination was performed at 1.5T (Intera 12.6, level 1; Philips Healthcare, Best, Netherlands). Images obtained included sagittal T1-weighted, axial T2-weighted, axial T2 fluid-attenuated inversion recovery, coronal T2-weighted, and a DTI sequence (TR, 4699 ms; TE, 68 ms; bandwidth, 24 Hz; acquired voxel 2 × 2 mm; reconstructed voxel, 1.75 × 1.75 mm; FOV, 180 × 180 mm; section thickness, 3 mm; section gap, 0 mm; number of signal averages, 3; sense factor, 2; b=800; directions of gradient sampling, 16; scanning time, 3 minutes, 60 seconds). The DTI sequence was registered so the successive series were compared and any motion was corrected. The fiber tracts were created on MR Extended Workspace (EWS release 2.5.3.0, Philips Healthcare) using the fiber tracking option. Fiber tract parameters were the following: FA minimum cutoff, 0.15; minimum fiber length, 10; angle changes, <27° for the corticospinal tract; and angle changes, <45° for the Probst bundles. A 2-region-of-interest method was used to create all of the fiber tracts.
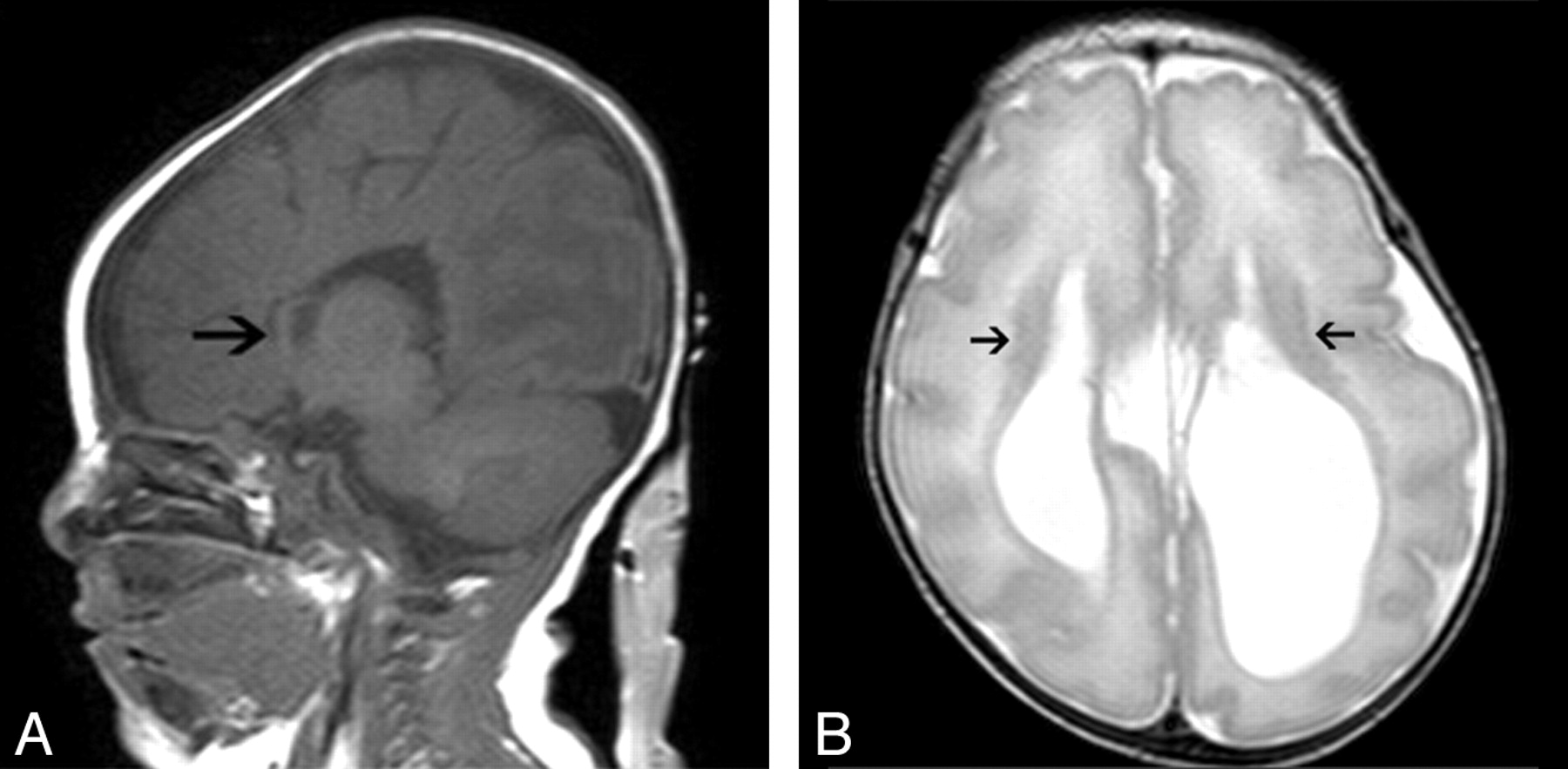
The MR images demonstrated agenesis of the corpus callosum, posteriorly enlarged lateral ventricles with parallel orientation (colpocephaly), agenesis of the cingulate gyrus, absence of the septum pellucidum, lateral displacement of the fornices, atrophy of the optic chiasm, minimal hypoplasia of the inferior vermis, and extensive lissencephaly with possible heterotopias along the ventricular wall (Fig 1). DTI tractography further confirmed agenesis of the corpus callosum, along with formation of Probst bundles having dysmorphic and extensive connections to the temporal lobes and anterior internal capsules (left > right) (Fig 2 A−C). DTI fiber tract analysis also showed that the foci of periventricular signal-intensity abnormalities initially thought to be heterotopias actually represented the corticospinal tracts (Fig 2D).

A, Sagittal T1-weighted image demonstrates agenesis of the corpus callosum. The anterior curvilinear area of soft tissue does not represent the corpus callosum but represents partial voluming with the anterior aspect of the fornix (arrow). B, Axial T2-weighted image at the level of the body of the lateral ventricles. No evidence of the corpus callosum is present. The lateral ventricles have a parallel configuration with dilation of the occipital horns (colpocephaly). The gyri are noted to be diffusely thickened and decreased in number, the Silvian fissures are wide, and the sulci are diffusely shallow. These findings are consistent with lissencephaly. Isointense-to–gray matter bands line the ventricles, and these were initially thought to be heterotopias (arrows).

A, Axial view of the Probst bundles in 3D superimposed on a directionally color-coded axial FA map of the brain. Green indicates anterior-to-posterior; red, left-to-right; and blue, superior-to-inferior predominant water motion. B, Left Probst bundle superimposed on a sagittal T1-weighted image demonstrates the anterior-to-posterior and superior-to-inferior projections of the fiber tract. C, Coronal color-coded FA map demonstrates the green anterior-to-posterior-coursing Probst bundles with no separate bundles identifiable as cingulate bundles (arrows). D, Axial T2-weighted image with cross-sectional representation of the left (red) and right (pink) corticospinal tracts.
The patient's twin was healthy. His mother and father had normal chromosome study findings. They were provided with genetic counseling regarding the patient's de novo chromosome deletion.
Discussion
Previous reports of proximal 14q deletions have been made, but it is an extremely rare occurrence. However, none have the specific chromosome deletion or the combination of CNS malformations as in our case. SOD has not been previously described, to our knowledge; and lissencephaly has been described only once in prior reports of cases with proximal 14q deletion.1 Also, the MR images of the reported case with lissencephaly were not presented, but the description of the imaging findings significantly differed from those in our patient.1 DTI tractography was used in the evaluation of our patient (Fig 2). This allowed better visualization of the aberrant white matter connections, which are often found in congenital CNS malformations and are not visualized with conventional MR imaging. DTI tractography allowed us to better evaluate the morphologic changes associated with agenesis of the corpus callosum. With DTI tractography, we visualized fibers from the hemispheric cortex failing to cross the midline and forming thick bundles running anteroposteriorly to become Probst bundles.2
Agenesis of the corpus callosum results in failure of association fibers to decussate to the contralateral hemisphere due to lack of induction by the massa commissuralis. The Probst bundle is formed from the development of association fibers, which do not pass through the callosal precursor and then continue to grow caudally along the medial surface of the ipsilateral cerebral hemisphere.3 Tractography in our patient demonstrated the Probst bundles as having prominent connections to the temporal lobes. Also, fibers were visualized extending into the anterior internal capsules on the left greater than on the right (Fig 2).This degree of temporal lobe and internal capsule connections has not been previously reported, though variability of Probst connections has been noted.2–7 The Probst connections that we have visualized may be an indication of the variability that can exist with their formation. However, tractography of the Probst bundles may also be demonstrating white matter connections of the cingulate gyri to the temporal lobes secondary to the cingulate bundles not being separated from the Probst bundles. Many attempts were made by tractography to separate the cingulate bundle from Probst bundle without success. Furthermore, our tractography findings may indicate spurious fiber tract connections resulting from performing fiber tractography in a 4-month-old with incompletely myelinated white matter. It would be interesting to see if the appearance of the Probst bundles in this subject changes with age.
DTI tractography also allowed us to determine the true nature of the suspected heterotopias found running adjacent to the lateral ventricles as actually being corticospinal tract fibers (Fig 2D). The isointense-to–gray matter T2 signal intensity associated with the corticospinal tract makes it similar in signal intensity to the gray matter; hence, the heterotopic appearance is hypothesized to be due to myelination of the corticospinal tract.
In conclusion, this is a case report of previously undescribed and rarely described findings associated with a proximal 14q deletion that included SOD and lissencephaly.1 Conventional MR imaging allowed excellent delineation of agenesis of the corpus callosum with the associated findings and the presence of diffuse lissencephaly. However, DTI tractography played a significant role in the evaluation by delineating the extent of potential dysmorphic connections of the Probst bundles and clarifying that apparent areas of periventricular heterotopias were in fact the corticospinal tracts.
References
- Received September 7, 2010.
- Accepted after revision October 26, 2010.
- © 2012 by American Journal of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.