
Abstract
SUMMARY: The balloon remodeling technique was initially designed for the endovascular treatment of anatomically complex aneurysms, specifically wide-neck aneurysms. A nondetachable balloon is inflated in front of the aneurysm neck during coil deposition and removed at the end of the procedure. Some controversies regarding the safety of the technique were introduced by the recent publication of a series showing a much higher rate of complications with the remodeling technique compared with the standard coiling technique. However, recent data from the literature review and from the large ATENA and CLARITY series show that the safety of standard coiling and remodeling is quite similar. Anatomic results are also probably better after remodeling. Finally, due to equivalent safety and better anatomic results, the remodeling technique can be widely used in the management of both ruptured and unruptured aneurysms.
ABBREVIATIONS
- ATENA
- Aneurysms Treated by Endovascular Approach
- CLARITY
- clinical and anatomic results in the treatment of ruptured intracranial aneurysms
- CHU
- Centre Hospitalier Universitaire
- EVT
- endovascular treatment
EVT with coils is widely used in the management of intracranial aneurysms.1 However, endovascular treatment can be technically difficult for anatomic reasons, particularly when the neck is wide or when the dome-to-neck ratio is not favorable. In 1994, Moret et al2 described the remodeling technique for extending the indications and feasibility of the endovascular treatment to wide-neck intracranial aneurysms. A few monocentric series were published analyzing clinical and anatomic results of this technique.3–9 However, in several of these series, no direct comparison between standard coiling and remodeling was available. Moreover, in most of the literature, ruptured and unruptured aneurysms were mixed, and a separate analysis of the safety and efficacy in both situations was not possible. A literature review was published in 2008.10 A direct comparison of the standard coiling technique and remodeling was recently conducted in both ruptured and unruptured aneurysms in 2 large multicentric prospective series.11,12
The publication by Sluzewski et al in 20069 suggested that the remodeling technique was associated with a high complication rate and should be used only if the standard coiling technique was impossible or had failed.
To know accurately the place of the remodeling technique (also called balloon-assisted coil embolization) in the endovascular treatment of intracranial aneurysms, a precise analysis of its feasibility, safety, and efficacy is now needed.
What is the Remodeling Technique?
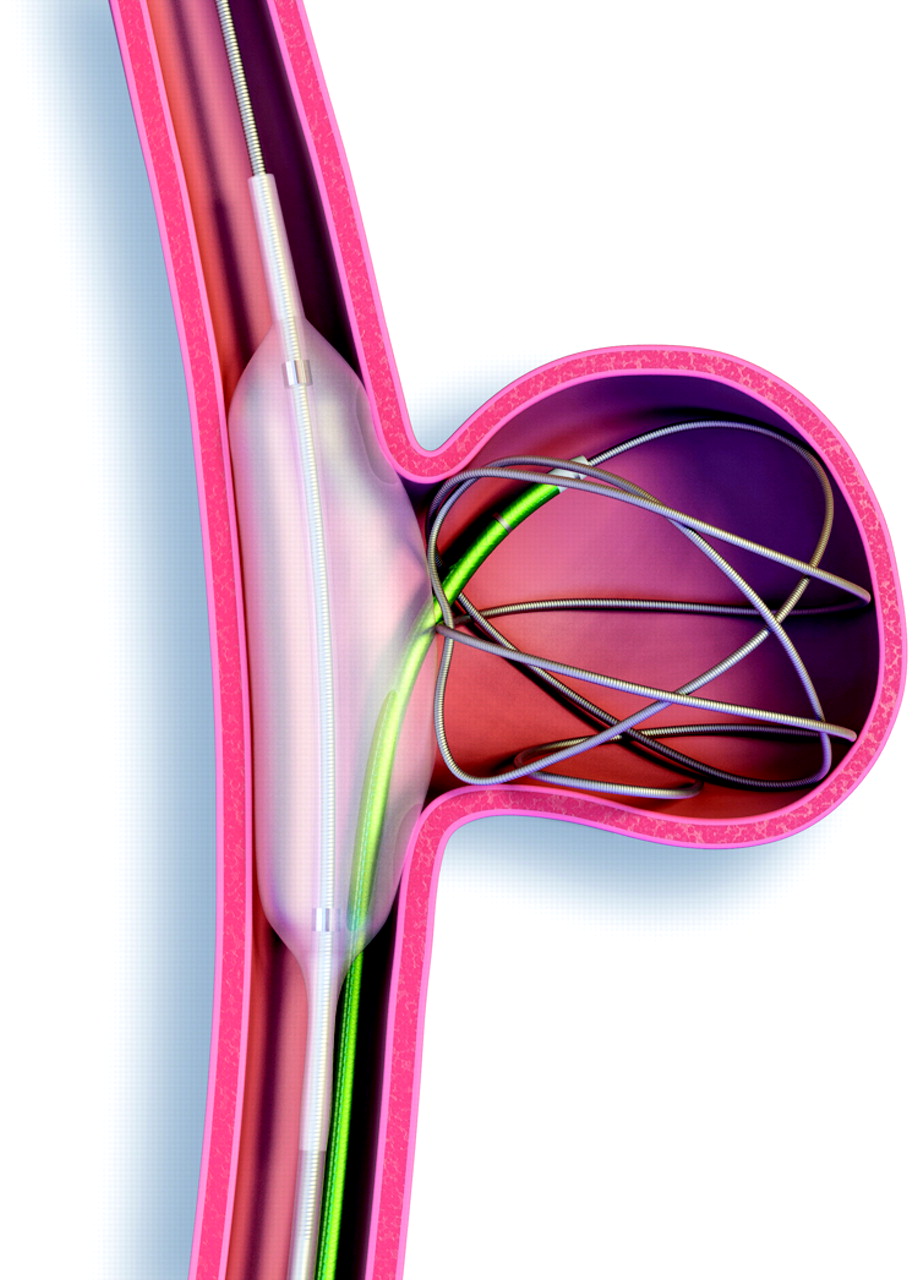
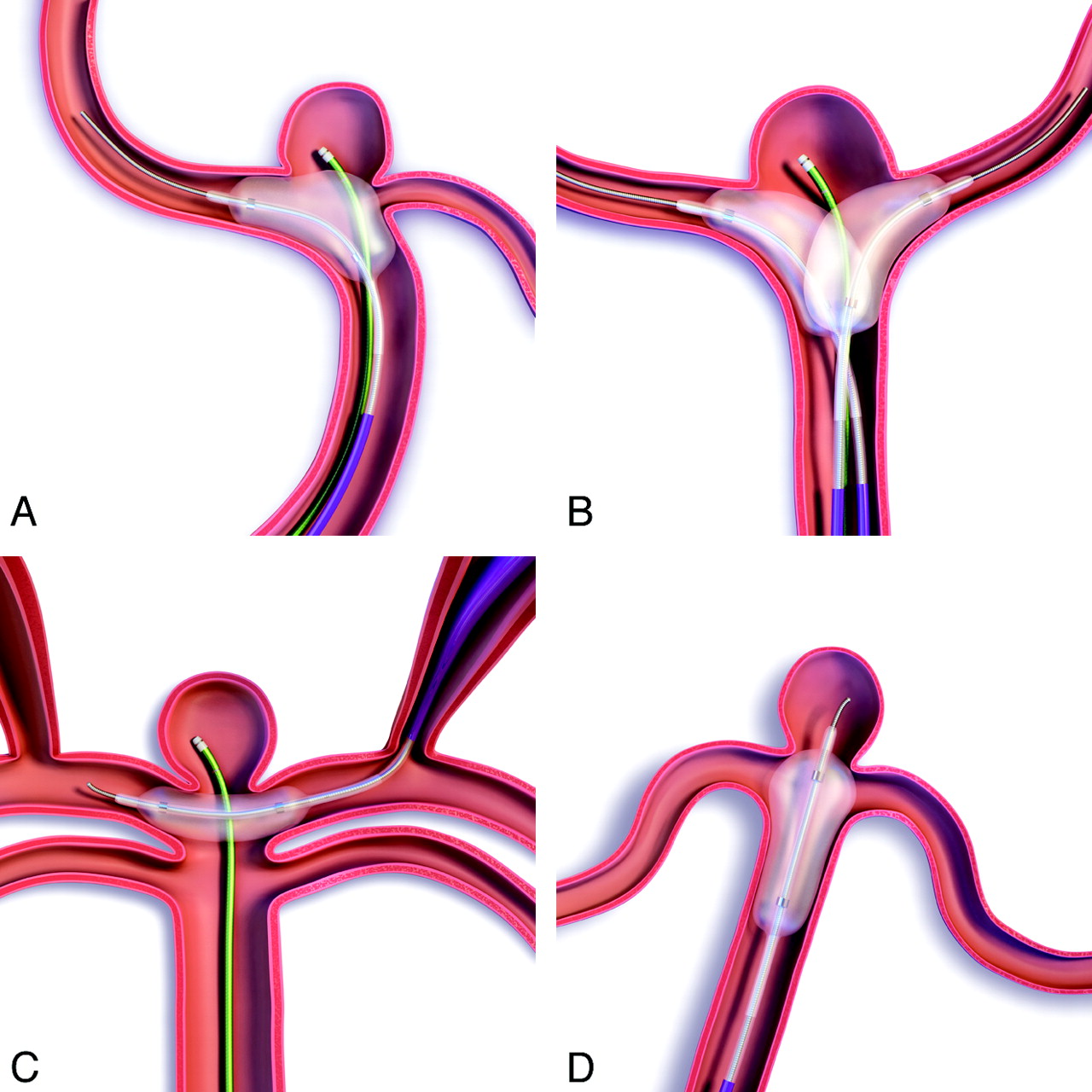
A nondetachable balloon is temporarily inflated in front of the neck of the aneurysm during each coil placement (Figs 1 and 2). At the end of the procedure, the remodeling balloon is removed and no device is left in place in the parent vessel (unless stent placement is subsequently performed).

Remodeling technique for sidewall aneurysms.
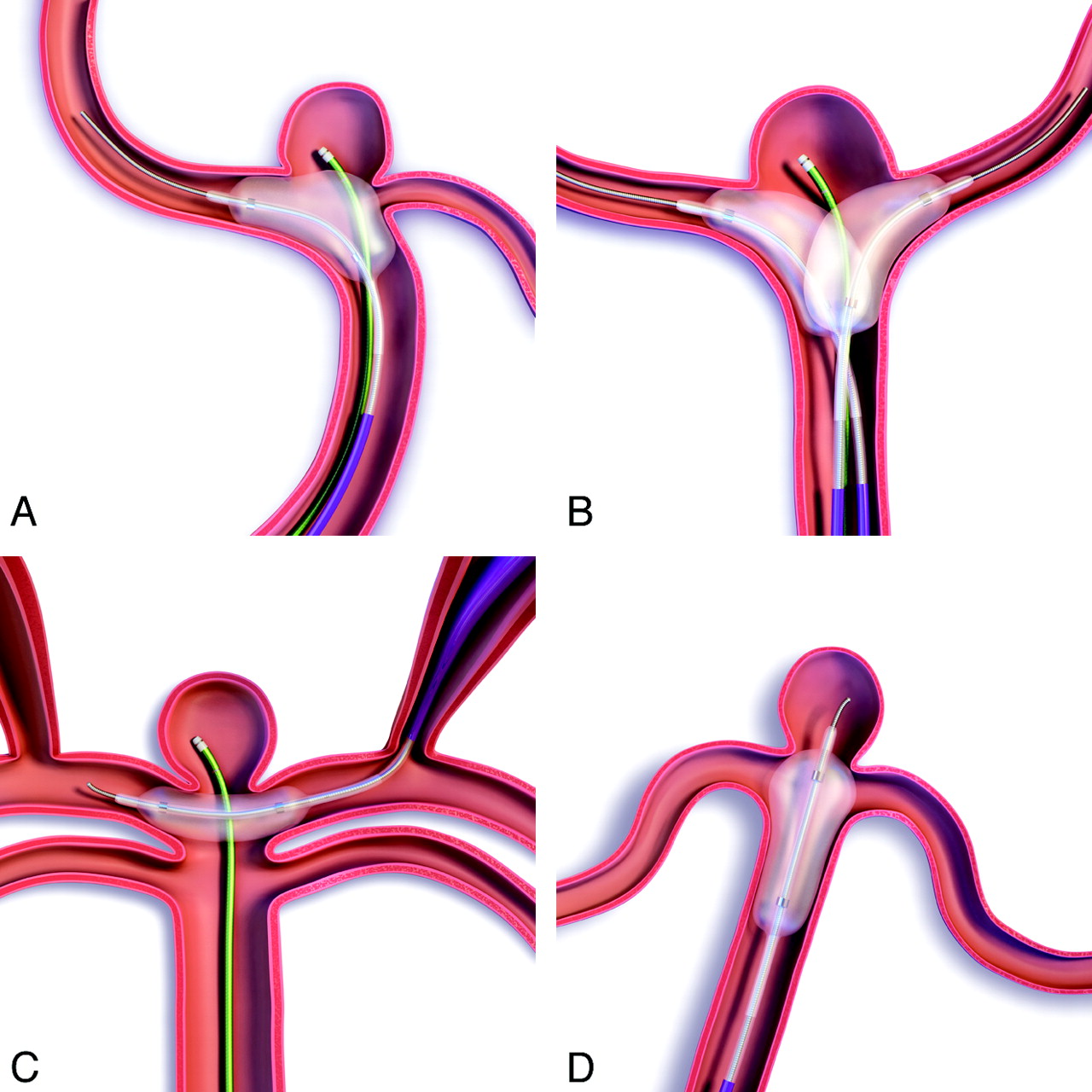
Remodeling technique for bifurcation aneurysms. A, Use of a pear-shaped balloon. B, Double-balloon technique. C, Placement of the remodeling balloon parallel to the aneurysm neck by using circle of Willis anastomosis. D, Use of a double-lumen remodeling technique.
In sidewall aneurysms, the balloon is simply placed in the parent vessel in front of the aneurysm neck (Fig 1). In bifurcation aneurysms, the situation is more complex because it is necessary to completely protect the neck to avoid coil protrusion (Fig 2). In this situation, there are several options: 1) Place 1 balloon in the parent vessel and a bifurcation artery. Inflate the balloon sufficiently to completely cover the neck (some balloons are specifically designed for this purpose with a pear shape when inflated). 2) Place two balloons in front of the aneurysm neck. For example, for a basilar tip aneurysm, a balloon is placed in the basilar artery extending into the 1 posterior cerebral artery and another balloon is placed on the other side. 3) Place a balloon parallel to the neck of the aneurysm by navigating through the circle of Willis anastomosis. For example, in a carotid bifurcation aneurysm, the balloon is not navigated through the ipsilateral carotid artery but through the contralateral one and the anterior communicating artery. This technique is feasible if the anastomoses of the circle of Willis are present and sufficiently large. 4) Place a round balloon mounted on a microcatheter in front of the aneurysm neck. These balloon catheters are no longer available; therefore, this technique can no longer be used. 5) Place a double-lumen microcatheter remodeling balloon. It is placed in front of the neck with the microguidewire inside the neck. The coils are deposited in the aneurysm sac through the second lumen. In bifurcation aneurysms, the best option is decided according to the anatomy of the parent vessel (cervical and intracranial portions), the anatomy of the circle of Willis (confirm that posterior communicating and anterior communicating arteries are present), and the aneurysm anatomy (size and position of the neck, direction of the aneurysm sac, and relations between aneurysm neck and bifurcation branches).
Use and Feasibility of the Technique
In 3 small series, the rate of use of the remodeling technique was very heterogeneous: 8.6%,9 16.9%,5 and 33.0%.8 The remodeling technique was more frequently used in unruptured aneurysms (37.3%) than in ruptured aneurysms (20.5%), according to the analyses conducted in the ATENA and CLARITY series.12,13
According to the ATENA and CLARITY analyses,12,13 the remodeling technique was used in all aneurysm locations but less frequently in anterior communicating and anterior cerebral aneurysms. The navigation in the anterior arterial complex was, with the first generations of remodeling balloons, relatively difficult. The profile of the most recent balloons has been improved, and navigation in the anterior complex is now easier.
The feasibility of the remodeling technique has not been widely studied. Cottier et al4 reported a failure rate of 8%. In this series, the 2 causes of failure were the impossibility of placing the balloon in front of the aneurysm neck and rupture of the balloon during the procedure. Balloon navigation can be difficult in the case of tortuosity of the cervical or intracranial vessels or acute angle of the parent vessel. Another cause of failure of the remodeling technique is a completely unfavorable dome-to-neck ratio with a very wide neck. In this case, the stabilization of coils into the aneurysm sac can be impossible despite inflation of the balloon in front of the neck.
Complications
The 2 most frequent complications of the endovascular treatment of intracranial aneurysms are thromboembolic events and intraoperative rupture. In some series, no comparison was available regarding the rate of complications in both standard coiling and remodeling.2,4,5
In the Layton et al series,8 the rate of thrombus formation was not significantly different in patients treated with standard coiling compared with the remodeling technique (9% and 14%, respectively). Symptomatic thromboembolic events were also observed in a similar percentage of cases (5% in standard coiling and 7% in remodeling). Similarly, in the Brooks et al series,14 diffusion-weighted-imaging abnormalities were detected in 32% in the coiling group and 24% in the remodeling group. However, in the Sluzewski et al series,9 the rate of thromboembolic events was higher in the remodeling group (9.8%) compared with the coiling group (2.2%). In the Shapiro et al review,10 the rate of thromboembolic events was quite similar in patients treated with coiling (8.1%) and remodeling (8.0%). Symptomatic thromboembolic events were encountered in 4.6% of patients treated with coiling and 4.4% of patients treated with remodeling. Death related to thromboembolic events was reported as 1.2% for patients treated with coiling and 0.4% for patients treated with remodeling. In unruptured aneurysms (ATENA), the rate of thromboembolic events was lower in the remodeling group (5.4% versus 6.2% in coiling group), and the clinical outcome was similar in both groups.11 In ruptured aneurysms (CLARITY), the rate of thromboembolic events was also similar in both groups (12.7% in coiling group and 11.3% in remodeling group).12
The rate of intraoperative rupture was not evaluated as extensively. In the Sluzewski et al series,9 the rate of intraoperative rupture was higher in the remodeling (4.0%) compared with the coiling group (0.8%). In the Shapiro et al review,10 the rate of intraoperative rupture was 3.4% in ruptured aneurysms treated with standard coiling, 1.7% in ruptured aneurysms treated with the remodeling technique, 1.4% in unruptured aneurysms treated with standard coiling, and 1.8% in unruptured aneurysms treated with the remodeling technique. In ruptured aneurysms, the clinical outcome was a symptomatic event or death in 2.7% in the coiling group and 1.7% in the remodeling group. In unruptured aneurysms, clinical outcome was a symptomatic event or death in 0.6% in coiling group and 0.9% in remodeling group.
Similar results were reported in the analyses conducted in the ATENA and CLARITY series. In ATENA (unruptured aneurysms), the rate of intraoperative rupture was 3.2% in the remodeling group and 2.2% in the coiling group.11 Clinical consequences (permanent deficit or death) of the intraoperative rupture were encountered in 0.6% in the coiling group and 1.4% in the remodeling group. In ruptured aneurysms (CLARITY), the rate of intraoperative rupture was exactly the same in both groups (4.4%).12 The overall complication rate was 10.8% for standard coiling of unruptured aneurysms and 11.7% for remodeling of unruptured aneurysms; 17.4% for coiling of ruptured aneurysms and 16.9% for remodeling of ruptured aneurysms.11,12
Clinical Outcome
In the Cottier et al4 and Lefkowitz et al5 series, clinical outcome was favorable in all patients. However, death or dependency was encountered in 14.1% after remodeling and 3.0% after coiling in the Sluzewski et al series.9
In the ATENA series, overall morbidity was 2.2% in the coiling group and 2.3% in the remodeling group, whereas mortality was 0.9% in coiling group and 1.4% in remodeling group.11
In the CLARITY series,12 treatment morbidity was 3.9% in the coiling group and 2.5% in the remodeling group. Treatment mortality was 1.2% in coiling group and 1.3% in remodeling group. Global morbidity and mortality (including consequences of subarachnoid hemorrhage and its complications) were 7.1% and 12.5%, respectively, in the coiling group and 3.8% and 12.5% in the remodeling group.
Anatomic Results
In the Lefkowitz et al series,5 initial anatomic results in patients treated with the remodeling technique were quite good, with 100% occlusion in 83% of patients and 95%–100% occlusion in the remaining 17% of patients. During the period of follow-up (range: 1–26 months; median, 10 months), no patient required further treatment or developed a recurrent aneurysm neck or lumen.
In the series reported by Cottier et al,4 anatomic results after treatment with the remodeling technique were also quite good. Immediate posttreatment results reported total occlusion in 69% of cases, subtotal in 29% of cases, and incomplete in 2% of cases. The initial total occlusions remained stable during the follow-up in 90% of cases, and recanalization was observed in 10% of cases. The initial subtotal occlusions showed no modification in 69% of cases, improved to total occlusion in 15%, and displayed regrowth of the remnant in 15%. Initial incomplete occlusion was unchanged during follow-up. Five aneurysms were retreated by using the remodeling technique. Final results (last follow-up angiogram) reported complete occlusion in 67% of cases, subtotal occlusion in 24% of cases, and incomplete occlusion in 9% of cases.
In both the Lefkowitz et al5 and Cottier et al4 series, anatomic results were good, but no direct comparison with standard coiling was available. Packing attenuation was also not studied.
In the Sluzewski et al series,9 anatomic results were different. Packing attenuation was similar in aneurysms treated by standard coiling (24.1%) and the remodeling technique (22.7%). At 6-month follow-up, incomplete aneurysm occlusion was more frequently observed in aneurysms treated with remodeling (27.7%) than with standard coiling (16.9%). Additional treatment was also more frequently performed in aneurysms treated with remodeling (16.9% versus 9.0% for aneurysms treated with the remodeling and standard coiling techniques, respectively).
The Shapiro et al10 literature review does not confirm the Sluzewski et al9 findings. Both initial and follow-up aneurysm occlusion rates were higher in balloon-assisted cases. The initial occlusion rate was total occlusion in 73% of patients in the remodeling group and 49% of patients in the standard coiling group, subtotal occlusion in 22% in the remodeling group and 39% in the coiling group, and incomplete occlusion in 5% in the remodeling group and 13% in the coiling group. At follow-up, there were similar results: total occlusion in 72% of patients in the remodeling group and 54% of patients in the standard coiling group, subtotal occlusion in 17% in the remodeling group and 34% in the coiling group, and incomplete occlusion in 10% of the remodeling group and 11% of the coiling group.
According to the ATENA and CLARITY series,11,12 results are possibly different in unruptured and ruptured aneurysms. In the ATENA series (unruptured aneurysms), immediate anatomic results reported were complete occlusion in 59.8% of aneurysms in the standard coiling group and 59.8% of aneurysms in the remodeling group, neck remnant in 24.3% in the coiling group and 20.1% in the remodeling group, and aneurysm remnant in 16.0% in the coiling group and 20.1% in the remodeling group.11 In the CLARITY series (ruptured aneurysms), immediate anatomic results were different: complete occlusion in 46.9% of aneurysms in the standard coiling group and 50.0% of aneurysms in the remodeling group, neck remnant in 41.6% in the coiling group and 44.9% in the remodeling group, and aneurysm remnant in 11.5% in the coiling group and 5.1% in the remodeling group.12 Using a 2-point classification, the rate of adequate occlusion was significantly higher in the remodeling group (94.9% compared with 88.5% in coiling group, P = .017). The mean packing attenuation was 36.7% ± 23.2% in the coiling group and 39.3% ± 57.7% in the remodeling group (P = .577). In both the ATENA and CLARITY series, long-term anatomic results are not yet available.
Conclusions
All except 1 publication showed a similar safety profile in the standard coiling and the remodeling techniques. The literature review comparing the anatomic results in aneurysms treated by standard coiling and remodeling shows that immediate and follow-up results are better in the remodeling group.9 These results are partially confirmed in the CLARITY series (ruptured aneurysms), showing that adequate occlusion is significantly more frequent in the remodeling group.12 Despite the fact that aneurysms treated by the remodeling technique are different from aneurysms treated with standard coiling, the safety of both techniques is similar with a higher anatomic efficacy of the remodeling technique. Accordingly, wide use of the remodeling technique can be proposed.
For several years, the remodeling technique has competed with stent-assisted coiling for the treatment of anatomically difficult aneurysms, specifically those with a wide neck. However aneurysm stent placement seems to be associated with a higher mortality compared with coiling with or without remodeling.15 Accordingly, wide use of stents should probably not be recommended.
Indicates open access to non-subscribers at www.ajnr.org
References
- © 2012 by American Journal of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Neqstent coil-assisted flow diverter (NQS) for the treatment of bifurcation aneurysms: the coil-assisted flow diversion safety and performance study (CAFI)
- Endosaccular flow disruption with the Contour Neurovascular System: angiographic and clinical results in a single-center study of 60 unruptured intracranial aneurysms
- Patient and aneurysm factors associated with aneurysm recanalization after coiling
- Efficacy and safety of endovascular therapy versus surgical clipping for patients with unruptured middle cerebral artery bifurcation aneurysms
- Immediate post-operative aneurysm occlusion after endovascular treatment of intracranial aneurysms with coiling or balloon-assisted coiling in a prospective multicenter cohort of 1189 patients: Analysis of Recanalization after Endovascular Treatment of intracranial Aneurysm (ARETA) Study
- Wide neck bifurcation aneurysms: what is the optimal endovascular treatment?
- High frequency optical coherence tomography assessment of homogenous neck coverage by intrasaccular devices predicts successful aneurysm occlusion
- Pipeline embolization device treatment of internal carotid artery terminus aneurysms
- Medina embolization device for the treatment of intracranial aneurysms: 18 months angiographic results
- Treatment of Wide-Neck Intracranial Aneurysms with the Woven EndoBridge Device Associated with Stenting: A Single-Center Experience
- Safety and efficiency of the fifth generation Woven EndoBridge device: technical note
- Balloon remodeling-assisted Woven EndoBridge technique: description and feasibility for complex bifurcation aneurysms
- Aneurysm Characteristics, Study Population, and Endovascular Techniques for the Treatment of Intracranial Aneurysms in a Large, Prospective, Multicenter Cohort: Results of the Analysis of Recanalization after Endovascular Treatment of Intracranial Aneurysm Study
- SAFE study (Safety and efficacy Analysis of FRED Embolic device in aneurysm treatment): 1-year clinical and anatomical results
- Feasibility, complications, morbidity, and mortality results at 6 months for aneurysm treatment with the Flow Re-Direction Endoluminal Device: report of SAFE study
- Angiographic and clinical outcomes of balloon remodeling versus unassisted coil embolization in the ruptured aneurysm cohort of the GEL THE NEC study
- The Barrel stent: new treatment option for stent-assisted coiling of wide-necked bifurcation aneurysms--results of a single-center study
- Delayed enhancing lesions after coil embolization of aneurysms: clinical experience and benchtop analyses
- Comparison of Clinical Outcomes of Intracranial Aneurysms: Procedural Rupture versus Spontaneous Rupture
- Safety and Efficacy of Aneurysm Treatment with the WEB: Results of the WEBCAST 2 Study
- Efficacy and Safety of the Woven EndoBridge (WEB) Device for the Treatment of Intracranial Aneurysms: A Systematic Review and Meta-Analysis
- Are Anatomic Results Influenced by WEB Shape Modification? Analysis in a Prospective, Single-Center Series of 39 Patients with Aneurysms Treated with the WEB
- Single-center experience in the endovascular treatment of wide-necked intracranial aneurysms with a bridging intra-/extra-aneurysm implant (pCONus)
- Republished: Initial experience of coiling cerebral aneurysms using the new Comaneci device
- WEB Treatment of Intracranial Aneurysms: Clinical and Anatomic Results in the French Observatory
- Flow-Diverter Stents for the Treatment of Saccular Middle Cerebral Artery Bifurcation Aneurysms
- Follow-up of intracranial aneurysms treated by flow diverter: comparison of three-dimensional time-of-flight MR angiography (3D-TOF-MRA) and contrast-enhanced MR angiography (CE-MRA) sequences with digital subtraction angiography as the gold standard
- LEO Baby Stent Use following Balloon-Assisted Coiling: Single- and Dual-Stent Technique--Immediate and Midterm Results of 29 Consecutive Patients
- Retrograde access to the posterior inferior cerebellar artery in balloon-assisted coiling of posterior inferior cerebellar artery aneurysms
- Woven EndoBridge Intrasaccular Flow Disrupter for the Treatment of Ruptured and Unruptured Wide-Neck Cerebral Aneurysms: Report of 55 Cases
- Initial experience of coiling cerebral aneurysms using the new Comaneci device
- Balloon remodeling of complex anterior communicating artery aneurysms: technical considerations and complications
- WEB Treatment of Intracranial Aneurysms: Feasibility, Complications, and 1-Month Safety Results with the WEB DL and WEB SL/SLS in the French Observatory
- Endovascular treatment of unruptured wide-necked intracranial aneurysms: comparison of dual microcatheter technique and stent-assisted coil embolization
- Low-profile Visualized Intraluminal Support device (LVIS Jr) as a novel tool in the treatment of wide-necked intracranial aneurysms: initial experience in 32 cases
- Safety and performance of the Penumbra Liberty stent system in a rabbit aneurysm model
- "Y" and "X" Stent-Assisted Coiling of Complex and Wide-Neck Intracranial Bifurcation Aneurysms
- Modified balloon assisted coil embolization for the treatment of intracranial and cervical arterial aneurysms using coaxial dual lumen balloon microcatheters: initial experience
- WEB Intrasaccular Flow Disruptor--Prospective, Multicenter Experience in 83 Patients with 85 Aneurysms
- Enhancing Brain Lesions after Endovascular Treatment of Aneurysms
- Temporary Solitaire Stent-Assisted Coiling: A Technique for the Treatment of Acutely Ruptured Wide-Neck Intracranial Aneurysms
- Coil Occlusion of Wide-Neck Bifurcation Aneurysms Assisted by a Novel Intra- to Extra-Aneurysmatic Neck-Bridging Device (pCONus): Initial Experience
- Endovascular Treatment of 300 Consecutive Middle Cerebral Artery Aneurysms: Clinical and Radiologic Outcomes
- Does Stent-Assisted Coiling Still Have a Place in the Management of Intracranial Aneurysms?
- Stent-Assisted Coiling Versus Balloon Remodeling of Wide-Neck Aneurysms: Comparison of Angiographic Outcomes
- In-hospital outcomes associated with stent-assisted endovascular treatment of unruptured cerebral aneurysms in the USA
- Endovascular Treatment of Intracranial Aneurysms: Current Status
- Trends in device-assisted aneurysm treatment at a single high-volume tertiary care center
- Coil Protection Using Small Helical Coils for Wide-Neck Intracranial Aneurysms: A Novel Approach
- Intraprocedural Aneurysmal Rupture during Coil Embolization of Brain Aneurysms: Role of Balloon-Assisted Coiling
- Y-Configuration Stent Placement (Crossing and Kissing) for Endovascular Treatment of Wide-Neck Cerebral Aneurysms Located at 4 Different Bifurcation Sites
- Intrasaccular Flow-Disruption Treatment of Intracranial Aneurysms: Preliminary Results of a Multicenter Clinical Study
- Flow Diverters at and Beyond the Level of the Circle of Willis for the Treatment of Intracranial Aneurysms