
Abstract
BACKGROUND AND PURPOSE: Surface disruption, either ulceration or fibrous cap rupture, has been identified as a key feature of the unstable atherosclerotic plaque. In this prospective observational study, we sought to determine the characteristics of the carotid lesion that predict the development of new surface disruption.
MATERIALS AND METHODS: One hundred eight asymptomatic individuals with 50%–79% carotid stenosis underwent carotid MR imaging at baseline and at 3 years. Multicontrast imaging criteria were used to determine the presence or absence of calcification, LRNC, intraplaque hemorrhage, and surface disruption. Volume measurements of plaque morphology and the LRNC and calcification, when present, were collected.
RESULTS: At baseline, 21.3% (23/108) of participants were identified with a surface disruption. After 3 years, 9 (10.6%) of the remaining 85 individuals without disruption at baseline developed a new surface disruption during follow-up. Among all baseline variables associated with new surface disruption during regression analysis, the proportion of wall volume occupied by the LRNC (percentage LRNC volume; OR per 5% increase, 2.6; 95% CI, 1.5–4.6) was the strongest classifier (AUC = 0.95) during ROC analysis. New surface disruption was associated with a significant increase in percentage LRNC volume (1.7 ± 2.0% per year, P = .035).
CONCLUSIONS: This prospective investigation of asymptomatic individuals with 50%–79% stenosis provides compelling evidence that LRNC size may govern the risk of future surface disruption. Identification of carotid plaques in danger of developing new surface disruption may prove clinically valuable for preventing the transition from stable to unstable atherosclerotic disease.
Abbreviations
- AUC
- area-under-the-curve
- CI
- confidence interval
- ImQ
- image quality
- IPH
- intraplaque hemorrhage
- JV
- jugular vein
- LRNC
- lipid-rich necrotic core
- OR
- odds ratio
- PD
- proton density
- ROC
- receiver operating characteristics
- T1W
- T1-weighted
- T2W
- T2-weighted
- TOF
- time-of-flight
Surface disruption, defined as the presence of ulceration or fibrous cap rupture, is a key element of the unstable atherosclerotic lesion. The occurrence of microemboli during presurgical monitoring with transcranial Doppler has been correlated with ulceration on histology after carotid endarterectomy.1 Park et al2 reported that 77% of carotid lesions removed from symptomatic patients had an ulceration, which was significantly higher than the prevalence of ulceration in plaques removed from asymptomatic patients with high-grade stenosis. Similarly, fibrous cap rupture has been shown to occur more frequently in symptomatic plaques compared with lesions from asymptomatic arteries within3 and among4 patients. Moreover, prospective data have demonstrated that surface conditions at baseline were predictive of future cerebrovascular events.5 While a strong association between surface disruption and symptomatic neurologic events has become apparent, features that predispose a lesion to the development of surface disruption remain ambiguous. Identification of plaque attributes that are present before the development of surface disruption may afford the opportunity to escalate medical intervention and reduce the risk of developing an unstable lesion.
Carotid MR imaging has enabled the in vivo assessment of both the morphologic6 and compositional characteristics of the carotid artery wall. Via histologic validation, multisequence carotid MR imaging has been proved as able to identify surface disruption and to detect and quantify the LRNC, calcification, and IPH.7–10 Subsequently, multisequence carotid MR imaging has been used for associating plaque features with neurologic events,3–5,11 following the natural history of carotid atherosclerosis,12,13 and for monitoring the response to therapy.14–16
In this study, we sought to determine carotid plaque characteristics that predict the development of a new surface disruption. Accordingly, we designed a prospective study that used carotid MR imaging to evaluate the morphology and features of carotid atherosclerotic disease at baseline and at 3-year follow-up.
Materials and Methods
Study Sample
Individuals with at least 1 carotid artery with 50%–79% stenosis as determined by duplex sonography by using Strandness criteria17 were serially recruited from the diagnostic vascular sonography laboratory at the University of Washington Medical Center and the Veterans Affairs Puget Sound Health Care System. The artery with 50%–79% stenosis was designated as the index artery and was selected for serial imaging by carotid MR imaging. In the case where the right and left carotid arteries had 50%–79% stenosis, the index artery was randomly assigned. Subjects were asymptomatic with respect to their carotid disease on the index side before enrollment. The study sample described herein represents the subset of individuals previously reported by Takaya et al5 who underwent a follow-up carotid MR imaging 3 years after their baseline scan.
At both scanning sessions, participants provided answers to a standardized health questionnaire. At the baseline scanning, subjects had their height, weight, and mean systolic blood pressure from both arms recorded. After the initial MR imaging evaluation, all participants were given a telephone interview every 3 months during the period of observation to assess the development of stroke, transient ischemic attack, or amaurosis fugax consistent with the side of the index artery. Participants who gave a history of a neurologic event on the telephone interview were scheduled for an interval visit and underwent a detailed neurologic examination by the study neurologist and review of hospital records.
The study procedures and consent forms were reviewed and approved by the institutional review board before study initiation. Exclusion criteria were prior carotid endarterectomy on the index carotid artery, prior radiation therapy to the neck, age >80 years at the time of enrollment, or contraindication for MR imaging. Medications were not a criterion for exclusion, and all patients were managed medically by their primary care providers for the duration of the observation period.
MR Imaging Protocol
From July 22, 1999, to January 18, 2007, 120 individuals initially asymptomatic were serially evaluated with carotid MR imaging on a 1.5T scanner (Signa Horizon EchoSpeed, Version 5.8; GE Healthcare, Milwaukee, Wisconsin) by using bilateral 4-element, phased array surface coils (Pathway MRI, Seattle, Washington). A standardized multicontrast protocol18 for carotid MR imaging was used to obtain 2D T1-weighted PD-weighted, and T2-weighted black-blood images and 3D TOF bright-blood angiography. All images were obtained with an FOV of 16 cm, matrix size of 256 × 256, and 2 signal-intensity averages. In-plane acquisition resolution was 0.62 × 0.62 mm. Twelve axial images were acquired with a 2-mm section thickness, for a total longitudinal coverage of 24 mm, centered at the bifurcation of the index artery. After acquisition, all images underwent zero-filled interpolation to an image size of 512 × 512. Total acquisition time for all images was approximately 30 minutes. Of note, the hardware, pulse sequences, and imaging protocol were identical for all subjects during the 3 years between baseline and follow-up scanning.
Image Review
Two reviewers, blinded to the time point and clinical information, matched the axial images of the index artery between time points on the basis of the distance from the bifurcation of the carotid artery. All matched axial locations for the index artery were evaluated for ImQ (4-point scale: 1 = poor, 4 = excellent) and were interpreted by reviewers reaching a consensus opinion. For images with ImQ ≥ 2 at both time points, image analysis software (CASCADE,19 Seattle, Washington) was used to draw the lumen and outer wall boundaries. Lumen volume, wall volume, and total vessel volume (lumen volume + wall volume) were used to calculate percentage wall volume (100% × wall volume / total vessel volume), a measure of plaque burden similar to that proposed by Nissen et al20 during imaging investigations of the coronary arteries. Multicontrast imaging criteria previously validated with histology were used to determine the presence or absence of calcification, LRNC, IPH, and surface disruption (ulceration or fibrous cap rupture).7–10 Volume measurements of the LRNC and calcification, when present, were collected. The proportion of each component (LRNC and calcification) relative to the wall volume was also determined (eg, percentage LRNC volume = LRNC volume / wall volume × 100%). Reproducibility for each morphology and compositional metric have been previously reported (inter-reader,8,9,21,22 interscan14,21,23,24). IPH was treated as a dichotomous variable (present versus absent) due to decreased reproducibility of volume measurements compared with the other metrics.8
Data Analysis
Minimum lumen area was determined by the minimum value across all matched locations for each artery. Summary statistics for each metric are presented as mean ± SD for all arteries included in each analysis. The independent t test was used to compare differences in continuous metrics of plaque morphology and composition at baseline between lesions with and without a surface disruption. The Fisher exact test was used to compare differences in the distribution of dichotomous variables (eg, presence versus absence of IPH) between lesions with and without a surface disruption. Univariate binary logistic regression analysis by using all of the clinical and baseline arterial variables identified in Table 1 was conducted to identify statistically significant predictors of a new surface disruption. An OR and its 95% CI are reported for statistically significant associations. Meaningful multivariate analysis could not be performed due to the small number of new surface disruptions that occurred during the study period. ROC and AUC were used to assess the accuracy of classification for each statistically significant metric from univariate analysis. AUC and its associated 95% CI are reported. Annualized change in continuous metrics was compared with zero by using the 1-sample t test. The independent t test was used to compare differences in annualized change between lesions that developed a surface disruption and lesions without a surface disruption. All calculations were made by using SPSS 12.0 for Windows (SPSS, Chicago, Illinois). Statistical significance was defined as a value of P < .05.
Baseline clinical and arterial data (N = 108)
Results
The mean interval between the baseline and follow-up scanning was 3.0 ± 0.2 years. One hundred eight (90.0%) subjects demonstrated image quality ≥2 at both time points. The demographics and baseline arterial characteristics for the evaluable population (N = 108) are presented in Table 1. The mean longitudinal coverage of the artery that matched between time points was 17.6 ± 3.2 mm.
Surface Disruption at Baseline
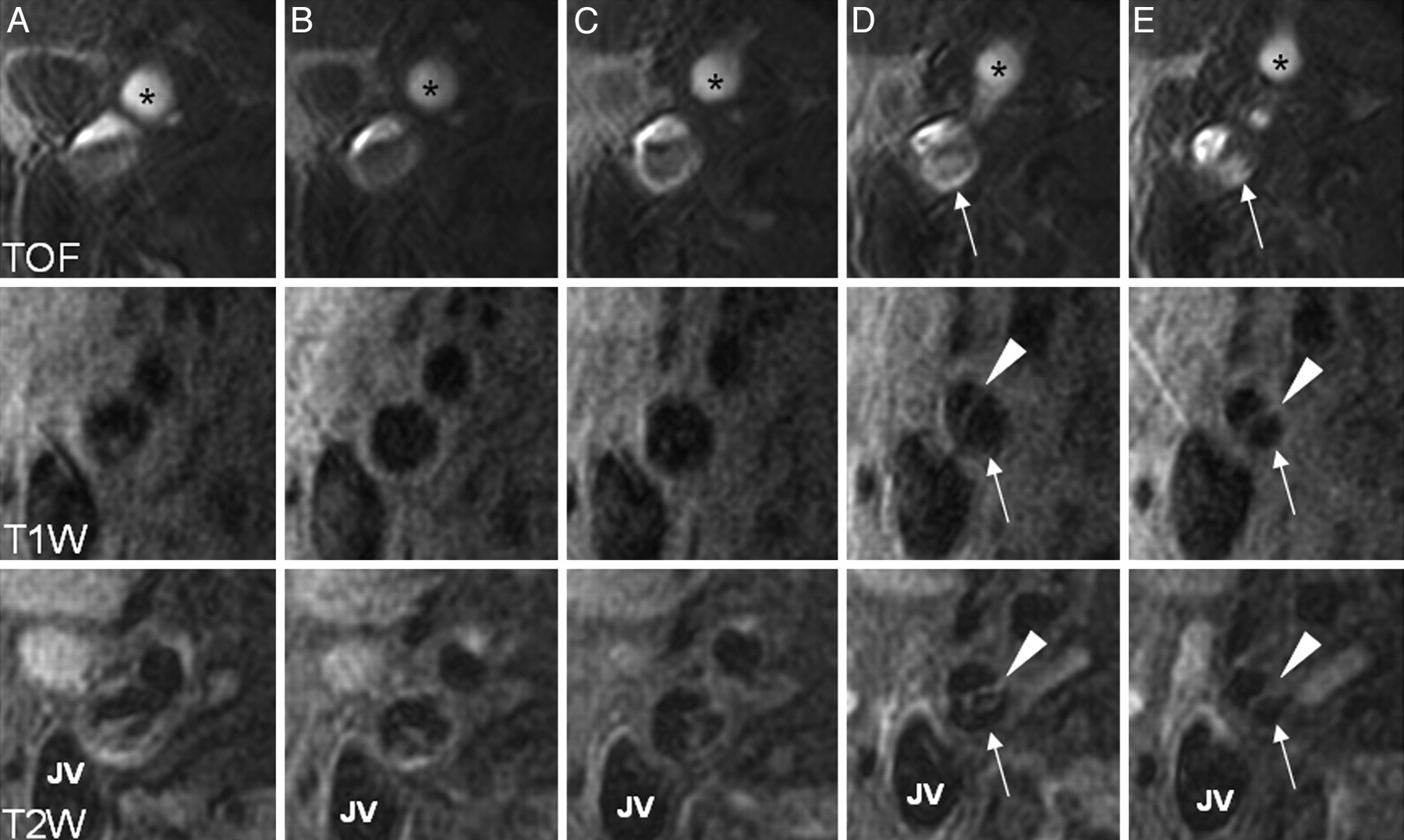
At baseline, 21.3% (23/108) of individuals were identified with a surface disruption. While not all lesions with a surface disruption exhibited an LRNC (Fig 1), compared with the group without surface disruption, a significantly higher prevalence of LRNC (91.3% versus 36.5%, respectively; P < .001) and IPH (87.0% versus 14.1%, respectively; P = .035) was found. The group with surface disruption compared with the group without had a smaller minimal lumen area (13.1 ± 4.9 versus 19.1 ± 10.7 mm2, respectively; P < .001), a larger percentage wall volume (60.6 ± 8.8 versus 51.8 ± 8.2%, respectively; P < .001), a larger percentage LRNC volume (16.1 ± 14.9 versus 3.1 ± 7.1%, respectively; P < .001), and a smaller percentage calcification volume (1.5 ± 2.4 versus 5.4 ± 6.0%, respectively; P < .001).

Multicontrast images from the baseline examination of a 68-year-old man. The axial images are consecutive sections of the right internal carotid artery beginning at the flow divider (column A). There are substantial flow artifacts due to the proximity of the bifurcation. In column D, 2 separate lumens are developing in the internal carotid artery as indicated by 2 levels of intensity on TOF and a band of tissue (arrowheads) separating the true lumen from a penetrating ulcer (arrow). The ulceration extends into the adjacent more distal section (column E). There is no evidence of an LRNC in this artery. Asterisk indicates the lumen of the external carotid artery.
Baseline Plaque Features and New Surface Disruption during Follow-up
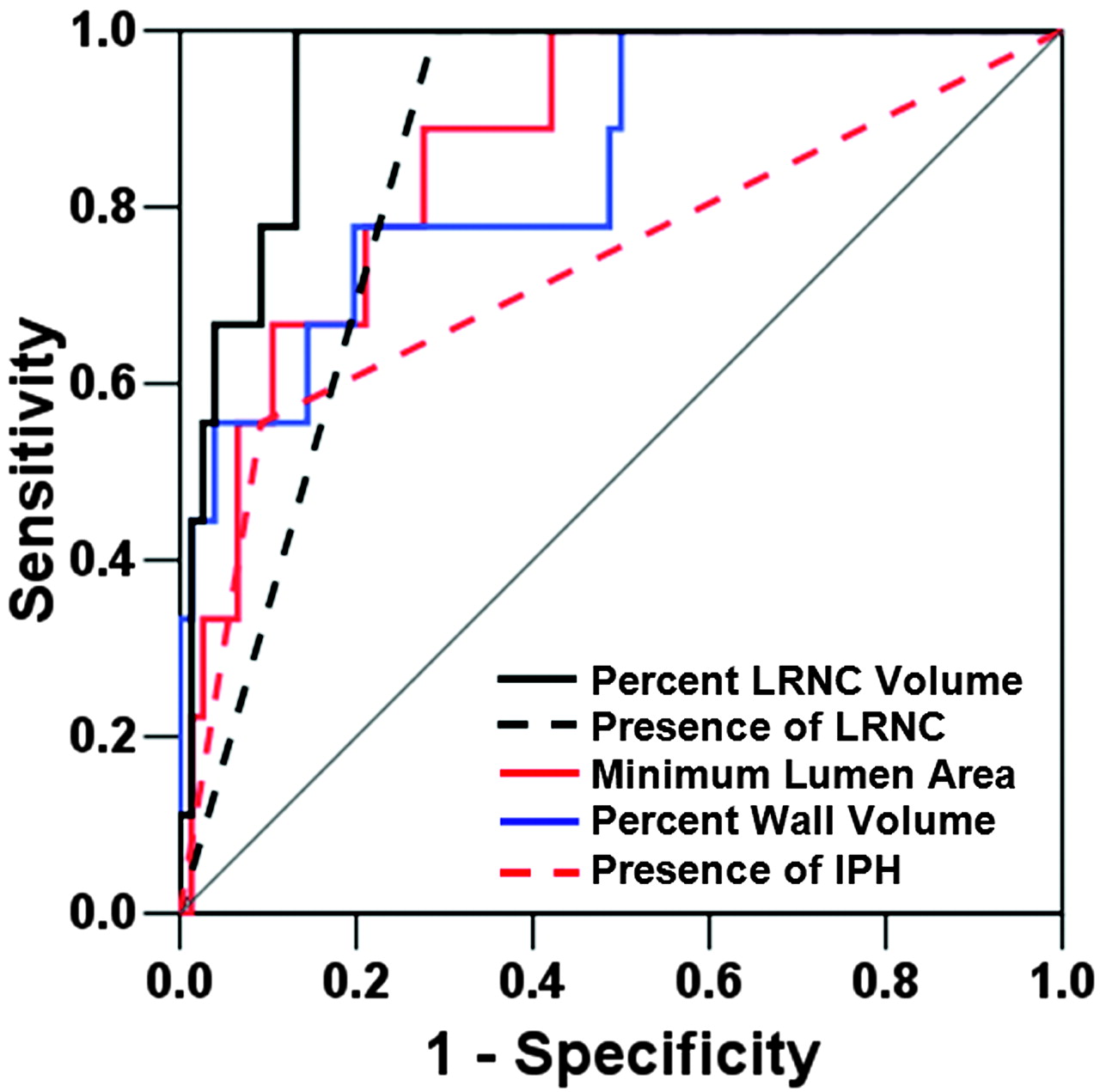
Of the 85 individuals without surface disruption at baseline, 10.6% (9/85) developed a surface disruption at 3 years (Fig 2). Metrics from Table 1 with a statistically significant association with the development of surface disruption during binary logistic univariate analysis are listed in Table 2. Results of ROC analysis and a comparison between lesions with and without new surface disruption for each metric are also provided (Table 2). All lesions that developed a new surface disruption had an LRNC at baseline. The percentage LRNC volume was the strongest classifier for predicting the development of a new surface disruption (AUC = 0.95, Fig 3). Clinical variables (listed in Table 1) were not significantly associated with the occurrence of a surface disruption.
Comparison (n = 85) of baseline features that develop a new surface disruption at follow-up versus lesions whose surface remains intact

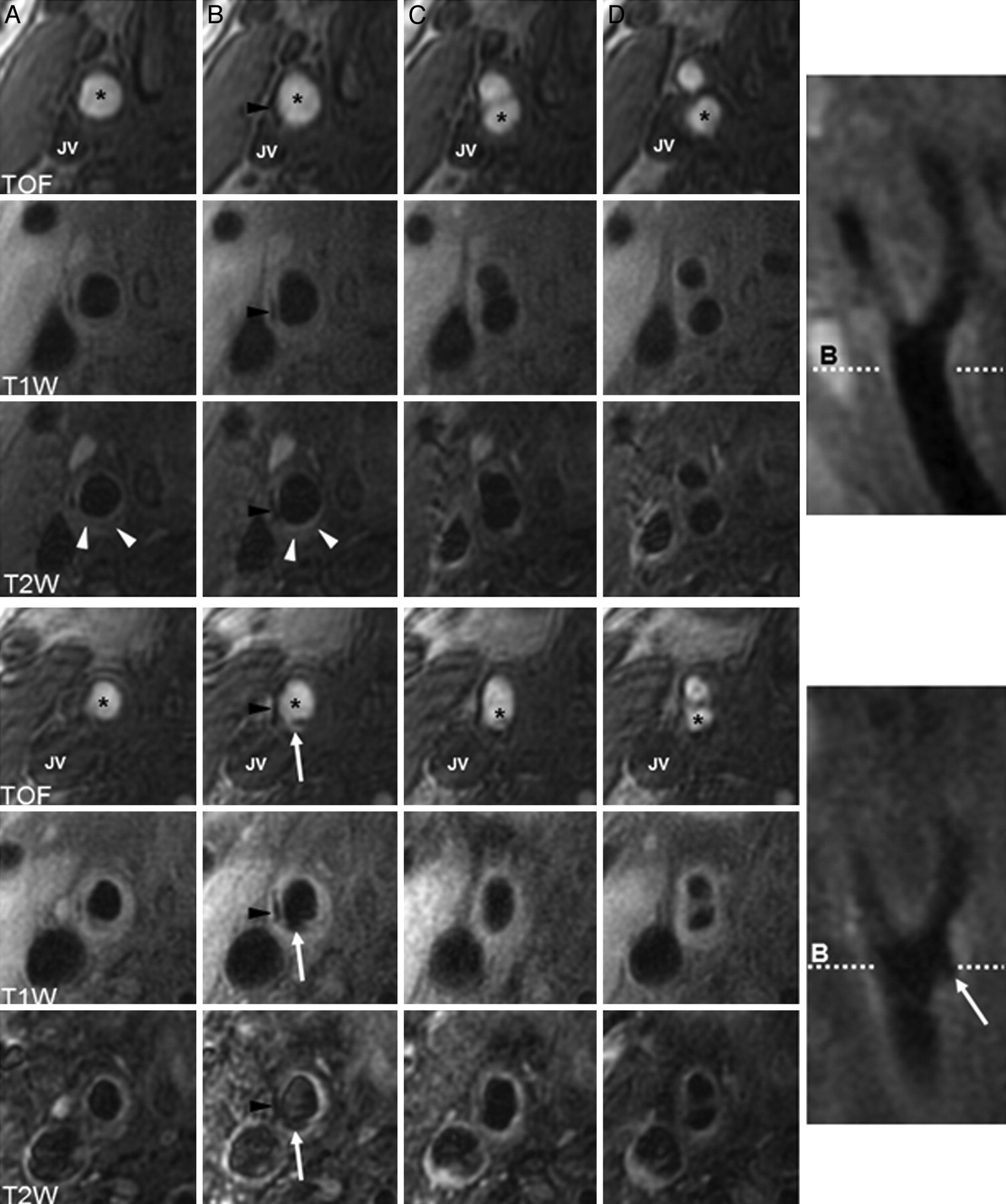
Multicontrast images from the right carotid artery of a 78-year-old man. Baseline images (top panel) demonstrate the presence of a relatively small lesion and minimal lumen narrowing, but a large portion of the arterial wall is occupied by the LRNC. There is an identifiable band of tissue separating the LRNC (white arrowheads, hypointense signal intensity on T2) from the lumen on T2, which is consistent with the presence of a thick fibrous cap. At 3 years (bottom panel), there is an identifiable surface disruption (white arrow) on both axial images and the longitudinal scout image. The dashed line on the longitudinal image represents the imaging location of the axial image in column B. IPH is not present at baseline or at follow-up, but there is visual evidence of an increase in plaque burden and a reduction in lumen area, particularly in column D. The asterisk indicates the lumen of either the common carotid artery or the internal carotid artery; the black arrowhead, calcification.
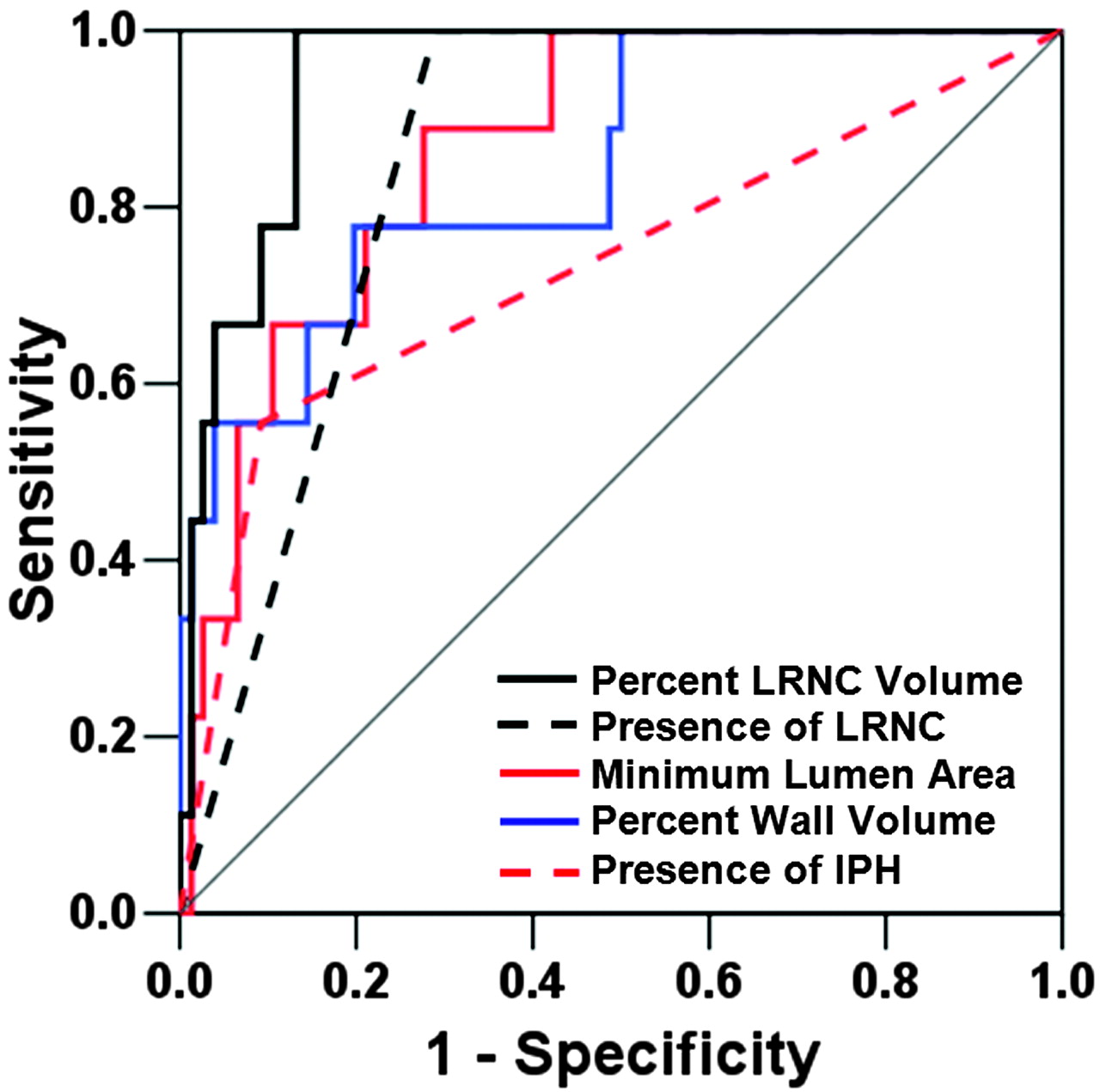
Plots from ROC analysis for development of a new surface disruption.
Plaque Progression and New Surface Disruption
Annualized rates of change in plaque morphology and composition are detailed in Table 3 for lesions that developed a new surface disruption compared with lesions that remained intact during the period of observation. In lesions with a new surface disruption, the percentage LRNC volume increased significantly faster compared with lesions with an intact surface (1.7 ± 2.0% versus 0.1 ± 0.7% per year, respectively; P = .049).
New surface disruption and plaque progression (n = 85)
Cerebrovascular Symptoms
During the 3-year period of observation, 3.7% (4/108) of participants developed cerebrovascular symptoms in the vascular distribution of the index carotid artery. Two subjects developed symptoms coincident with their 3-year follow-up scan. The other 2 subjects developed symptoms before the 3-year follow-up MR imaging: 1 subject elected medical therapy and the other was not a candidate for surgery due to comorbidities. Three of the 4 (75%) symptomatic subjects had an IPH at baseline, and 2 of these 3 (67%) had a fibrous cap rupture at baseline. The fourth symptomatic individual demonstrated imaging evidence of a calcified nodule and had neither an IPH nor a fibrous cap rupture at baseline. Because the study sample was a subgroup of the individuals evaluated by Takaya et al,5 we refer the reader to this previous work for a complete analysis of the association between baseline arterial and clinical features and the development of neurologic symptoms. In the present study, none (0/9) of the individuals who developed a new fibrous cap rupture became symptomatic during the 3-year period of follow-up.
Discussion
In this prospective observational study of asymptomatic individuals with 50%–79% stenosis, we found a striking association between the proportion of the wall occupied by the LRNC at baseline and the development of a new surface disruption. Furthermore, development of a new surface disruption was significantly associated with an increase in the proportion of arterial wall volume occupied by the LRNC. Identification of lesions at risk of developing a new surface disruption may prove clinically valuable for preventing the transition from stable to unstable atherosclerotic disease.
Severity of stenosis has been the traditional imaging criterion for atherosclerotic risk stratification.25 In this investigation, there was a propensity for surface disruption to develop in lesions with a smaller luminal area at baseline. However, minimal luminal area was not the best classifier of surface disruption. This result is consistent with data from the Asymptomatic Carotid Atherosclerosis Study, which evaluated 1662 subjects with >60% stenosis and found that 17 carotid endarterectomies were necessary to prevent a single stroke during 5 years.26 In addition, the European Carotid Surgery Trial reported that 43.8% of the 3018 individuals with symptomatic carotid disease had <30% stenosis on angiography,27 and the North American Symptomatic Carotid Endarterectomy Trial reported that of the 2226 symptomatic subjects with <70% stenosis, 61% had <50% stenosis.28 The limits of stenosis as a predictor of plaque stability are primarily driven by the outward expansion of the arterial wall in response to an increase in plaque burden to preserve luminal dimensions.29 This adaptive arterial remodeling phenomenon has been previously attributed to the poor concordance between luminal stenosis and the severity of plaque burden.30 As such, complementary imaging criteria that evaluate the arterial wall may provide a better assessment of plaque stability.
In the coronary artery, the size of the LRNC has been associated with surface disruption.31 Analysis of carotid endarterectomy specimens have found that plaques with surface ulceration and subintimal hemorrhage contain more cholesterol and less collagen than plaques without these features.32 Evaluation of carotid lesions with sonography has previously demonstrated that the relative risk of cerebrovascular events increased monotonically with the extent of plaque echolucency, a marker of the LRNC.33 Our prospective data indicated that the proportion of the arterial wall occupied by the LRNC was a better classifier of future surface disruption than several known indicators of plaque instability, including IPH and plaque burden. Collectively these findings offer compelling evidence that the metrics associated with the LRNC may provide a better index of plaque vulnerability for new surface disruption than other metrics of lesion morphology and plaque composition.
Two study limitations merit consideration. Although 108 individuals were serially evaluated and monitored during an interval of 3 years, only 3.7% of individuals had clinical events. As such, statistically significant associations were not observed between the occurrence of a new surface disruption and the development of symptoms. Of note, Takaya et al5 have previously reported a stronger association with the prospective development of neurologic symptoms for fibrous cap status and IPH at baseline compared with size of the LRNC at baseline. Accordingly, lesions with IPH and/or surface disruption may pose a greater clinical risk for development of subsequent symptoms than lesions with only a large LRNC. However, the temporal association between the development of surface disruption in lesions with a large LRNC and the subsequent occurrence of embolic events remains ambiguous. Larger long-term prospective studies are necessary to differentiate lesion severity better on the basis of the presence, absence, or combination of high-risk features (eg, IPH, surface disruption, large LRNC) at baseline. Nevertheless, the findings presented herein offer exciting evidence that plaques with a larger LRNC are more susceptible to a future surface disruption.
Second, serial brain MR imaging of all subjects was not performed. In the Cardiovascular Health Study of 3324 asymptomatic individuals, 28% of participants had evidence of silent infarcts on MR imaging at baseline.34 Additionally, there were 1433 participants who underwent 2 MR imaging scannings separated by 5 years and had no infarcts on initial MR imaging. On follow-up MR imaging, 17.7% had ≥1 infarcts; and of these individuals, only 11.4% were symptomatic.35 While not all of the events in these studies34,35 were attributable to carotid disease, these findings indicate that the effects of carotid atherosclerotic disease, including surface disruption, would be better understood if future studies evaluate silent ischemia.
Conclusions
The proportion of wall volume occupied by the LRNC was the strongest classifier for predicting a new surface disruption. Furthermore, carotid plaques that developed new surface disruption demonstrated more rapid progression in percentage LRNC. These initial findings demonstrate the value of high-resolution carotid MR imaging in prospective studies investigating the mechanisms of plaque progression and form the basis for larger studies on the relationship between predictors of plaque disruption, its role in the etiology of future ischemic events, and the efficacy of aggressive preventative medical therapy.
Footnotes
This work was supported by grants from the National Institutes of Health (R01-HL073401, RO1 HL 67406, P01-HL072262, and T32-HL07838).
Indicates open access to non-subscribers at www.ajnr.org
References
- Received May 28, 2009.
- Accepted after revision July 14, 2009.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Characteristics of intracranial plaque in patients with non-cardioembolic stroke and intracranial large vessel occlusion
- Roadmap Consensus on Carotid Artery Plaque Imaging and Impact on Therapy Strategies and Guidelines: An International, Multispecialty, Expert Review and Position Statement
- Plaque Composition as a Predictor of Plaque Ulceration in Carotid Artery Atherosclerosis: The Plaque At RISK Study
- Change in Carotid Plaque Components: A 4-Year Follow-Up Study With Serial MR Imaging
- Carotid Plaque Lipid Content and Fibrous Cap Status Predict Systemic CV Outcomes: The MRI Substudy in AIM-HIGH
- Intraplaque Hemorrhage and the Plaque Surface in Carotid Atherosclerosis: The Plaque At RISK Study (PARISK)
- Nonpharmacological Lipoprotein Apheresis Reduces Arterial Inflammation in Familial Hypercholesterolemia
- Intravascular Frequency-Domain Optical Coherence Tomography Assessment of Carotid Artery Disease in Symptomatic and Asymptomatic Patients
- Arterial Stiffness Is Associated With Carotid Intraplaque Hemorrhage in the General Population: The Rotterdam Study
- Prediction of High-Risk Plaque Development and Plaque Progression With the Carotid Atherosclerosis Score
- Blood Pressure Parameters and Carotid Intraplaque Hemorrhage as Measured by Magnetic Resonance Imaging: The Rotterdam Study
- Intravascular Frequency-Domain Optical Coherence Tomography Assessment of Atherosclerosis and Stent-Vessel Interactions in Human Carotid Arteries
- Carotid Atherosclerotic Plaque Progression and Change in Plaque Composition Over Time: A 5-Year Follow-Up Study Using Serial CT Angiography
- Comparison of Carotid Atherosclerotic Plaque Characteristics by High-Resolution Black-Blood MR Imaging between Patients with First-Time and Recurrent Acute Ischemic Stroke
- Sustained Acceleration in Carotid Atherosclerotic Plaque Progression With Intraplaque Hemorrhage: A Long-Term Time Course Study
- Discriminating Carotid Atherosclerotic Lesion Severity by Luminal Stenosis and Plaque Burden: A Comparison Utilizing High-Resolution Magnetic Resonance Imaging at 3.0 Tesla
- Association Between Carotid Artery Plaque Ulceration and Plaque Composition Evaluated With Multidetector CT Angiography