
Abstract
BACKGROUND AND PURPOSE: Image-guided selective nerve root block/steroid injection is commonly performed for lumbar radiculopathy. The purpose of this study was to evaluate the clinical/imaging characteristics and injection response of adjacent double-root contributions to unilateral lumbar radiculopathy in a typical interventional spine practice.
MATERIALS AND METHODS: In 132 of 350 patients (37.7%) with unilateral radiculopathy, adjacent double–nerve root block/steroid injection was performed on the basis of preprocedural clinical/imaging characteristics. Clinical presentation (pain pattern, VAS), response to injection, and imaging features of potential root compression/irritation (disk protrusion, subarticular/foraminal stenosis) were tabulated.
RESULTS: Clinically, a subset of patients with both L4+L5 and L5+S1 radiculopathy presented with proximal sciatica only in addition to those with typical L4, L5 or S1 radicular patterns. Preprocedural imaging demonstrated evidence of adjacent double-root abnormality in 56 of 79 (71%) patients without prior surgery (single-level disease, 32; 2-level disease, 24) and in all 53 patients with prior lumbar surgery (scar, 42; separate-level root abnormality, 13). Adjacent double-level replication of the patient's familiar pain was present in 82 of 132 (62%) patients, with single-root replication in 37 (28%) and no response in 13 (10%). Typical sciatica was encountered by injection at L4 (15%–33%), likely reflecting furcal nerve lumbar plexus contribution from L5. Sensations from each injected root usually replicated separate recognizable portions of the patient's radiculopathy, with marked or complete pain improvement reported in most patients.
CONCLUSIONS: Adjacent double-level contributions to lumbar radiculopathy are common, and clinical/imaging clues should be assessed to ensure optimum nerve root block/steroid injection treatment response.
Abbreviations
- Pts
- patients
- VAS
- visual analog scale
- LBP
- low back pain.
Image-guided selective lumbar nerve root block/steroid injection is commonly performed in patients who have lumbar radiculopathy.1–7 The choice of the root to treat is usually based on a pattern of radiating leg pain coupled with imaging identification of nerve root compression or irritation. The nerve root passing the disk space in the spinal canal may become compressed or irritated from disk protrusion or lateral recess encroachment. The nerve root passing through the foramen may become irritated or compressed due to disk and facet disease in the foraminal region or far lateral disk protrusion. In most instances of radiculopathy, a single root is involved and is easily recognized through coupling of the clinical and imaging findings. When an injection is made adjacent to an irritated or inflamed root, the patient's familiar pain and radiculopathy are typically replicated, likely due to additional irritation from the local anesthetic used with the steroid injection.1–4
In a subset of patients, the clinical pattern is more confusing, and double-level contributions to radiculopathy may be present. In general, L5 or S1 radiculopathy is perceived as pain below the knee to the calf, ankle, or foot, while L4, L3, and L2 radiculopathy is perceived as pain projecting to the knee, thigh, or groin. A number of factors can alter the typical radicular pattern, including aberrant (transitional) spine segmentation, furcal nerve contribution (interplexus connection between the lumbar and sacral plexuses), and referred pain.8,9 In addition, conservative management with nonsteroidal anti-inflammatory agents or oral steroids can lead to partial improvement, with the development of a less specific radicular presentation. Indeed, some pain-management physicians advocate routine treatment of the 2 adjacent nerve roots or levels for theses reasons.2
In our practice, a combination of specific and less specific referrals is encountered, with many patients evaluated in consultation for pain management. The purpose of this study was to retrospectively assess the clinical presentation, imaging characteristics, and pain response at treatment in adjacent double-level steroid injections for radicular lumbar pain.
Materials and Methods
Over a 4-year period, unilateral lumbar nerve root block was performed in 350 patients for lumbar radicular pain, with or without a component of low back pain, on the service of 1 of 2 interventional spine neuroradiologists. Single-level injections were performed in 214 patients, and 3-level injections were performed in 4 patients, with adjacent double-root injections performed in 132 patients (37.7%). The injection-visit records of these 132 patients were retrospectively assessed with specific attention paid to presentation, imaging and clinical features on evaluation, and immediate and postprocedure responses to the root injections. Lumbar root injections were also performed for bilateral radiculopathy or in combination with other injection procedures (ie, facet, sacroiliac joint) but are not the focus of this report. Institutional review board approval was obtained for this retrospective study.
In the 132 patients with double-level injections, the 2-level procedure was specifically requested by the referring physician in 47 patients. Adjacent double-root injection was chosen for 85 patients after consultation with the treating physician, on the basis of our examination characteristics of the radicular pain in combination with the imaging appearance suggesting adjacent double-root abnormality on the preprocedural imaging studies. A preprocedural interview was also conducted by the spine nurse in all patients with pain characteristics, and a VAS 0–10 grade level was documented in most patients. The treating physician further performed a focused history and examination in the procedure suite, with specific attention to the characteristics and location of radiating leg pain and assessment of preprocedural imaging available in all patients.
In most cases, preprocedural imaging findings were abnormal and demonstrated evidence of 2-level root abnormality or degenerative disk disease. In general, L5+S1 root injections were performed when imaging suggested L5 and S1 root abnormality, and radiculopathy was either isolated to the proximal sciatic region (buttocks, hip, or posterior thigh) or projected below the knee, involving the calf, lateral shin, ankle, or foot. L4+L5 root injections were performed when imaging suggested L4 and L5 root abnormality and radiculopathy was either isolated to the proximal sciatic region (buttocks, hip, or posterior thigh) or involved the anterior thigh and knee as well as projecting to the calf, ankle, or foot. L3+L4 root injections were performed when imaging suggested 2-level root abnormality and radiculopathy projected to the midanterior thigh or knee; and L2+L3 root injections were performed when imaging suggested 2-level root abnormality and radiculopathy projected to the anterior thigh and groin.
The appropriate adjacent nerve roots in question were considered abnormal or suspicious when the roots were either obviously compressed/displaced/distorted or when lateralizing disk margin abnormality (asymmetric bulge or protrusion) or lateral recess encroachment was present that could be related to nerve compression or irritation.10,11 The roots in question could be compressed either in the lateral aspect of the spinal canal or in the foramen/far-lateral region. Nerve root abnormality was identified in the lateral canal when the root was compressed or displaced by subarticular (paracentral) focal disk protrusion or was compressed/trapped in the lateral recess by a combination of disk disease, facet disease, or ligamentum flavum hypertrophy.10–12 Nerve root abnormality was identified in the foramen/far-lateral region when disk protrusion or a spur caused compression or displacement of the root or a combination of disk and facet disease caused foraminal impingement. For this retrospective study, preprocedural imaging was further analyzed by consensus by 2 experienced neuroradiologists and the results were tabulated.
CT fluoroscopy was used for image guidance in 130 patients, with 2 procedures performed with routine fluoroscopic guidance. Image-guidance choice was primarily based on machine availability, though CT fluoroscopy was generally preferred for the S1 nerve root due to more confident identification of the trajectory to the root through the posterior S1 sacral foramen. While not mandatory, additional advantages of CT and CT fluoroscopy include the ability to obtain complementary preprocedural imaging immediately before treatment and improved identification of the trajectory to the target root in the setting of fusion hardware and adjacent fusion bone mass. When performed with CT fluoroscopy, scout images were obtained through the levels of intended treatment by using an optimal gantry tilt. The trajectory to the posterior aspect of each nerve root was planned with axial levels and the skin entry point marked. When performed with routine fluoroscopy, the location of the target nerve roots was assessed with oblique fluoroscopy targeting the inferior aspect of the pedicle of the intended root. Most procedures were performed by using 9- to 10-cm-long 25-gauge spinal needles, with longer 22-gauge spinal needles used when a greater distance from the skin to the nerve root target was necessary. Local anesthetic (1–2 mL of lidocaine 1% with bicarbonate) was typically used with 22-gauge needles, but it was more variably administered when 25-gauge shorter needles were required.
After targeting the intended nerve, we inserted the spinal needle and brought it adjacent to the root to be injected. When we performed the procedure with CT fluoroscopy, the needle-tip position was confirmed posterior to the target root. When we performed it with routine fluoroscopy, the needle tip position was visually confirmed beneath the pedicle of the intended root by using anteroposterior and lateral fluoroscopy. Assessment for unwanted vascular access was performed by inspection of the needle hub and slight aspiration. Further confirmation of the needle-tip location was obtained with injection of a small volume of nonionic contrast material (CT fluoroscopy: 0.3–.5 mL of iohexol, 180 mg I/mL; routine fluoroscopy: 1 mL of iohexol, 240 mg I/mL; GE Healthcare, Cork, Ireland) to establish an internal wheal adjacent to the root or ganglion when the procedure was performed with CT guidance or by direct visualization of contrast flow to exclude vascular injection when it was performed by fluoroscopy. During injection of the steroid/anesthetic mixture under CT guidance, CT fluoroscopy was intermittently observed to confirm appropriate dilution of the contrast wheal posterior to the nerve root and ganglion. When fluoroscopy was used, a small quantity of contrast agent was added to the steroid/anesthetic mixture and the injection was monitored for potential vascular injection. The 2 treatment needles were typically placed concordantly.
After confirmation of needle-tip location, 40 mg of methylprednisolone comixed with 1.5 mL of bupivicaine 0.25% was injected adjacent to each of the roots targeted for treatment. The patients were actively questioned during injection about whether they sensed local or radiating discomfort with the injection, whether this was their typical radiating pain, and where the provoked pain traveled. Responses were recorded. An attempt was made to determine if the provoked pain radiated to distinctly separate locations or whether the provoked pain overlapped a common distribution. The patient was also asked to grade what percentage, if any, each of the injections contributed to their radiculopathy. Approximately 15 minutes following the injections, the patients were questioned by a dedicated interventional-spine nurse regarding their postprocedure pain level with a VAS pain grade available in most patients.
High Lumbar Injections
Recently, cord infarction has been encountered with injection of an L2 root for high lumbar radiculopathy performed under routine fluoroscopy.13 We routinely use 25-gauge needles, which likely minimize the risk of vascular injury. With this event in mind though, we have recently modified our technique for high lumbar injections with the use of dexamethasone (Decadron) in place of methylprednisolone to avoid the potential for microparticulate embolization into the artery of Adamkiewicz.
Results
The results are summarized in Tables 1⇓–3. Fifty-six of the 132 patients were men, and 76 were women, ranging from 19 to 84 years of age (average, 53.4 years). Adjacent nerve root injections were performed at L5+S1 in 72 patients (54.6%), at L4+L5 in 47 patients (35.6%), at L3+L4 in 11 patients (8.3%), and at L2+L3 in 2 patients (1.5%). In 1 patient ultimately treated at L4+L5, the initial treatment at L3+L4 was ineffective, so it was altered. Transitional spine segmentation at the lumbosacral junction was noted in 17 of 132 patients (13%). Previous lumbar spine surgery was present in 53 patients, (40%), with no prior lumbar surgery in 79 (60%).
Patient's sense of radiating/radicular pain during double-root injection: L4+L5
Patient's sense of radiating/radicular pain during double-root injection: L5+S1
Patient's sense of radiating/radicular pain during double-root injection: L3+L4 and L2+L3
In the 79 patients without prior surgery, imaging features of clinically concordant adjacent double-root abnormality were present at a single lumbar level in 32 patients (coexistent lateral canal and foramen/far-lateral root distortion), with imaging features of concordant double-root abnormalities at separate adjacent lumbar levels involving separate but adjacent roots in 24 patients. In 10 of 79 patients, root abnormality was noted, only associated with a single root; and in 13 patients, degenerative disk disease only was noted without evidence of root compression or disk protrusion. In these patients, double-root treatment was either specifically requested, or clinical and imaging features suggested alternate root contribution to radiculopathy. Both levels were ultimately treated.
In the 53 patients with previous lumbar surgery, clinical symptoms and injected roots were at the prior surgical level in 42 patients and separate from the level of prior surgery in 11. In the 42 patients injected at the surgical level, either simple postoperative changes were noted (epidural/perineural scar) or postoperative change and areas of canal/root distortion from an adjacent degenerative disk or facet disease were present. In the 11 patients injected at a level or levels separate from a prior surgery, typical imaging changes of canal or foraminal/far-lateral root abnormality were present, consistent with the presenting clinical symptoms of double-root disease.
Eleven patients had prior ineffective or only partially effective nerve root block at a single level. Multiple sequential blocks were performed in 21 patients (2 blocks in 16 patients, 3 blocks in 4 patients, and 4 blocks in 1 patient).
L4+L5 Injection
Thirty-two of 47 patients (68%) injected at L4+L5 presented with radicular pain to the knee and/or anterior thigh as well as to the calf or ankle, strongly suggesting radicular contributions from both L4 and L5 (Table 1). In 21 of 32 patients (68%), both roots replicated the patient's radicular pain (Fig 1), with single-root replication in 8 and no provoked pain with injection in 3. In 14 patients with adjacent double-root response, a distinctly different but complementary contribution was clearly recognized by the patient from each root replicating the patient's typical radicular pain, and in 7 patients, the response was perceived as equivalent. In 5 of 32 patients (15.6%), L4 injection provoked typical gluteal, hip, or posterior thigh pain (sciatica) consistent with prominent furcal nerve contribution to the sacral plexus (Fig 2), with 3 of these patients reporting pain projecting to the ankle or foot (Fig 3).

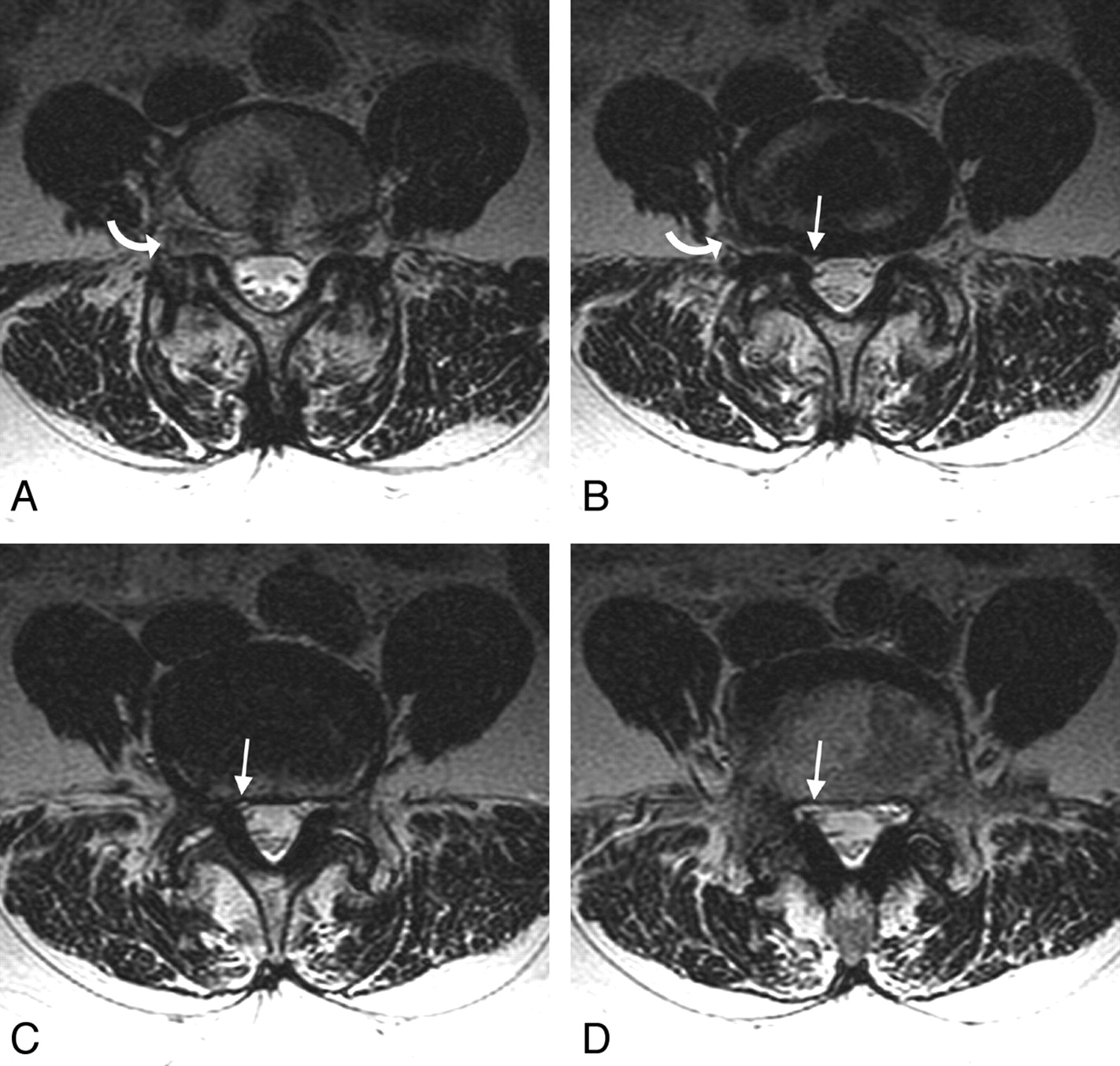
A 69-year-old woman with right-sided radiating leg pain that projected to her posterolateral thigh, knee, calf, and ankle, referred for right-sided nerve root block and steroid administration. Preprocedural MR imaging demonstrated an abnormality at L4–5, with right-sided L4 involvement in the foramen and L5 involvement in the lateral recess. Injection of the L4 root reproduced the patient's thigh and knee pain, and injection of the L5 root reproduced her right calf and ankle pain. She was completely pain-free after the injection. A−C, Axial T2-weighted MR images at L4–5 demonstrate uplifting of the right L4 root in the foramen and far lateral region due to disk (curved arrows), with compression of the L5 root in the lateral recess (arrows). D, At the lowest extent of the lateral recess (arrow), the lateral canal widens and the root reappears in the narrowed niche.
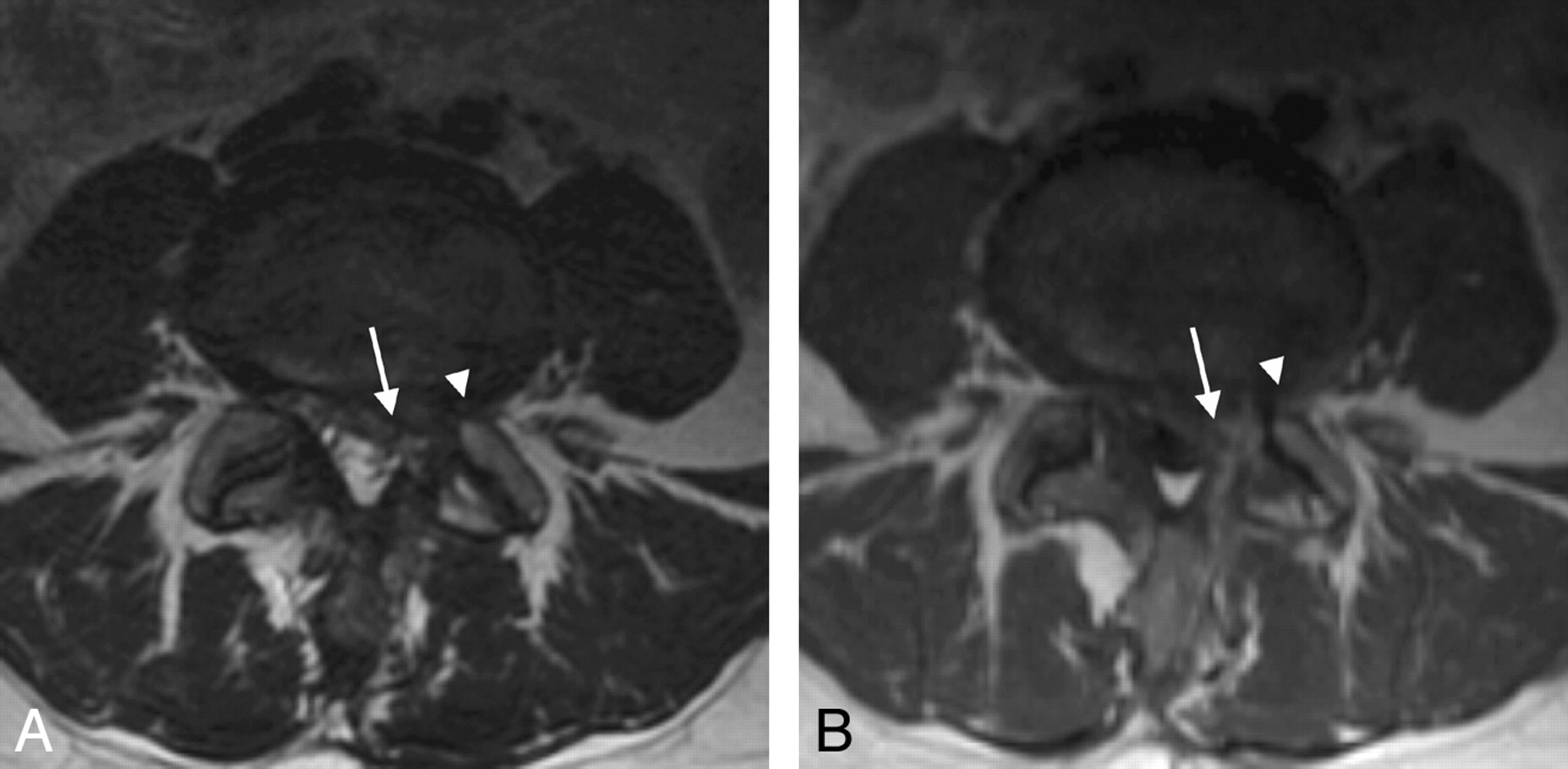
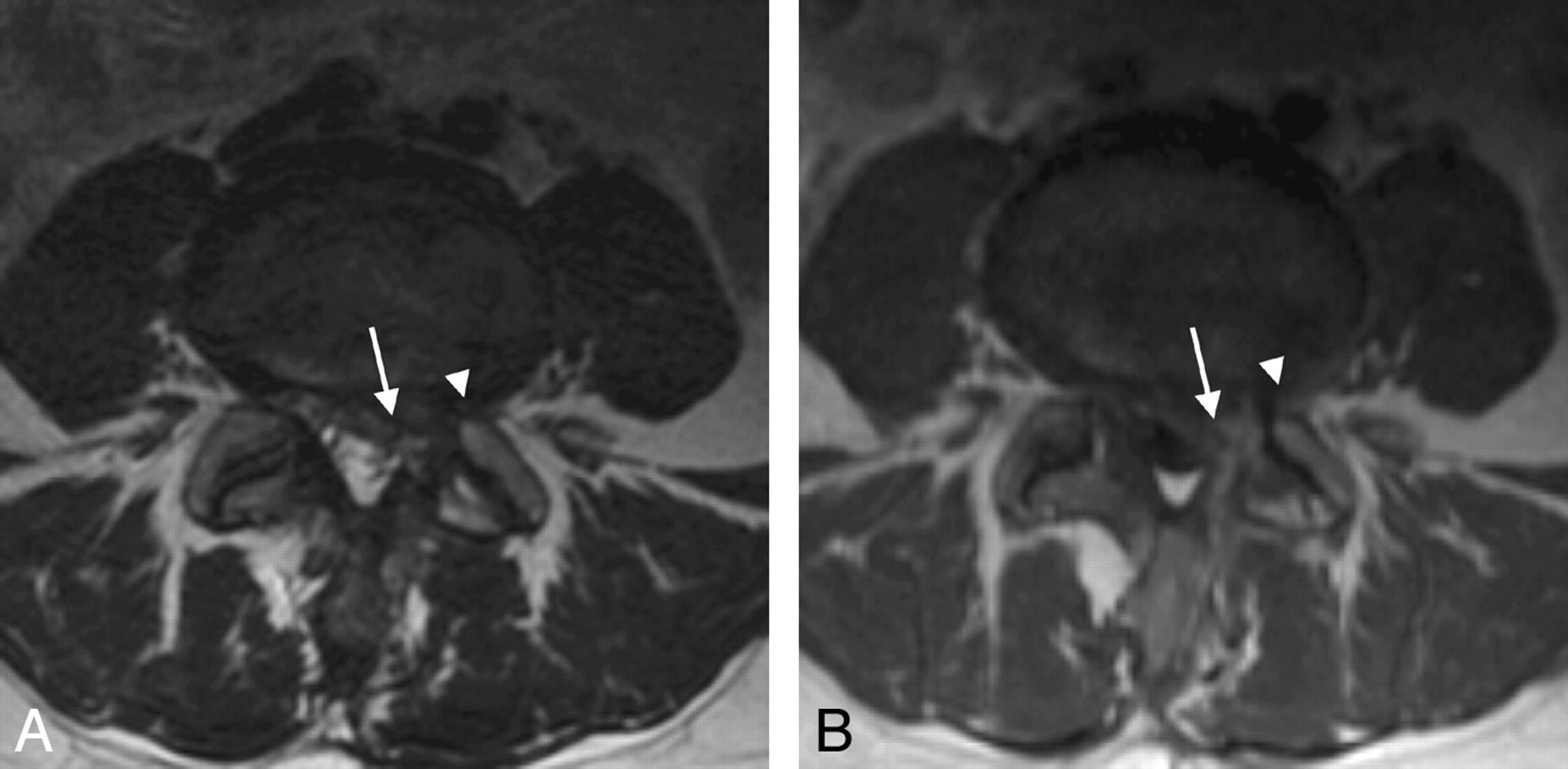
A 46-year-old woman with prior left L4–5 diskectomy 9 months prior, who presented with recurrent left-sided gluteal, posterior thigh, knee, and shin pain and was referred for left-sided nerve root block and steroid administration. Preprocedural MR imaging demonstrated postoperative changes on the left at L4–5, with a scar and root distortion involving the left L4 and L5. Injection of the L4 root reproduced the patient's gluteal and thigh pain, like sciatica, consistent with prominent furcal nerve contribution from L4 to L5. Injection of the L5 root reproduced the patient's shin pain only. She was completely pain-free after the procedure. A, Axial T2-weighted MR image demonstrates postoperative changes on the left, with distortion of the corner of the canal (arrow) affecting the L5 root, and the foraminal region (arrowhead) affecting the left L4. B, Axial T1-weighted image after contrast administration demonstrates a postoperative scar in the canal (arrow) and neural foramen (arrowhead) on the left, involving the L5 and L4 roots.

A 58-year-old man with left-sided leg pain that projected to the thigh, knee, calf, ankle, and foot, referred for nerve root block and steroid administration. Preprocedural MR imaging demonstrated a prominent disk bulge/protrusion at L3–4 and L4–5, suggesting a possible L4 and L5 root involvement. Injection at L4 reproduced the patient's calf and ankle pain, consistent with a significant furcal nerve contribution to L4 from L5, with injection at L5 reproducing a component of the patient's foot and toe pain. A, Axial T2-weighted image at L3–4 demonstrates a prominent asymmetric diffuse disk bulge, with distortion of the left lateral recess (arrow), likely affecting the L4 root. B, Axial T2-weighted image at L4–5 demonstrates a prominent diffuse disk bulge and asymmetric central disk protrusion, with distortion of the left lateral recess (arrow), very likely affecting the left L5 root.
Fifteen of 47 patients (31.9%) presented with proximal sciatica only (gluteal, hip, or posterior thigh pain). In 7 of 15 patients (46%), both roots provoked the patient's typical radicular pain on injection with single-root replication in 5 and no response to injection in 3. In the 7 patients with adjacent double-root response, 5 noted a distinct difference in response between the 2 roots, with each replicating a component of their pain; and in 2 patients, the response was equivalent. In 5 of 15 patients (33%), injection adjacent to L4 was consistent with a significant furcal nerve contribution to the sacral plexus, generating typical gluteal, hip, or posterior thigh sciatic pain; and in 2 of these patients, pain projected to the posterior calf.
Overall in the L4+L5 injection group, 2-root contribution and replication of radiculopathy were present in 28 of 47 patients (60%), with single-root replication in 9 of 47 patients (19%). In the 6 patients without a sense of provoked pain during the injection, presenting pain was completely eliminated at 15 minutes in 5 patients, with partial improvement in 1.
L5+S1 Injection
Twenty-three of 72 patients (32%) treated at L5 and S1 presented clinically with proximal sciatica only (gluteal, hip, or posterior thigh pain), similar to the presentation of patients with L4 and L5 radiculopathy (Table 2). In 3 of these patients, proximal sciatica was accompanied by forefoot or ankle numbness and tingling. Radicular pain was provoked with both injections in 14 of 23 patients (61%), each replicating or contributing to the patient's pain (Fig 4), with a single-root radicular response in 6 and no response to injection in 3 patients. In patients with adjacent double-root response, 6 sensed most of their radicular symptoms from 1 root, with the remainder reporting that either the sensation from the 2 roots was indistinguishable or that each root contributed separately but significantly to the distribution of their radicular pain.

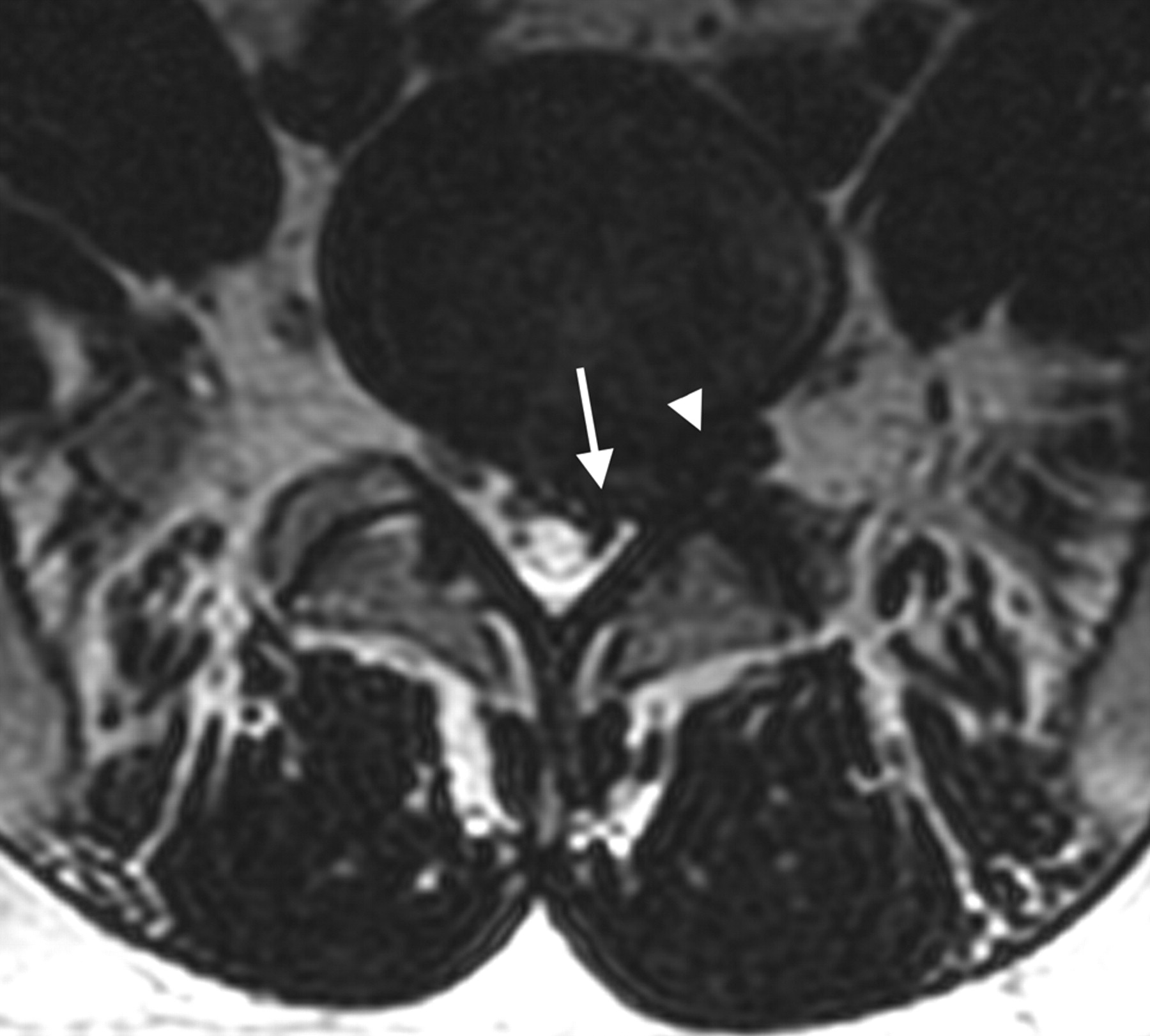
A 35-year-old man with left-sided sciatica radiating down his posterior thigh to the level of the knee, referred for nerve root block and steroid administration. Preprocedural MR imaging demonstrates a moderately large disk protrusion at L5–S1 on the right, with involvement of the S1 root (arrow) in the canal and L5 root (arrowhead) in the neural foramen. Injection of both L5 and S1 reproduced the patient's sciatic pain, with slightly greater pain reproduction from the S1 root.
Forty-nine of 72 patients (68%) presented with radicular pain projecting below the knee to the calf, ankle, or foot (Table 2). In 33 of 49 patients (66%), radicular symptoms were replicated with both injections with single-root replication in 13 and no provoked pain in 3. As in patients with proximal sciatica only, most patients reported either separate but complementary pain provoked from each of the 2 roots, more dominant pain replication from 1 of 2 roots, or indistinguishable radicular discomfort on injection. When a difference between injections was noted, a paradoxical response was often reported, with L5 injection replicating the patient's forefoot discomfort and S1 injection replicating the patient's ankle discomfort. In 1 patient, injection adjacent to L5 provoked anterior thigh discomfort.
Overall in the L5+S1 injection group, a 2-root contribution and replication of radiculopathy were present in 47 of 72 patients (65%), with single-root replication in 19 of 72 patients (26%). In the 6 patients without a sense of provoked pain during the injection, presenting pain was completely eliminated at 15 minutes in 4 patients, with partial improvement in 2.
L3+L4 Injection
Six of 11 patients treated at L3+L4 presented with hip, anterior thigh, and/or knee pain, with additional groin pain reported in 5 patients. The pain was replicated with injection at both levels in 6 patients, with single-injection replication in 5 (Table 3). Complete or near-complete improvement 15 minutes postinjection was reported in 7 patents, with partial improvement in 1 and minor or no improvement in 3.
L2+L3 Injection
LBP and groin pain were the presenting symptoms in both patients treated at L2+L3. In 1 patient, typical pain was reproduced with both injections but no substantial improvement was noted (Table 3). In the other patient, no pain response was noted with the injections but the patient had significant improvement after the procedure.
Injection Response Summary
Double−nerve root replication of the patient's typical radicular pain occurred in 82 of 132 patients (62%) injected at 2 adjacent levels, with single-root replication in 37 (28%) and no radicular replication in 13 (10%). Average VAS before the injections was 5.54, and after the injections, it was 1.36.
Previous Single-Level Injections
In 7 of 11 patients, partial but incomplete improvement was reported after an initial single-level injection, with 4 patients reporting no improvement or only minimal improvement with the initial single-level injection. Follow-up treatment in these patients was adjusted to include adjacent double-root injections. In all 11 patients, the residual pain was provoked with the added adjacent level, and complete or near-complete pain improvement was noted after the procedure. In the 4 patients with no or minimal improvement after an initial single-level injection, double-level injection confirmed the most contribution from the added level, and pain improvement after injection was complete or near-complete. In the 7 patients with initial partial improvement from a single-level injection, a double-level injection confirmed complementary contribution from the added level, with complete or near-complete pain removal after the procedure in 6 of 7 patients.
Multiple Injection Responses
Multiple adjacent double-root blocks were performed in 21 patients. Reduced replication of radicular pain was reported in 1 or both roots in 9 patients, with similar provoked responses noted in 5. In 3 patients, an increase in radicular pain replication was noted on follow-up injections, but all 3 noted complete or near-complete pain relief after the procedure. In 1 patient, both injections replicated their radicular pain but the dominant contributing root fluctuated.
Discussion
Most patients with unilateral lumbar radiculopathy likely have single-level disease. In these instances, coupling of the clinical features and imaging appearance correlates with single-root compression and irritation, and single-level treatment is effective. In a subset of patients, adjacent double-level contributions to radicular pain are present. Understanding the clinical expression of double-root contributions and imaging features of double-root abnormality is important in recognizing this subset of patients. If adjacent double-root contributions are present, single-level treatment will be only partially effective or will be perceived by the patient as inadequate. Given the metabolic effects of the administered steroid, only a limited number of injections can be performed within a fixed time period. In many instances, several injections are required to control radicular pain, making it important to properly recognize patients with dual-level contributions preemptively.
Overall in our selected population, 82 of 132 patients (62%) demonstrated adjacent double-root contributions to radiculopathy, with components of their typical radiating pain replicated during injection of the steroid/anesthetic mixture at each root. Of great importance, in most instances, the patient could clearly recognize the distinctly different but familiar, overlapping, and complementary nature of the replicated pain from each injection, similar to the observations of pain replication with injection in single-level radiculopathy.
The presence of adjacent double-root contributions in our patients was easily perceived clinically with L4+L5 radiculopathy. The presentation of radicular pain both below the knee and above the knee was the most obvious clue, and the patient's replication of pain at both injection locations helped confirm a 2-root contribution, in particular when different and complementary portions of the patient's pain were replicated by each individual injection. Clinical presentation for L5+S1 involvement was more confusing, with either a mixture of calf, ankle, or foot radicular pain or proximal sciatica, only without distal specificity. Indeed, even a subset of patients with L4+L5 pain appears to present with sciatic symptoms, only without clear root specificity. Complementary adjacent double-root contributions could also be recognized in patients with L3+L4 and L2+L3 injections. A number of factors can contribute to the confusing presentations in these patients.
Spine-segmentation irregularities (fused levels, extra levels, rib anomalies, transitional lumbosacral junction) are common and may be present in 20%–25% of the population.14–17 This undoubtedly affects somatome development and ultimately final vascular and nerve root projection to a limb. The anatomic effects are likely compounded caudally and will result in a variation in perceived radicular pain from an individual nerve root. Transitional features at the lumbosacral junction alone are present in approximately 6%–8% of patients.17 In many instances, these make root targeting and treatment decisions unclear or difficult. The presence of anomalous segmentation at the lumbosacral junction certainly influences the accuracy of preprocedural targeting of the roots, contributing to radiculopathy. The high incidence of L5–S1 transitional segmentation present in our patients (13%) in part reflects this challenge to accurate root targeting.
Anatomic variation of the lumbar (L2, L3, L4: femoral and lateral femoral cutaneous nerves) and sacral plexus (L5, S1, S2: sciatic nerve) is well recognized, with branch crossover between the 2 seen in approximately 93% of cadavers.8 In the most common arrangement (50%), a branch from L4 crosses to L5 and travels with the sciatic nerve. Therefore, L4 irritation can produce sciatica, with pain perceived through the sciatic nerve to the calf or ankle. In patients with traditional sciatic presentation, imaging correlation is important to assess potential L4 contribution to the radicular symptoms. Significant L4 contribution to proximal sciatica or calf/ankle radicular pain was found in 10 of 47 of our patients (21%) injected at L4+L5, suggesting a prominent furcal nerve connection to the sciatic plexus in these individuals. Awareness of this anatomic arrangement can be important in patients who present with typical sciatic symptoms but have evidence of L4 root compression or irritation noted on preprocedural imaging.
Conservative management and preprocedural medications (oral steroids or nonsteroidal anti-inflammatory agents) could affect the patient's clinical presentation, making root targeting more difficult. With partial clinical improvement, distal radiculopathy often improves, leaving only proximal sciatic symptoms (buttocks, hip, and posterior thigh pain). Questioning the patient about the initial presentation when symptoms were more severe or recognizing the importance of distal paresthesia (ie, ankle, foot) is often helpful. This might in particular affect recognition of the L4 contribution to distal sciatica.
Axial structures such as the disk, interspinous ligament, facet, and sacroiliac joint can be the source of referred pain that projects down the extremity.9,18,19 Often labeled “Zones of Head,” these referred patterns are less specific and nondermatomal but overlap true radiculopathy. Many patients have multilevel degenerative changes at the disk and facet joint, and back pain is commonly associated with radiculopathy in this patient population. Referred pain from the disk is difficult to exclude, and conservative management could blunt or mask the focal LBP component of axial facet pain. Indeed at some treated levels where radicular pain is not provoked with injection, a positive clinical response with pain elimination might be achieved albeit through a block of the origin of the median branch (dorsal ramus) or treatment of facet referred pain. In 13 of our 132 patients (10%), complete (10 patients) or partial (3 patients) pain improvement occurred after adjacent double-level treatment, despite the absence of radiating pain during injection, suggesting a referred radiating pain source in these individuals.
Recognizing the subtle imaging features of potentially chronically compressed or chronically irritated nerve roots is also critical.18 The root passing by the disk space can be compressed in the canal by subtle disk protrusion, mechanical compression in the corner of canal, or true compression in the lateral recess niche.20 The root exiting the foramen at the disk space can be compressed or irritated at the same level by the disk or facet due to foraminal impingement or foraminal/far-lateral disk protrusion.20 It is also well recognized that regression of an acute disk protrusion can occur,21,22 and while the chronic appearance may become diminutive, initial radicular symptoms may persist or even worsen.22 In addition, biomechanical factors induced by weight-bearing or extension could augment compressive or irritation effects, not perceived at standard lumbar spine imaging.23–25 Degenerative disks often have an asymmetric shape, and recognizing locations of potential root interaction may be crucial in specific patients.
Conclusions
Adjacent double−nerve root contributions to radiating pain were identified in 82 of 132 patients (62%) treated in this selected patient cohort for unilateral lumbar radiculopathy. Presenting clinical symptoms at the time of treatment were often nonspecific, with proximal sciatica only recognized in one-third of patients with both L4+L5 and L5+S1 radiculopathy. Overt or subtle imaging features suggesting double-root involvement, including lateral recess or lateral spinal canal root encroachment, foraminal/far-lateral disk protrusion, or foraminal narrowing, were typically identified and were often essential in clarifying the 2 contributing roots. Factors that might lead to clinical confusion include transitional spine segmentation, furcal nerve contribution to sciatica, referred pain from adjacent structures, and pain improvement with symptom regression after conservative management. Accurate targeting of the levels contributing to radiculopathy is essential to comprehensive patient treatment, and adjacent double-root contributions to radiculopathy could affect the results of treatment-outcome evaluation.
References
- Received May 16, 2009.
- Accepted after revision July 13, 2009.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.