
Abstract
SUMMARY: Assessment of otherwise occult seizure foci arising from the anterior mesial temporal region occasionally necessitates placement of sphenoidal electrodes (SEs). This minimally invasive procedure is often performed without imaging guidance; however, more precise lead positioning with a reduced risk of complications has been described with fluoroscopic guidance. We describe the added value of rotational flat panel CT imaging for precise anatomic localization of the SE tip in relation to the foramen ovale.
Conventional scalp electroencephalogram (EEG) electrode placement alone may be unable to detect basal temporal lobe ictal foci in 5%–10% of patients with temporal lobe epilepsy.1 Therefore, extended EEG monitoring of patients with refractory complex partial epilepsy occasionally necessitates the minimally invasive placement of sphenoidal electrodes (SEs).2–4 Ideal positioning of the electrode tip is slightly anterior and lateral to foramen ovale (FO).3,4 Whether electrodes are placed blindly or under fluoroscopic guidance, submentovertex radiographs are generally obtained to document tip position.
We describe the use of rotational flat panel CT (RFPCT) for precise anatomic depiction of the SE tip position.
Technique and Results
Two consecutive female patients (24 and 43 years of age) with diagnoses of epilepsy undergoing SE placement were the subjects of this report. Each patient underwent SE placement followed by 4 and 8 days' continuous EEG monitoring, respectively. No clinical or technical complications occurred.
After obtaining informed consent and ensuring no history of coagulopathy, we placed each patient on the Axiom Artis biplane fluoroscopy table (Siemens, Erlangen, Germany) in the supine position. A pillow was placed under the shoulders, and the neck was extended as much as could be tolerated comfortably by the patient.
The posteroanterior plane was set in a submentovertex position optimizing visualization of FO. The lateral plane was then set to allow maximal visualization of the needle approach between the mandibular condyle and coronoid process, beneath the zygoma.3 The preauricular skin was then prepped in standard aseptic fashion and a small skin wheal was made by using 2% buffered lidocaine delivered through a 3.5-cm 25-gauge needle. The planned SE entry tract was then also anesthetized with 2% buffered lidocaine to the skull base. Subsequently, the Sphenoidal Electrode Kit (Ad-Tech, Racine, Wis) containing a 40-gauge electrode, composed of 7 strands of 0.001-mm Teflon-insulated (Dupont, Wilmington, Del) stainless steel wire, which was loaded on a 21-gauge 7-cm needle, was advanced under intermittent biplane fluoroscopy until the tip of the needle was brought within approximately 2 mm of the anterolateral aspect of FO. Submentovertex radiography was obtained following needle/electrode insertion. Imaging after removal of the guide needle resulted in very poor visualization of the electrode compared with imaging with the guide needle left in situ (Fig 1).

Submentovertex radiographs obtained after placement of bilateral SEs. The lead alone on the right is not visualized. The guide-needle/electrode system is seen on the patient's left (arrow). Patients often report with scalp electrodes already in place, further complicating optimal visualization of the electrode tip and skull base foramina.
We then performed RFPCT (Syngo Dyna CT imaging; Siemens) to document needle-tip position relative to that expected on the basis of submentovertex radiography. The radiation dose for the RFPCT acquisition was 193.68 μGy (0.36 μGy/image). Please see the Table for RFPCT imaging parameters.5
RFPCT imaging parameters
Postprocessing at the computer workstation, by using Syngo Workplace software (Siemens), allowed data reconstruction in a 512 × 512 matrix with a section thickness of 5 mm. Maximum intensity projection. multiplanar reformatting (MPR), and volume rendering (VR) were then possible.
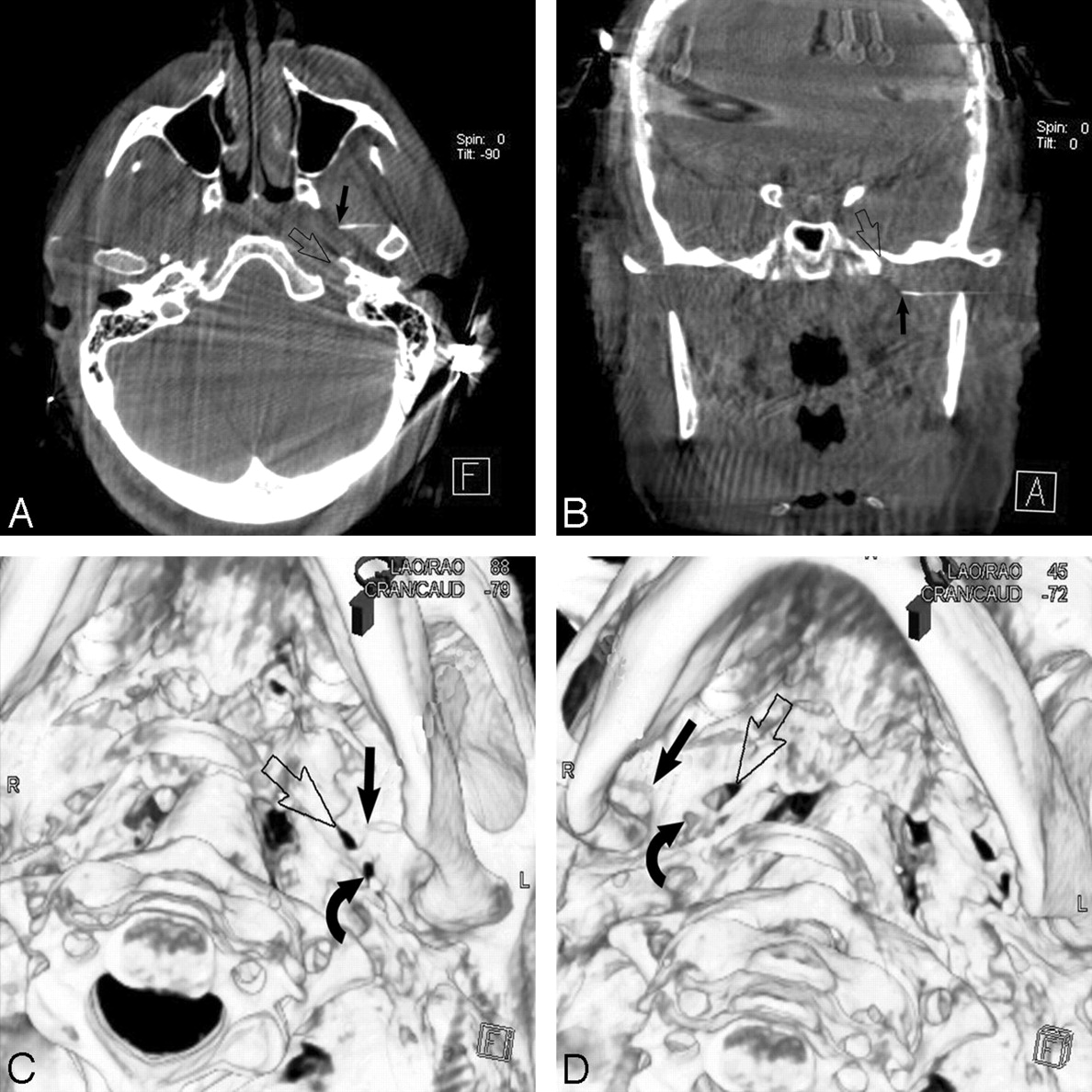
When correlated with RFPCT, needle-tip position was precisely ascertained relative to the skull base with a combination of sagittal and coronal reformations and 3D VR (Fig 2). Coarse adjustments in positioning of the SE delivery system could then be made before needle withdrawal on the basis of the CT acquisition, with confident final SE tip placement radiographically confirmed.
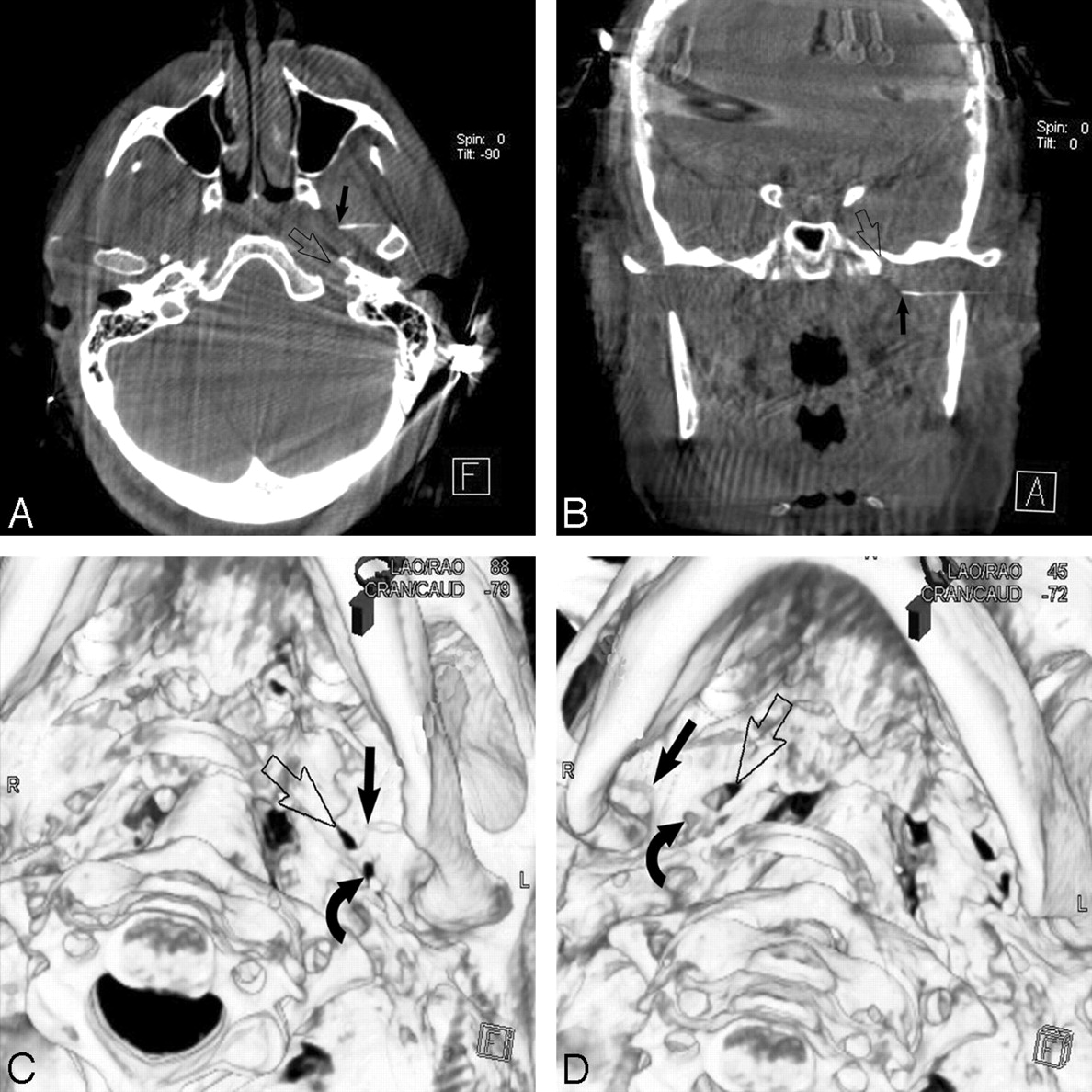
Axial (A) and coronal (B) MPRs and 3D VR (C) RFPCT images precisely depict the relationship of the left SE tip (solid arrow) to FO (open arrow). D, 3D VR RFPCT image shows the right SE tip approximately 14 mm lateral to FO. Repositioning was then performed (not shown). Note foramen spinosum (curved arrows, C and D).
We found that all needles were farther from FO than expected on the basis of submentovertex radiography. When RFPCT was performed before guide-needle withdrawal (2 of 4 needles), coarse adjustments were made to bring the SE tip within approximately 2 mm of the FO. We have also found this technique helpful in the placement of needles in difficult spine interventions such as sacroplasty, wherein the technique affords the opportunity for further needle adjustment before injection of polymethylmethacrylate bone cement.
Once SE tip placement was confirmed, the guide needle was removed with careful attention to pinning the electrode to the patient's skin. The electrode was then carefully coiled and secured to the patient's skin with a sterile dressing, leaving a short tail for manipulation by the EEG technician.
Discussion
The utility of SEs in detecting occult seizure foci within the anterior mesial temporal region is well established.1–4,6–8 At many centers, the placement of SEs is done blindly with tip position documented by postprocedure submentovertex radiographs of the skull.3 Kanner et al4 found the accuracy of blind placement in 6/17 patients (12 electrodes) to range from 4 to 35 mm away from FO on postprocedure radiographs. Although SE placement is generally considered a safe procedure with only minor complications such as minor bleeding, pain, and swelling, there have been reports of transient facial palsy (likely due to infiltration of facial nerve branches with local anesthetic)6 and convulsive syncope (vagally mediated reaction).7 Conscious sedation is generally not necessary.8
Seventeen patients, who initially had nondiagnostic SE placement performed blindly, subsequently underwent fluoroscopy-guided electrode placement, and a seizure focus was then identified in 9/17 patients.4 Imaging guidance also adds safety to the procedure because risk associated with injury to the middle meningeal artery and trigeminal nerve is reduced.3 Wilkus and Thompson9 described the apparently normal superficial migration of electrodes during extended EEG monitoring, likely attributable to normal activities such as chewing and talking. This would suggest that more precise deep localization of the electrodes near FO would allow a longer period during which maximal sensitivity to ictal spiking would exist.
RFPCT-supplemented biplane fluoroscopy has become our standard practice for image-guided SE placement and is a useful adjunct in difficult needle placement during spine interventions such as sacroplasty. The use of RFPCT resulted in dramatically improved visualization of the electrode tip compared with submentovertex radiography and allowed coarse adjustment in electrode placement before guide-needle withdrawal. We acknowledge that these benefits come at an added radiation dose to the patient, with a dose of 193.68 μGy (0.36 μGy/image) for the RFPCT acquisition.
Conclusions
Precise anatomic localization of SE placement can be achieved with RFPCT performed before guide-needle withdrawal. This technique allows further adjustment of lead placement based on the findings of the CT acquisition and permits greater confidence in the 3D orientation of the electrode tip relative to FO. In addition, more precise anatomic placement of the SE may improve the procedural safety and sensitivity of this minimally invasive technique for the detection of otherwise occult seizure foci arising from the anterior mesial temporal region.3,4
Acknowledgments
The authors thank Maxwell Glad, RT(R), for expert assistance with the technical aspects of rotational flat panel CT data manipulation.
References
- Received January 14, 2009.
- Accepted after revision February 6, 2009.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.