
Abstract
BACKGROUND AND PURPOSE: Spontaneous intracranial hypotension (SIH) presents with orthostatic headache, and the diagnosis is made on the basis of low CSF pressure and brain MR imaging findings characteristic of the disorder. However, a broad spectrum of symptoms and MR imaging findings of SIH is recognized, and some cases have no typical MR imaging abnormalities. SIH is believed to be caused by CSF leakage from the spinal dural sac, whereas the usefulness of MR imaging of the spine remains unclear. Our aim was to elucidate the diagnostic value of brain and spinal MR imaging
MATERIALS AND METHODS: The sensitivities for the detection of SIH were retrospectively evaluated in 18 patients with SIH treated in our institutions between January 1998 and August 2007.
RESULTS: Brain MR imaging detected abnormalities in 15 of the 18 patients (83%): diffuse pachymeningeal enhancement in 15 (83%), descent of the cerebellar tonsil in 13 (72%), brain stem sagging in 13 (72%), enlargement of the pituitary gland in 12 (67%), and subdural fluid collection in 13 (72%). Spinal MR imaging detected abnormalities in 17 of the 18 patients (94%): distention of the epidural veins in 14 (78%), epidural fluid collection on fat-saturated T2-weighted images in 16 (89%), and abnormal visualization of the nerve root sleeve in only 1 (6%). The sensitivity for SIH was 83% for brain MR imaging and 94% for spinal MR imaging.
CONCLUSIONS: Spinal MR imaging is useful for the diagnosis of SIH, especially in the early stage.
Spontaneous intracranial hypotension (SIH) is a disease characterized by orthostatic headache and low CSF pressure and is not so rare as previously thought.1,2 The criteria of the International Classification of Headache Disorders3 are widely used to diagnose this type of headache. These criteria require at least 1 of the following to confirm the diagnosis of SIH: low CSF pressure; diffuse pachymeningeal enhancement of brain MR imaging; or evidence of CSF leakage on conventional myelography, CT myelography, or radionuclide cisternography. However, low CSF pressure is not always present in SIH.4 A broad spectrum of neuroimaging features has also been recognized in patients with SIH,2,4–11 in particular diffuse dural enhancement and sagging of the brain on MR imaging1,5,6; and such diagnostic abnormalities are not always detected.12,13
SIH is usually caused by CSF leakage through the spinal dural sac, so spinal MR imaging should demonstrate abnormal findings at a high frequency. However, the International Classification of Headache Disorders does not include the findings of spinal MR imaging. Previous spinal MR imaging studies have suggested that distention of the spinal epidural venous plexus, extradural fluid collection, and abnormal intensity around the root sleeves are specific MR imaging findings indicative of SIH.7,8,14–19 Those studies were based on a relatively small patient series or single cases, so the sensitivity of spinal MR imaging remains unclear.14–19
In the present study, we evaluated the usefulness of spinal MR imaging findings for the diagnosis of SIH in a series of 18 patients.
Materials and Methods
Patients
Eighteen patients (5 men and 13 women) from 24 to 64 years of age (mean, 45 years) with orthostatic headache were treated in our institutions under the diagnoses of SIH between January 1998 and August 2007. Clinical characteristics of the patients are summarized in Table 1. CSF opening pressure in a decubitus position was negative in 10 of the 17 patients (59%) examined, and aspiration was needed to sample the CSF. Normal CSF pressure was present in 5 of 17 patients (29%). Blood pressure was normal in all patients. Symptoms were relieved only by bed rest and intravenous hydration for approximately 1 week in 4 patients, and the other 14 patients underwent autologous epidural blood patch (Table 1). The records of these patients were retrospectively analyzed.
Clinical characteristics of 18 patients with SIH
MR Imaging
Brain axial T1-weighted images (TR/TE, 440/8 ms); axial T2-weighted images (TR/TE = 3000/90 ms); and axial, sagittal, and coronal images with gadolinium were obtained by using a 1.5T MR imaging scanner (GE Healthcare, Milwaukee, Wis) in all patients. Spinal MR imaging used the protocol for T1-weighted images (TR/TE = 400/10 ms), T2-weighted images (TR/TE = 2600/80 ms), and fat-suppressed T2-weighted fast spin-echo images (TR/TE = 3000/70 ms) in all patients. Spinal imaging covered the whole spinal cord in 10 patients, the cervical spine in 2, the cervicothoracic spine in 2, the thoracic spine in 1, the lower thoraco-lumbosacral spine in 1, and the lumbosacral spine in 2. Sagittal fat-saturated T2-weighted imaging was performed in all patients, and axial imaging, in 16. The spinal MR images were reviewed independently by 2 neurosurgeons, and abnormal findings were determined by agreement between the findings.
We considered the findings as positive when diffuse pachymeningeal enhancement was diffusely identified,20 the tip of the cerebellar tonsil was positioned ≥5 mm below the level of the foramen magnum line,21 and the mean height of the pituitary gland was more than 1.5 times that of normal size (4.8 mm for women and 3.5 mm for men).20,22
Results
Findings on Brain MR Imaging
Brain MR imaging showed abnormalities in 15 of the 18 patients (83%): diffuse pachymeningeal enhancement in 15 (83%), descent of the cerebellar tonsil in 13 (72%), brain stem sagging in 13 (72%), enlargement of the pituitary gland in 12 (67%), and subdural fluid collection in 13 (72%). Two of the 3 patients with no abnormalities underwent MR imaging within 2 days of the onset of symptoms (patients 5 and 18).
Findings on Spinal MR Imaging
Spinal MR imaging detected abnormalities in 17 of the 18 patients (94%) (Table 2). Fourteen of the 18 patients (78%) showed distention of the spinal epidural veins, detected as 2 prominent signal-intensity flow voids in the anterolateral epidural space at the upper cervical region, and a consequent collapsed dural sac appearing as a hexagon-like contour in the axial plane (Fig 1A, -B). Irregular signal-intensity flow voids were delineated in the anterior epidural space on the sagittal images, and 2 prominent signal-intensity flow voids were seen in the anterolateral epidural space on axial images at the thoracolumbar region (Fig 2A, -B).
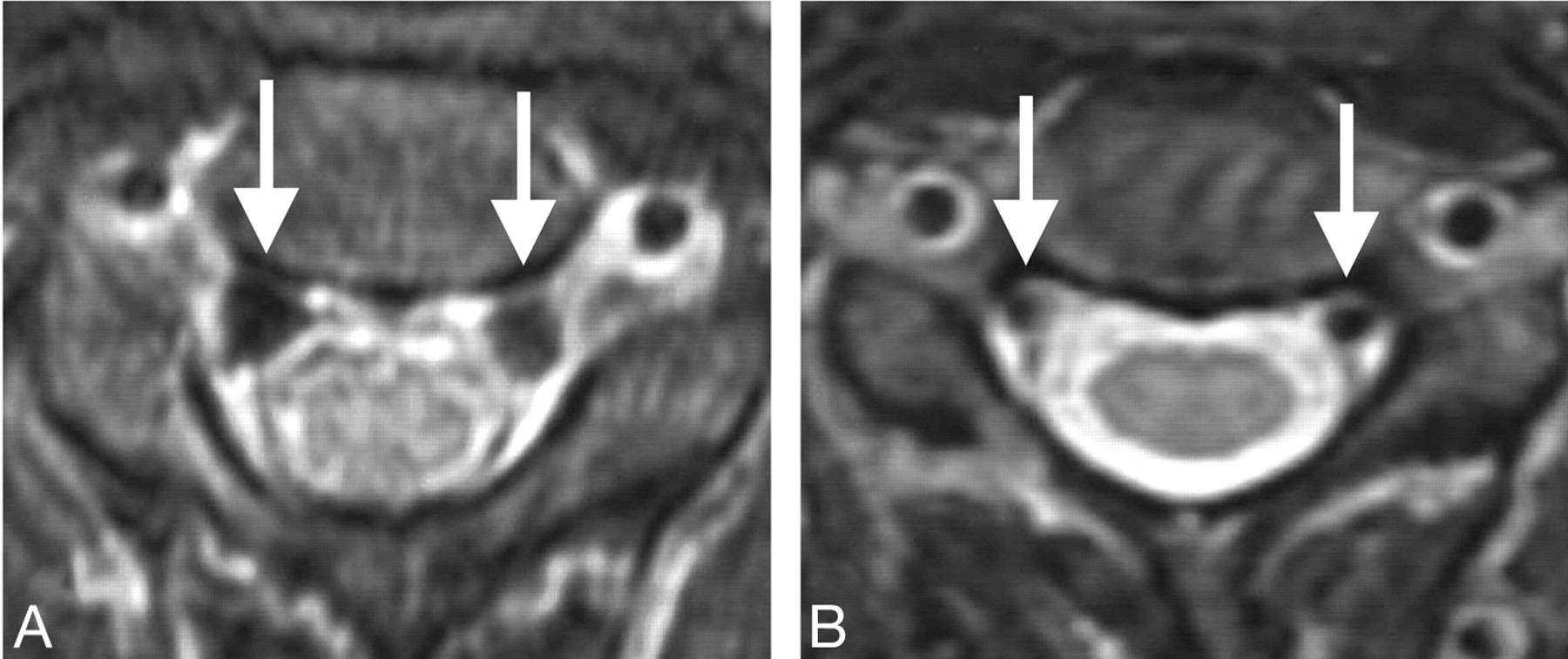
Patient 10 had orthostatic headache. CSF pressure was negative, and brain MR imaging demonstrated diffuse pachymeningeal enhancement, tonsilar herniation, brain stem sagging, and subdural fluid collection. Spinal MR imaging showed distended epidural veins and epidural fluid collection at the cervical spine. The patient was successfully treated with epidural blood patch. A, MR image at the C2 level before treatment shows distention of the epidural veins (arrows). Collapsed dural sac appears as a hexagonal contour. B, Expansion of the dural sac and reduction of the venous size (arrows) are shown after treatment.

Patient 4 presented with orthostatic headache and was diagnosed with SIH. Brain MR imaging demonstrated diffuse pachymeningeal enhancement, tonsillar herniation, sagging of the brain stem, and enlargement of the pituitary gland. Radioisotope cisternography revealed rapid excretion of tracer into the urine and CSF leakage at the lumbar spine. Thoracolumbar spinal MR imaging showed a prominent flow void. Her headache resolved after epidural blood patch treatment. A, Axial MR image shows prominent flow voids (arrows) in the bilateral anterolateral portions of the epidural space at the thoracolumbar region. B, Fat-saturated T2-weighted MR image at the thoracolumbar spine shows winding signal-intensity flow voids of the dilated epidural veins (arrows) behind the vertebral bodies on the parasagittal plane.
Summary of spinal MR imaging
Sixteen of the 18 patients (89%) showed epidural fluid collection on fat-saturated T2-weighted MR imaging. Epidural fluid collection was detected from the cervical through the lumbar spine but was the most prominent in the thoracic area (Fig 3A–C). Epidural fluid collection was mainly located in the anterior epidural space at the cervical region, in the posterior epidural space at the thoracic region, and peripherally at the lumbar region in patients who underwent axial fat-saturated imaging. In addition, 1 of 16 patients (6%) who underwent axial fat-saturated imaging showed fluid collection along the nerve root sleeves and in the paravertebral soft tissue at the thoracic spine (Fig 4A–C).
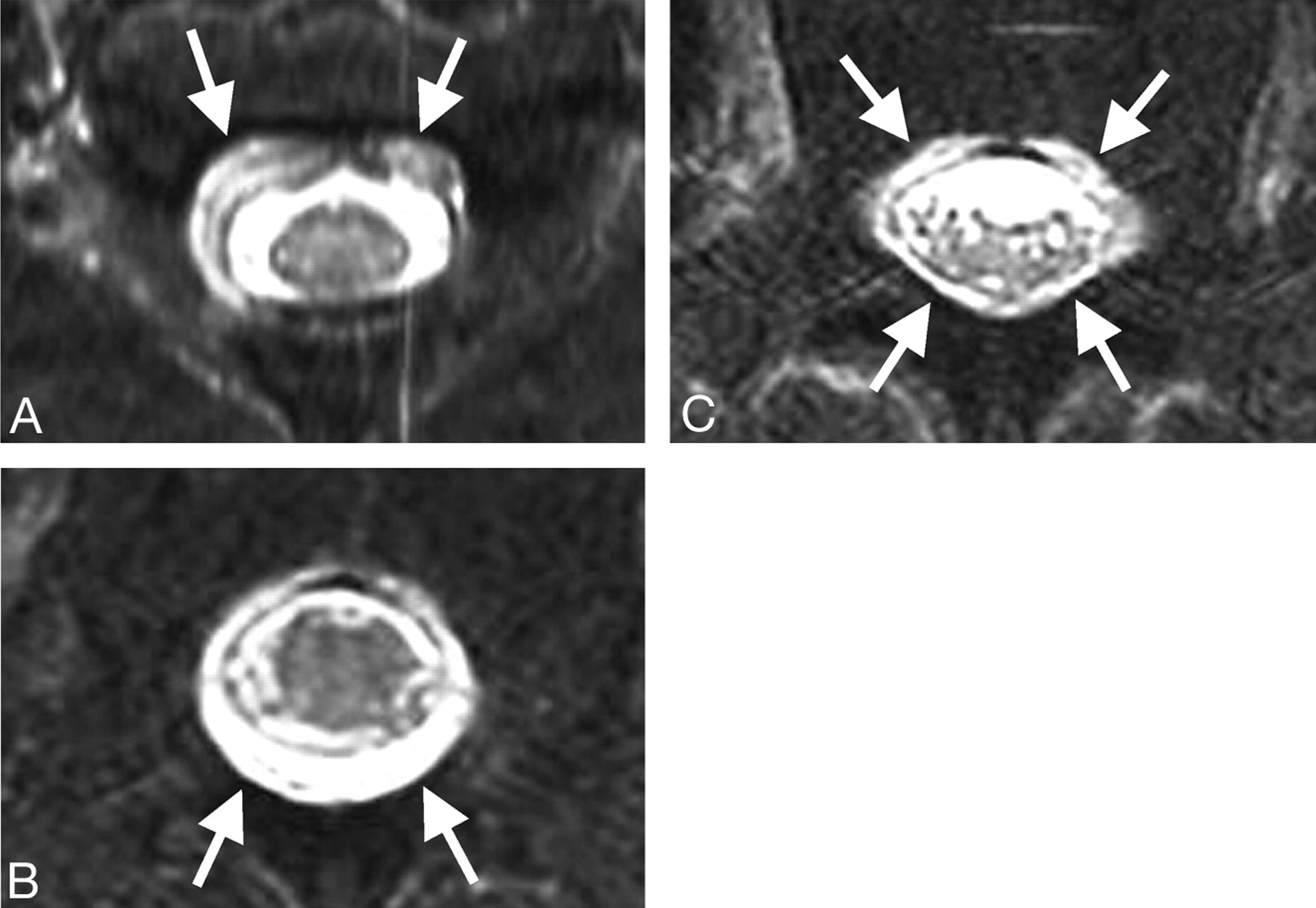
Patient 1 had sudden onset of headache persisting for 1 month and was transferred to our institution with possible diagnosis of subarachnoid hemorrhage. Brain MR imaging revealed typical findings of SIH, including diffuse dural enhancement. Whole-spine MR imaging demonstrated epidural fluid collection. Epidural blood patch was effective, and the symptoms resolved. A–C, Axial fat-saturated T2-weighted MR images show fluid collection before treatment. Fluid collection (arrows) is visualized in the anterior epidural space at the cervical region (A), prominent in the posterior space at the thoracic region (B), and peripherally at the lumbar region (C).

Patient 18 had typical orthostatic headache. CSF pressure was zero. Thoracic spinal MR imaging showed irregular high signal intensity along the nerve root sleeve. He underwent epidural blood patch, and his symptoms completely disappeared. A and B, Axial fat-saturated T2-weighted MR images show irregular high signal intensity (arrows) along the nerve root sleeve at the T1 level. C, Radioisotope cisternogram shows extradural tracer accumulation (arrows) at the high thoracic spine consistent with the MR imaging finding.
Overall, the sensitivity for SIH was 83% for brain MR imaging and 94% for spinal MR imaging.
Discussion
The present study found that the sensitivity for detection of SIH was 83% for brain MR imaging and 94% for spinal MR imaging. In this series, 3 of 18 patients with SIH had no abnormal findings on brain MR imaging, but 2 of these 3 patients showed distended epidural veins and epidural fluid collection on spinal MR imaging. The cause of the discrepancy between brain and spinal MR imaging is obscure but may involve the short interval from the onset to neuroimaging evaluation and/or the small amount of leakage.12,13,18 These 2 patients underwent brain MR imaging within 2 days of the onset of symptoms. In contrast to abnormalities in the cranium, fluid collection in the spinal epidural space is direct evidence of CSF leakage. Therefore, the interpretation of abnormalities on the spinal MR imaging should be more straightforward.
Distended Spinal Epidural Veins
Distended epidural veins were detected in 14 of the 18 patients (78%) in this study, consistent with previous reports of 75%–100% of patients with this finding in a relatively small series with variable diagnostic criteria.7,9,14
A possible explanation of this finding is that decreased intrathecal CSF leads to collapse of the spinal subarachnoid space and results in the enlargement of the epidural space, which is associated with the enlargement of epidural veins and even accumulation of the epidural CSF in the spinal canal. Extended anterior internal vertebral venous plexuses with a convex shape were prominent as signal-intensity flow voids at the cervical region in SIH.17 The collapsed dural sac shows a characteristic hexagon-like contour appearance, which was described as a “festooned appearance.”5,14 This appearance is due to limited collapse of the dura at the tethering points to the posterior longitudinal ligament and to the nerve roots existing through the foramina.14
The anterior and posterior internal vertebral venous plexuses are located in the spinal epidural space.23–25 The anterior internal vertebral venous plexus is located in the anterior spinal epidural space, and epidural fat is usually absent in this area. The size of this venous plexus gradually increases to a maximum at L4 and L5 and rapidly decreases in the sacral canal.25 The posterior venous plexus is absent at the cervical level but is evident at the thoracic level and more voluminous and sinusoidal in the lumbar region.24 On the basis of these anatomic characteristics, distended anterior venous plexus at the high cervical region should be considered as an abnormal finding suggesting SIH.
Contrast-enhanced scanning will provide higher identification for distended epidural veins,16 though we performed a contrast-enhanced study in only a few patients.
In the differential diagnosis, vascular lesions such as arteriovenous (AV) malformation, AV fistulas, varicose veins, or compensated cervical epidural venous enlargement caused by neoplasm or infection should be considered.26,27
Epidural Fluid Collection
Distinguishing extradural fluid collection from fat tissue in the epidural space is difficult on the basis of T2-weighted MR imaging, so fat-saturated imaging is necessary to identify the fluid. In a previous study,14 7 of 8 patients with SIH showed epidural fluid collection on fat-saturated MR imaging, similar to our present results. However, careful observation of not only fat-saturated T2-weighted images but also T2 and T1-weighted images is important.
Anatomic studies indicate that the posterior epidural space is maximum at the midlumbar level and progressively diminishes at higher levels.25 No posterior epidural space is present above the C7-T1 level. In our patients, epidural fluid collection was obvious in the anterior epidural space at the cervical spine and more dominant in the posterior epidural space at the thoracic spine and around the dural sac at the lumbar spine. In addition, the collection was the most prominent at the thoracic spine, probably due to the site of CSF leakage.4 CSF leakage frequently occurs at the thoracic spine.4 The dura mater, which is surrounded by extradural fluid, appears as a hypointense ring, which may be confused with flow-related signal-intensity loss of CSF around the spinal cord on T2-weighted images and may be easily overlooked. The flow-related signal-intensity loss is usually thicker than the hypointense ring of the dura mater and may be interrupted around the thoracic spinal cord.
Abnormalities around the Root Sleeve
In this study, axial fat-saturated imaging showed abnormal root sleeve findings suggestive of fluid collection in 1 of the 16 patients studied. The CSF signal intensity in the paraspinal soft tissue on fat-saturated T2-weighted images is the most diagnostic MR imaging finding.8,16 Our patient 18 showed abnormal CSF intensity in the paraspinal soft tissue at the T2 level, which was compatible with the tracer accumulation site detected by radioisotope myelocisternography. However, the sensitivity of this finding was not high.14,16 The range of imaging, unfamiliarity of observers with the finding, or a noncommittal definition of this finding could also be responsible for the low incidence. Some patients without SIH may harbor a dural pouch, which can be misinterpreted as extradural fluid collection along the nerve roots. Abnormal intensity around the nerve root sleeve may indicate the precise CSF leakage site; however, a false localizing sign at the C1-2 level is also pointed out.28 The low sensitivity of this finding shown in our study suggests less value of this finding for the diagnosis of SIH.
Conclusions
Spinal MR imaging, especially cervical axial imaging and thoracic axial fat-saturated imaging, can lead to an accurate diagnosis of SIH. Spinal MR imaging is recommended to confirm the diagnosis in patients with SIH without abnormalities on brain MR imaging, especially in the early stage.
References
- Received May 26, 2008.
- Accepted after revision July 15, 2008.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Natural history of spontaneous intracranial hypotension: a clinical and imaging study
- Phase Contrast Spine MRI for the Evaluation of CSF Leak, and Why It Matters
- Decubitus CT Myelography for CSF-Venous Fistulas: A Procedural Approach
- Spontaneous Intracranial Hypotension: Atypical Radiologic Appearances, Imaging Mimickers, and Clinical Look-Alikes
- Spine MRI in Spontaneous Intracranial Hypotension for CSF Leak Detection: Nonsuperiority of Intrathecal Gadolinium to Heavily T2-Weighted Fat-Saturated Sequences
- Procedural predictors of epidural blood patch efficacy in spontaneous intracranial hypotension
- Quantitative Measurement of CSF in Patients with Spontaneous Intracranial Hypotension
- A classification system of spontaneous spinal CSF leaks
- Postoperative Intraspinal Subdural Collections after Pediatric Posterior Fossa Tumor Resection: Incidence, Imaging, and Clinical Features
- Sensitivity of MRI of the spine compared with CT myelography in orthostatic headache with CSF leak
- When Should I Do Dynamic CT Myelography? Predicting Fast Spinal CSF Leaks in Patients with Spontaneous Intracranial Hypotension
- Spinal subtraction MRI for diagnosis of epidural leakage in SIH
- MRI with intrathecal gadolinium to detect a CSF leak: a prospective open-label cohort study
- Postpuncture CSF leakage: A potential pitfall of radionuclide cisternography
- MR Imaging of the Optic Nerve Sheath in Patients with Craniospinal Hypotension