
Abstract
BACKGROUND AND PURPOSE: At lumbar diskography, intradiskal lidocaine can eliminate or reduce provoked diskogenic pain. The purpose of this study was to evaluate the postdiskogram CT features of lidocaine-sensitive and lidocaine-insensitive severely painful disks.
MATERIALS AND METHODS: Intradiskal lidocaine was injected at 182 severely painful levels in 111 patients. Clinical records/imaging studies were reviewed for response to intradiskal lidocaine (complete/substantial, partial, and no pain improvement), evidence of diskographic contrast leakage (fluoroscopic/CT images), and the overall postdiskogram CT appearance in these severely painful disks. The assessed traditional Dallas grade (degeneration/radial tear [RT]) was supplemented by identified postdiskogram CT features of annular derangement (annular gap [AG], RT into peripheral annular tear [PAT], isolated PAT, lamellar annular tear, free/attached annular fragments, bucket-handle tear, and peripheral annular pocket).
RESULTS: Isolated degenerative changes (40%) and radial defects with or without degeneration (60%) subsets were noted. Dallas grade 3 degeneration was most commonly observed (69%) with increased features of annular derangement in disks with a worsening Dallas grade. Complete/substantial versus no pain improvement was significantly associated with disk state (diskographic leakage, contained), radial defect (none, RT, or AG), and “RT-into-PAT” and were statistically significant in univariate models (P < .001). The associations remained significant in multivariate models. Higher Dallas degenerative grade and presence of free annular fragments were associated with a greater chance of no pain relief.
CONCLUSION: Severely painful disks demonstrated complex annular derangement with both radial defects (RTs and AGs) or degenerative changes present, alone or in combination. Complete/substantial pain improvement after lidocaine administration is associated with disk state, radial defect (RT and AG), and RT-into-PAT.
There are many potential causes of low back pain (LBP), including the facet joint, intervertebral disk, vertebral body, sacroiliac joint, instability, and muscular spasm.1–4 Diskogenic LBP is difficult to assess and confirm. CT and MR imaging are excellent screening studies that aid in identifying potentially abnormal disks by recognizing degenerative features, shape abnormality, and adjacent marrow reaction. The “high-intensity zone” identified at MR imaging correlates with diskogenic pain, but, in general, imaging findings are nonspecific.5–10 In contrast, provocation lumbar diskography, like physical examination, can help identify the specific disk(s) responsible for LBP by direct disk stimulation.11–14
Injection of local anesthetic into lumbar disks has been reported previously15,16 and reduces pain after disk provocation. A relationship has been identified recently between the extinction of provoked pain after intradiskal lidocaine administration and imaging demonstration of diskographic contrast leakage.17 Potential treatment implications of this response are of current interest in the spine surgical community.18 The purpose of this study was to assess the postdiskogram CT features of lidocaine-sensitive and lidocaine-insensitive painful disks to evaluate for possible anatomic/morphologic features associated with the intradiskal lidocaine pain response.
Materials and Methods
During a 13-month period, 130 consecutive patients had provocation lumbar diskography at our institution by 1 of 2 experienced spine interventional neuroradiologists. Eighty-seven patients were male, and 43 female (average age, 41 years; range, 22–64 years). Patients typically presented with long-standing severe LBP unresponsive to conservative management and were referred by spine-focused orthopedic surgeons or neurosurgeons for preoperative planning. Twenty-eight of 130 patients had previous lumbar surgery.
In 111 of the 130 patients, one or more significantly painful disks were encountered, and intradiskal lidocaine was injected to reduce/eliminate the patient's provoked pain. Nineteen patients were not included (normal diskogram, volume limitation to lidocaine injection, pain only at Cage fused levels, lidocaine not administered, and uninterpretable provocation response).
Provocation diskography was performed at 350 levels in these 111 patients, and at 182 disk levels, severe pain was provoked and intradiskal lidocaine was injected for pain control (concordant, 154 levels; nonconcordant, 28 levels). Unoperated (L5–S1, 64; L4–5, 53; L3–4, 24; L2–3, 6; L1–2, 1; T11–12, 1) and previously operated on levels (L5–S1, 16; L4–5, 17) were both studied. These 182 disk levels form the basis of this report.
Intradiskal lidocaine was not administered at the remaining 168 levels (normal, 126 disks; mild nonconcordant discomfort, 30 disks; volume limitation to lidocaine injection or extensive venous filling on disk contrast injection, 12 disks). Institutional review board approval was obtained for this retrospective study.
Lumbar Diskography Technique
Diskography was performed in a standard fashion as described previously.17,19 Back pain versus leg pain contribution was clarified. The patient's most severe and immediate preprocedure pain level was documented by using the 0–10 Visual Analog Scale (VAS). Limited intravenous sedation (fentanyl, 0.05 mg; Versed, 1 mg [midazolam; Bedford Laboratories, Bedford, Ohio]) was given before the procedure, occasionally supplemented during the study with fentanyl given at the end of the examination. Double needle technique using a 20-gauge guiding spinal needle followed by a long 25-gauge spinal needle accessed the center of the disk space with routine fluoroscopic guidance. All of the needles were placed concordantly opposite the side of leg pain before disk evaluation. The anticipated normal/control disk was studied first.
Disks were provoked by a moderate/rapid hand injection of 1.5–4.5 mL of iohexol (240 mg/cc; GE Medical Products, Milwaukee, Wis) under direct fluoroscopic guidance. Injection volume depended on disk volume end point, clearly established severe pain response, or exaggerated capacity in degenerative disks. Patients were kept unaware of whether a level was being provoked or which level was being studied. Initial injection response was observed by the operator and with a positive pain response, the features of the pain were clarified, VAS level of pain was established, and these items were recorded similar to Walsh et al.19 Concordant pain was recorded if the provoked pain was the patient's typical/familiar pain, and nonconcordant pain was recorded if the provoked pain was not the patient's typical pain. Fluoroscopic spot films were obtained for each disk level in anterior-posterior/lateral projections during and after the injections.
During disk testing, the patient's immediate injection response, response to injection end point (if present), and perception of provoked pain (concordant/nonconcordant) were primarily focused on by the diskographer. Syringe/disk pressures were not recorded during injection.
If a severely painful disk space (typically VAS ≥ 7; concordant/nonconcordant) was encountered, preservative-free lidocaine (2% strength, 1.0–1.5 mL, Xylocaine-MPF; Astra-Zeneca, Wilmington Del) was injected into the disk in an attempt to reduce the patient's provoked pain and to allow response clarity in subsequently studied disks.
The patient was routinely questioned regarding any pain reduction after administration of the intradiskal lidocaine, and the response was recorded as one of the following: 1) complete/near-complete pain relief; 2) partial pain relief; or 3) no significant pain relief or a specific VAS grade reduction from the pain generated by disk provocation relative to baseline pain, depending on the patient's ability to express the change. Responses reported with the VAS were converted to the 3-point scale by calculating the percentage of pain reduction relative to baseline VAS pain level with the following: more than 66% pain reduction indicated complete or near-complete pain relief; 33%–66% pain reduction indicated partial pain relief; and less than 33% pain reduction indicated minimal or no significant pain relief.
Postdiskogram CT (General Electric, Milwaukee, Wis) using bone/soft tissue algorithm with either direct axial 3-mm-section acquisition or spiral technique, 3-mm axial/sagittal reformatting with isotropic voxels was obtained in all of the patients immediately after the diskogram.
Imaging and Lidocaine Response Analysis
Diskogram fluoroscopic images, together with the postdiskogram CT of all of the severely painful lidocaine treated disk spaces, were independently and blindly reviewed by 2 neuroradiologists experienced with lumbar diskography. Identification of epidural diskographic contrast leakage was primarily established by assessment of the fluoroscopic images with secondary inspection and correlation with the postdiskogram CT. Significant leakage at the disk margin around the needle entry site was classified as true leak, but minimal contrast identified at needle entry only after needle withdrawal was not classified as leakage. Disks were judged as either “contained” (no contrast leaking from the disk space) or “leaking” (epidural contrast leakage from the disk space) itemized and tabulated. Discordant judgments were resolved by consensus. Imaging identification of diskographic leakage in the severely painful/treated disks was compared with the response to lidocaine administration: 1) complete/near-complete relief, 2) partial relief, and 3) minimal/no relief.
Postdiskogram CT Feature Analysis
Assessment of the postdiskogram CT features generally followed the characteristics referred to in the Dallas diskogram scale.20 Fundamental observations and subdivisions included the following: 1) radial annular tears, 2) degenerative disk features, and 3) pain response.
The appearance of these disks was typically more complicated than summarized by the Dallas scale.20,21 Diminutive radial tears (grades 1–2) were rarely observed, and wide radial annular defects were commonly encountered beyond simple expansion of a grade 3 radial tear. In addition, the observed degenerative features were typically complex, requiring description beyond the suggested 0- to 3-point grade for accuracy. The Dallas scale was, therefore, supplemented to better reflect the CT observations.
The features identified and used in the modified grading approach are summarized in on-line Table 1 and Figs 1 and 2. “Radial annular defects” (RDs) were commonly seen and described as either “radial annular gaps” (AGs) or “radial annular tears” (RTs). RTs appeared as grade 3 radial annular clefts with opposable edges, 1–8 mm in size. AGs appeared as grade 3 radial annular clefts related to an avulsed or macerated annular fragment. All of the RDs (AGs and RTs) were, therefore, in the substance of the annulus and typically retained a portion of the peripheral annular margin with various thicknesses. Central and lateral RTs were tabulated separately but combined for simplicity of analysis.

Postdiskogram CT features commonly identified in painful degenerative lumbar disks studied at diskography. A, Simple radial annular tear (column 1); radial annular tear with a peripheral annular pocket (column 2); annular gap or wide radial annular tear (column 3). B, Central radial tear into a peripheral annular tear (column 1); combined central and lateral radial tears into peripheral annular tear (column 2); lateral radial tear into a peripheral annular tear (column 3). C, Central radial tear with lamellar annular tears (column 1); combined central and lateral radial tears with lamellar annular tears (column 2); lateral radial tear with lamellar annular tears (column 3). D, Central lamellar annular tears (column 1); combined central and lateral lamellar annular tears (column 2); lateral lamellar annular tears (column 3). E, Central peripheral annular tear (column 1); combined central and lateral peripheral annular tear (column 2); lateral peripheral annular tear (column 3). F, Extensive circumferential lamellar annular tears (column 1); attached annular fragments, loose annular fragments, and bucket-handle annular tear (column 2); extensive free annular fragments with severe macerative annular tears and debris (column 3).

Development of annular gaps. Complex radial annular tears extending into peripheral circumferential annular tears may (A–C) lead to detachment of fragments of the annulus that become free within the central nuclear region (G). Alternatively, peripheral circumferential annular tear (D and E) may become sufficiently detached from the outer annulus with development of a “bucket-handle tear” (F) that subsequently fragments and detaches, coming to lie free within the central nuclear region.
RTs commonly extended into a focal peripheral circumferential annular tear (“RT-into-PAT”), and this feature was noted and analyzed separately. An RT or AG was also identified terminating in a peripheral annular “pocket,” (like knee meniscal cyst) and this feature was analyzed separately.22 Many of these modified features have been considered of significance in relation to diskogenic pain by previous authors.10,21,23,24
The extent of annular degeneration was graded according to traditional Dallas criteria (grade 1, <10%; grade 2, <50%; grade 3, >50%). The features of advanced degenerative annular change noted on postdiskogram CT have been described25 but also resemble findings of knee meniscal degeneration, including the following: 1) peripheral circumferential annular tear; 2) lamellar (onion skin-like) concentric annular tear; 3) bucket-handle tear; 4) attached annular fragments; and 5) free annular fragments/macerated annular debris (AFrags).22 These observations were itemized/tabulated.
Statistical Analysis
Logistic regression models that permit multiple disks per patient were used to obtain odds ratios and corresponding P values associated with testing for association between the postdiskogram CT feature and lidocaine response (total versus no response). Subgroups of statistically significant (P < .05) postdiskogram CT features were analyzed in multivariate logistic regression models relative to lidocaine response (SAS release 9.1; SAS Institute, Cary, NC). All of the multivariate models tested 4 basic postdiskogram CT features, including the following: 1) disk state (leak, contained); 2) radial annular defect state (radial defect [RT, AG]; RT into annular tear; and RD into pocket); 3) basic Dallas degenerative disk grade [grades 0–1, 2, and 3]; and 4) AFrags. Interobserver agreement between the 2 neuroradiologists was assessed using the κ statistic.
Results
Distribution and frequency of the postdiskogram CT features are itemized in on-line Table 1. In 110 (60.4%) of 182 disks, an RD (AG and RT) was present with “degenerative changes only” in 72 disks (39.6%). Two disks appeared normal (1%, one with a Schmorl's node). Degenerative changes were also seen in disks with RDs.
A peripheral circumferential annular tear was identified most frequently (65%) followed by lamellar concentric annular tears (50%) and AFrags (50%). Multiple degenerative features were commonly present simultaneously in an individual disk. Peripheral circumferential annular tears often involved 50%–100% of the peripheral annular margin. Disks that demonstrated “degenerative change only” typically had extensive disease (grade 3). Grade 1 degenerative change was usually present in the setting of RT.
In the 110 disks with RDs, a distinct RT was present in 62 (56%), and AG was present in 48 (44%). Of 62 disks with RT, 42 (68%) tears were central, projecting toward the spinal canal; 18 (29%) were lateral, projecting toward the foramen/far lateral region; and 2 projected anteriorly. RT-into-PAT was present in 37 (60%) of these 62 disks (central, 20 disks; lateral, 16 disks; anterior, 1 disk).
Diskographic contrast leakage was identified in 100 disks, with 82 disks appearing contained. RD (AG and RT) was identified in 79 of 100 leaking disks with “degenerative changes only” in 21. In disks with a simple RT, contrast leakage was identified, extending through the annular margin communication. In disks with RT-into-PAT, a defect in the peripheral annular cleft (tear) was commonly the site of leak into the foramen or spinal canal. In disks with AG, leakage was seen either through the thinned remaining peripheral annular rim or around impacted nuclear/annular debris. In degenerative disks without RD, the leak was near an area of annular thinning.
Of 82 contained disks (without diskographic contrast leakage), 51 (62%) demonstrated degenerative changes only (typically grade 3) with an RD (AG and RT) noted in 31 (38%). These RDs extended to the peripheral annular margin, but the margin remained intact. There was good interobserver agreement between the 2 neuroradiologists for assessed disk features; κ values ranged from 0.75 to 0.92, itemized in on-line Table 2 (legend).
Lidocaine Response
Lidocaine response, as related to postdiskogram CT features, is itemized in on-line Table 3. In 91 disks, complete/substantial pain relief was noted after lidocaine administration (74 with diskographic contrast leakage; 17 contained). Of 74 disks with diskographic contrast leakage and complete/substantial pain relief, 61 (82%) demonstrated an RD (Fig 3), with degenerative change only identified in 13 (typically grade 3). In the 17 contained disks with complete/substantial pain relief, an RD was present in 10 disks, with degenerative changes only in 7.

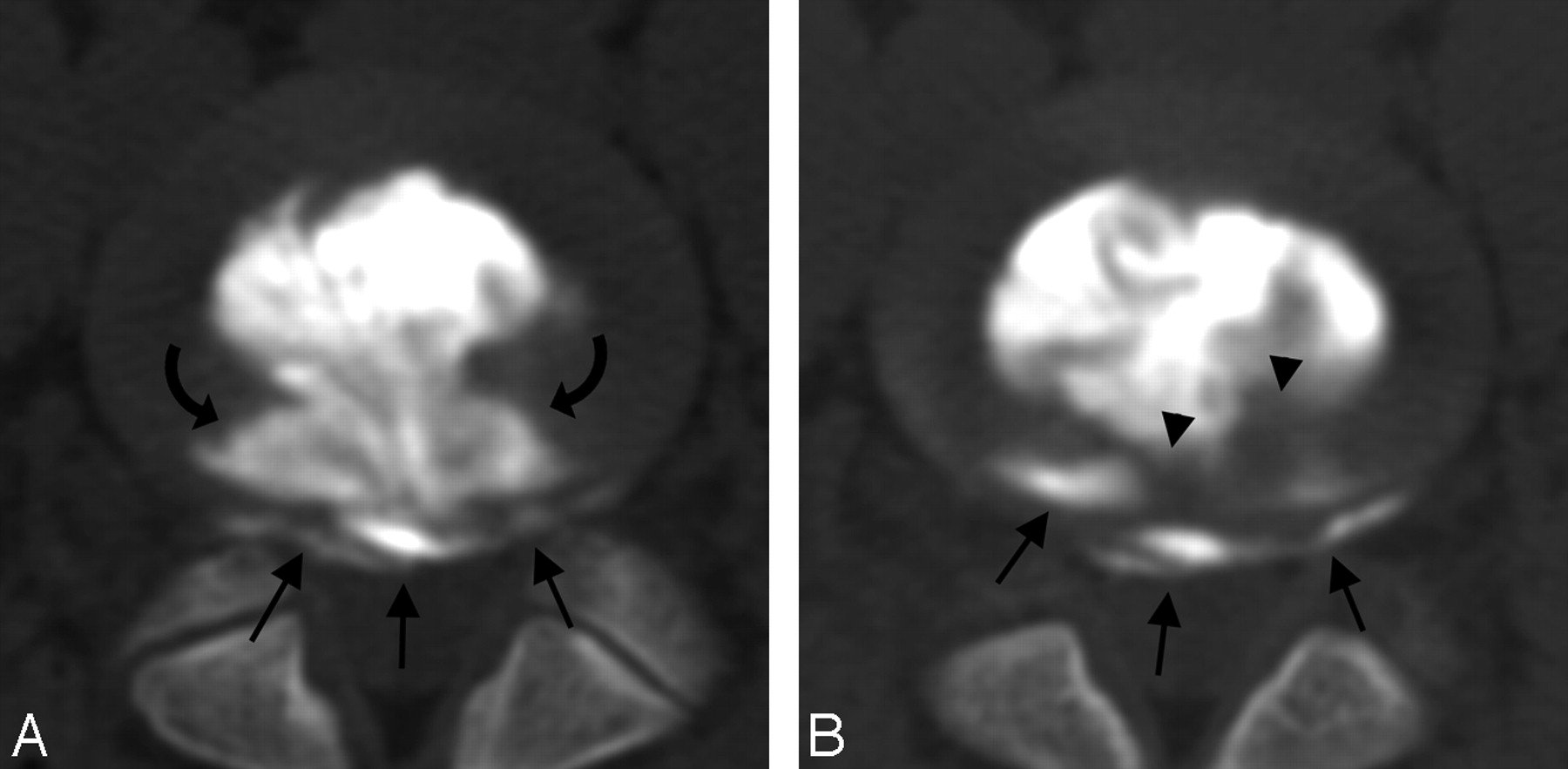
A and B, Patient is a 30-year-old man with a 4-year history of increasing severe LBP with some left leg numbness, which he relates to heavy labor at work but without clear injury incident. MR imaging demonstrated degenerative changes with asymmetric disk bulge at L4–5. Diskographic contrast injection at L4–5 (3 mL) provoked severe and concordant back pain (VAS 7/10). Lidocaine injection into this disk (1.5 mL) resulted in near-complete elimination of the provoked pain. Axial postdiskogram CT demonstrates a wide annular gap (curved arrows) along with a peripheral annular tear (arrows). Also noted are free annular fragments present in the annular gap (arrowheads). Diskographic contrast leakage was noted at the margin of the annular gap (not shown).
In 67 disks, no significant pain relief was noted after lidocaine administration (56 contained; 11 with diskographic contrast leakage). Of 56 contained disks without pain relief after lidocaine, 35 (63%) demonstrated degenerative changes only (Fig 4), with RD noted in 21 (Fig 5). In the 11 disks demonstrating contrast leakage without pain relief after lidocaine, an AG was present in 6 and degenerative changes only in 5.

Patient is a 33-year-old man with a long-standing history of severe LBP that has worsened over the past 3 years. Outside MR imaging demonstrates disk degenerative changes, in particular at L5–S1. Diskographic contrast injection at L5–S1 (2.5 mL) provoked severe and concordant LBP (VAS 10/10). Intradiskal lidocaine injection (1.5 mL) resulted in no improvement in the provoked pain. Axial postdiskogram CT imaging demonstrates circumferential lamellar annular tears (arrows), multiple free annular fragments (arrowheads), and a peripheral annular tear (curved arrow) without diskographic contrast leakage.

A and B, Patient is a 38-year-old man who sustained a service-related injury 16 years ago with progressively increasing severe LBP with some left leg radiation. Outside MR imaging demonstrated significant degenerative disk changes at L3–4. Diskographic contrast injection (3 mL) provoked severe concordant pain (VAS 9/10) at L3–4. Lidocaine injection into the disk (1.5 mL) resulted in no improvement in the provoked pain. Postdiskogram CT imaging demonstrates a central radial tear (curved arrows) and a peripheral annular pocket (arrow), along with loose annular fragments (arrowheads) without diskographic contrast leakage.
Statistical assessment of the identified postdiskogram CT features with respect to the lidocaine response to provoked pain is itemized in on-line Table 2. Disk state was associated with pain improvement after intradiskal lidocaine and remained highly statistically significant (P < .001) in univariate and all of the multivariate models. RD (none, AG, and RT) and RT-into-PAT were also statistically significant with respect to pain improvement with intradiskal lidocaine in univariate analysis and multivariate models.
The presence of AFrags was statistically significant, but the impact appeared inverse, disk-state and morphology related (on-line Tables 2 and 4). Free AFrags were identified most frequently in degenerative change only (37 disks) and AG (25 disks) states, with infrequent identification in RTs (12 disks). In leaking disks, complete pain resolution was noted less frequently in the degenerative change only group, possessing AFrags with no observable change in the AG/RT groups. In contained disks, complete pain resolution was less frequent, with observed AFrags in all of the groups (degenerative changes only, AG, and RT).
Basic degenerative disk grade (Dallas grades 0–1, 2, and 3; inverse reaction to lidocaine) and the presence/absence of a peripheral annular pocket were significant in univariate but not multivariate analysis. The presence/absence of peripheral circumferential annular tear, lamellar (onion skin) concentric annular tears, attached annular fragments, and bucket-handle tear were not statistically significant.
Discussion
The causes of diskogenic LBP are not well understood. More than one factor may be responsible, and multiple factors may contribute in an individual disk, including the following: 1) stretch of the annulus; 2) pressurization of the adjacent vertebral endplate; and 3) leakage of inflammatory irritating debris on epidural structures.12 As seen in provocation lumbar diskography, more than one disk may be painful in an individual patient.17,26
The normal disk is now considered to be innervated peripherally in the outer one third of the annulus by free nerve endings, probably pain fibers, and pressure sensing organelles, probably proprioceptors.1,27–29 In the setting of disk degeneration, pain fiber and neurovascular granulation in-growth have been demonstrated to the inner annulus and even the nucleus.30–32 In the presence of disk degeneration, sensory fiber in-growth may occur, potentially stimulated by the presence of disk space inflammatory debris. In addition, epidural structures, including the dura, epidural vessels, and adjacent ligaments, are richly innervated by pain fibers,33–36 and disk material in the epidural space is known to provoke an inflammatory response.37–42
Our results demonstrate several features related to the significantly painful lumbar disk, including the following: 1) highly complex and overlapping morphology of degenerative changes in currently studied painful lumbar disks on postdiskogram CT; 2) the importance of diskographic contrast leakage is reinforced as a highly significant factor in the intradiskal lidocaine response of painful lumbar disks; 3) demonstration that RDs (AG and RT) and RT projecting into a circumferential annular tear are significant factors related to the intradiskal lidocaine response (separate from relationship to diskogenic pain); and 4) demonstration that AFrags is an additional factor associated with the intradiskal lidocaine response.
Morphology of Painful Degenerative Disks
To evaluate the postdiskogram CT features of the painful disk, we found it necessary to describe and catalog more comprehensively the degenerative features beyond the traditional Dallas diskogram description. Our results confirm the complex nature of the painful degenerative disk and reinforce the observations of many previous anatomic studies.25,43 The intrinsic annular structure is commonly disrupted, leading to RDs (AG and RT). RDs may exist in isolation but often coexist with complex circumferential annular degenerative changes. When assessed comprehensively, abnormalities seen in the severely painful disks in our patients parallel features of meniscal injury and knee internal derangement at MR imaging.22 Parallel features between annular and meniscal derangement included the following: radial annular defects (AGs and RTs), peripheral circumferential annular tears, lamellar circumferential annular tears, bucket-handle tears, annular fragments, and attached annular fragments.22 Peripheral annular pockets may resemble meniscal cyst.22 Multiple annular abnormalities are common, not the exception.
Pain Response to Intradiskal Lidocaine Administration
Only a select group of observations appears to relate to the intradiskal lidocaine response to provoked pain on both univariate and multivariate analysis. The strongest association remains the presence of diskographic contrast leakage (P < .001). Also significant are the observations of RD (AG and RT), RT-into-PAT, and the presence of AFrags.
The RT (grade 3 RT and RT with leakage) and RT-into-PAT are features previously considered significant in the painful lumbar disk.9,10 It is interesting that these features also appear important in the intradiskal lidocaine response to pain after disk provocation, but the mechanism is unclear. Certainly an RD will alter the biomechanical features of the disk. Weight bearing could lead to both stretch and thinning of the residual annular margin in the AG or the peripheral annular tear in RT-into-PAT with subsequent peripheral annular injury or evolving annular leakage. When RT alone is present, the site of the leak is usually clear. With AG or RT-into-PAT, the thinned annular margin is commonly the site of leak on postdiskogram CT.
Most degenerative features identified, including advanced Dallas grade (ie, grades 2 and 3), peripheral circumferential annular tear, lamellar concentric annular tear, attached annular fragments, and bucket-handle tear, do not appear to be associated with the lidocaine response. This parallels the common observation that degenerative disk changes are often identified by MR imaging, but pain is not provoked with stimulation at diskography.5–8
The mechanism by which AFrags inversely influences the intradiskal lidocaine response is not clear. Annular fragmentation with collagen fiber reversal has been described anatomically and is difficult to identify at diskography.44 Annular fragments are found along with nucleus pulposus in surgical diskectomy specimens.44 The presence of AFrags could suggest a more advanced degenerative state of the disk with an ongoing process that develops inflammatory by-products or leads to reduced mechanical stability. The debris, if inflammatory in character, could stimulate reactive changes to the disk inducing granulation tissue, in-growth of pain fibers, or development of adjacent vertebral marrow reaction.41,42,45
The strong statistical significance of diskographic contrast leakage could be related to combined effects of the degenerative process (inflammation) and mechanism behind the leak. Clearly, location of lidocaine contact should play a role in the local-anesthetic effect on pain.
These observations have potential implications for future disk imaging and ultimate patient management. Improved MR imaging characterization of disk degeneration features (annular defects and degenerative features) may be important in targeting the painful disk and predicting pain response to lidocaine. These complex features of disk internal derangement also clearly influence the appearance of the peripheral annular margin, as routinely encountered on CT/MR imaging studies. The lidocaine response to provoked pain at diskography reinforces the diskogenic origin of the pain. Coupled with postdiskogram imaging features, the lidocaine response should improve localization of the disk-specific cause of LBP, better directing cause-specific surgical or medical treatment.
Conclusions
The morphology of the painful lumbar disk studied at diskography is complex, with combinations of annular defects and superimposed degenerative annular features. Diskographic contrast leakage remains strongly statistically associated with the lidocaine response to provoked pain. Additional significant factors include the presence of an RD (AG and RT), RT projecting into a peripheral circumferential annular tear, and the presence of AFrags.
Footnotes
Indicates article with supplemental on-line tables.
References
- Received December 12, 2007.
- Accepted after revision April 9, 2008.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}