
Abstract
SUMMARY: 3D digital subtraction angiography (DSA) allows clinicians to review intracranial aneurysms and other vascular lesions. We report 2 basilar aneurysms that were imaged by both 3D DSA and DynaCT. These 2 techniques produced very different aneurysm appearances. Anterior portions of the aneurysms were invisible on 3D DSA but were revealed by DynaCT. These aneurysms appeared to have been flattened by image artifacts in 3D DSA. Pulsation and gravity are 2 possible causes of aneurysm underestimation.
Digital subtraction angiography (DSA) has been the “gold standard” for many vascular and cerebrovascular imaging studies. 3D rotational DSA enables clinicians to review intracranial aneurysms and other vascular lesions thoroughly in an angiography study or during an interventional procedure. 3D rotational DSA was shown to perform better than either MR or CT angiography in 1 experimental study1 in which time-of-flight MR angiography underestimated aneurysm volumes, whereas CT angiography overestimated. Nevertheless, 3D DSA still is affected by image artifacts that may potentially influence diagnostic accuracy and impact clinical decisions.2 The requirement of uniformly distributed contrast agent across the region of interest often cannot be met in some vascular regions, such as at a lateral saccular aneurysm with a narrow neck.3 Aneurysms with certain orientation also may not be accessible by contrast injection. This is especially true during endovascular procedures when coils are already inside the aneurysm. Moreover, insufficient contrast influx can introduce image artifacts in 3D DSA.3 For example, parent vessels near an aneurysm may appear stenotic.4 In this report, we describe 2 cases of basilar aneurysms for which there are considerable differences in aneurysm volume and morphology between 3D DSA and DynaCT (Siemens Medical Solutions, Erlangen, Germany).5
Case Report
The first case was a 79-year-old woman who had a history of hypertension, diabetes, and hyperlipidemia. She was diagnosed with a basilar tip aneurysm after an episode of fainting. The aneurysm was treated with coil embolization without any incidents. Figure 1 shows the lateral and oblique view of the basilar tip aneurysm from 3D DSA and DynaCT. Because both images have the same resolution, a thick section in the middle of the aneurysm was selected for comparison and is presented in Fig 1.
Top row shows the front (left) and lateral views (middle) of 3D DSA and a rendering image (right). Bottom row shows the front (left) and lateral views (middle) of DynaCT images and overlap of basilar tip aneurysm models from DSA and DynaCT images (right). Aneurysm from 3D DSA is in red and aneurysm from DynaCT is in light gray. A large portion of aneurysm from DynaCT is missing in 3D DSA. 3D DSA indicates 3D digital subtraction angiography.
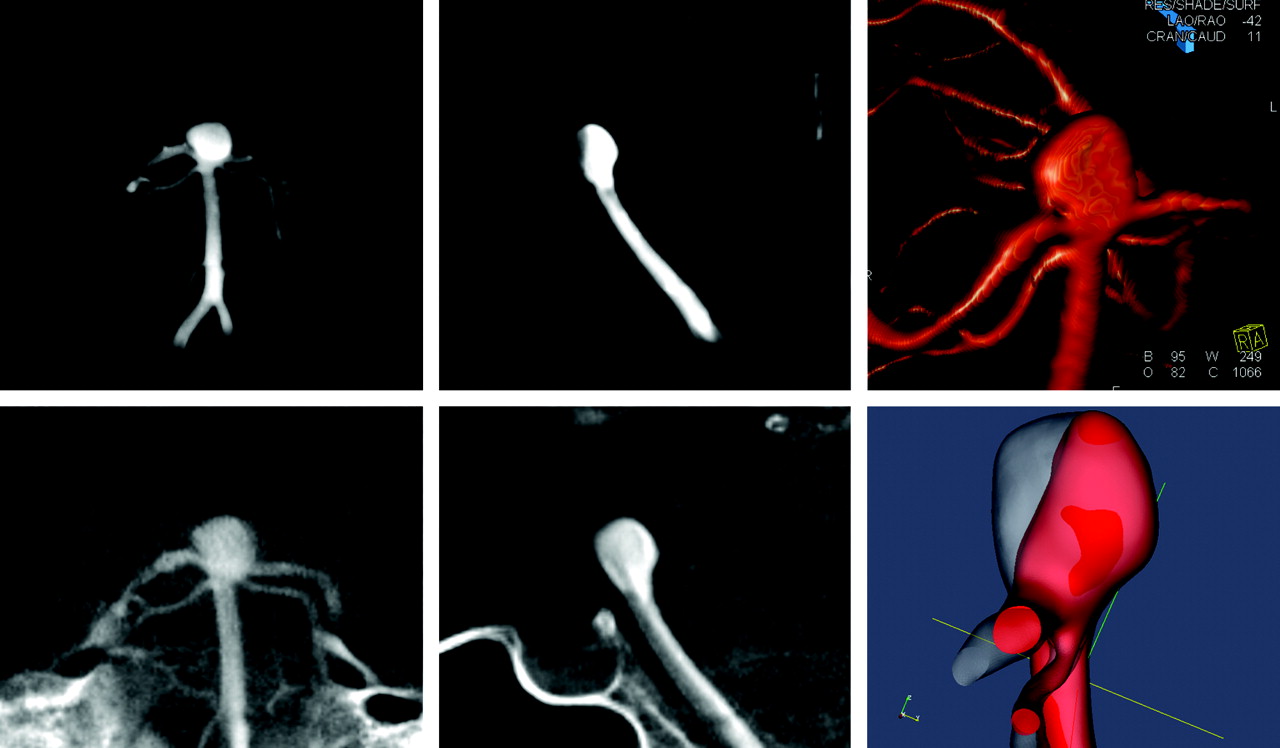
The second case was a 48-year-old man with asthma in whom a basilar trunk aneurysm was diagnosed. His bilobed basilar aneurysm was measured at 9 × 10 mm on the right and 10 × 10 mm on the left. The patient underwent stent placement and coiling for the basilar aneurysm. Both 3D DSA and DynaCT images of the aneurysm are shown in Figure 2. The anterior portion of his right-lobed aneurysm was not visible on 3D DSA.

Top row shows the front (left) and lateral views (middle) of 3D DSA and a rendering image (right). Bottom row shows the front (left) and lateral views (middle) of DynaCT images and overlap of basilar trunk aneurysm models from DSA and DynaCT images (right). Aneurysm from 3D DSA is in red, and aneurysm from DynaCT is in light gray. A portion of aneurysm in DynaCT is missing in 3D DSA. 3D DSA indicates 3D digital subtraction angiography.
Both patients were imaged with 3D DSA and DynaCT protocols on an AXIOM Artis dBA biplane flat detector system with DynaCT capability (Siemens Medical Solutions). For 3D DSA, 30 mL of contrast agent (Omnipaque 300; GE Healthcare, Princeton, NJ) was injected at 2.5 mL/s for 12 seconds, and 275 projections were acquired in 220° within 10 seconds to reconstruct 3D images. There was a 2-second delay for contrast filling. In DynaCT, 22 mL of same contrast agent diluted by the saline (25%) was injected at 1 mL/s, and 543 projections within 220° were acquired for reconstruction. Both procedures had a 2-second x-ray delay and produced 3D images with a 0.4-mm isotropic resolution after reconstruction. The difference in the appearance of aneurysms in DynaCT and 3D DSA after coregistration is presented in Fig 1 for the first case and in Fig 2 for the second. Both cases showed anterior portions of aneurysms in DynaCT, but they were missing from the 3D DSA. In the 3D DSA images, anterior portions of the aneurysms seemed flat on the X-Leonardo workstation (Siemens Medical Solutions); this appearance may be caused by image artifacts.
Discussion
Presence of artifacts may affect the calculation of aneurysm volume and the determination of packing ratio during an endovascular procedure. In turn, this may influence the clinician's perception about the completion of a procedure.6 Aneurysm volumes for these 2 cases were underestimated by approximately 20% in 3D DSA. The basilar trunk aneurysm in case 2 had a narrow neck, and its image appearance may have been affected by contrast deficit during imaging. The basilar tip aneurysm in case 1 had a wider neck and was directly in the flow path for the basilar artery. Therefore, this artifact cannot be explained simply as insufficient flow into the aneurysm.3 The possible mechanisms that resulted in this artifact are the blood flow pulsation and difference in density between blood and contrast medium.
Although contrast medium is injected at a constant rate, blood flow into the aneurysm is pulsatile, resulting in a fluctuation of contrast medium concentration. This can be observed in projective views of unmasked images. Contrast injection also can increase the flow rate considerably in cerebral vessels. The mean flow rate at the basilar artery is approximately 3 mL/s7; thus, an injection of 2.5 mL/s in these cases may have nearly doubled the mean flow rate at the basilar artery. Injection from only one of the vertebral arteries does not produce blood with uniform contrast at the basilar artery, and a portion of the aneurysm consisting of blood mainly from the noninjecting vertebral artery may appear unopacified.
Gravity also may have played an important role in generating this artifact. The contrast medium used for cerebral angiography has a higher density than the blood and often settles at the posterior part of the aneurysm after washout.8 The artifacts in both cases appear at the anterior side of the aneurysms, indicating that it may be difficult for the contrast medium to reach these regions. Given that the specific density of Omnipaque is 1.35, the specific density of blood injected with contrast medium is 1.18 in 3D DSA and 1.02 in DynaCT for the mean flow rate of 2.5 mL/s at the basilar artery. Therefore, the diluted contrast agent used in DynaCT has a density that is closer to that of the blood and may be able to fill the entire aneurysm better than the concentrated contrast medium used in 3D DSA. This may partly explain why the disappearance is always at the anterior side.
In both of these cases, the significant difference between 3D DSA and DynaCT was at the basilar artery. Although the basilar artery is the only artery we have observed so far that is susceptible to this artifact, there is no reason to believe that it is limited to this part of the vasculature. A careful examination of images from 3D DSA and DynaCT at other regions may allow a better understanding of this artifact.
References
- Received January 16, 2007.
- Accepted after revision March 23, 2007.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Critical role of angiographic acquisition modality and reconstruction on morphometric and haemodynamic analysis of intracranial aneurysms
- The utility of cone beam volume CT in the evaluation of thrombosed intracranial aneurysms in subarachnoid hemorrhage
- In vitro and in silico study of intracranial stent treatments for cerebral aneurysms: effects on perforating vessel flows
- The utility of cone beam volume CT in the evaluation of thrombosed intracranial aneurysms in subarachnoid hemorrhage
- Feasibility of Intravenous Flat Panel Detector CT Angiography for Intracranial Arterial Stenosis
- Patient-Specific Computational Hemodynamics of Intracranial Aneurysms from 3D Rotational Angiography and CT Angiography: An In Vivo Reproducibility Study
- Use of Angiographic CT Imaging in the Cardiac Catheterization Laboratory for Congenital Heart Disease
- DynaCT evaluation of in-stent restenosis following Wingspan stenting of intracranial stenosis