
Abstract
SUMMARY: This report presents a 55-year-old woman who underwent 2 Teflon injections in 1971 for a patulous eustachian tube. The patient returned in 2006 with a bloody left otorrhea. A positron-emission tomography-CT scan demonstrated a 2-cm hypermetabolic parapharyngeal mass, initially interpreted as a skull base tumor. Repeat neck CT confirmed a 2-cm hyperattenuated left parapharyngeal granulomatous mass. This is the first reported case of a Teflon granuloma presenting as a false-positive parapharyngeal mass.
Positron-emission tomography (PET) with [18F]fluorodeoxyglucose is a useful clinical tool for diagnosing and staging head and neck malignancies. Although sensitive for assessing neoplasms, increased uptake may be seen in nondiseased muscle, fat, glands, or tissues involved with infection and inflammatory granulomatous disease. This report presents a case of a 55-year-old woman who underwent 2 Teflon injections for treatment of a patulous eustachian tube (pET) in 1971 with a resultant false-positive PET-CT in 2006. In the 1970s, Teflon (polytetrafluoroethylene) was used to treat pET via a Bruning syringe for injection of Teflon into the eustachian tube orifice to create mass effect. This patient underwent 2 Teflon injections for pET treatment in 1971 for discomfort experienced while singing. The patient returned in 2006 for evaluation of left-sided bloody otorrhea. Her work-up included a PET-CT scan demonstrating a hypermetabolic parapharyngeal mass below the skull base measuring 2 cm in diameter, initially interpreted as a skull base tumor at an outside institution. Repeat CT, MR imaging, and biopsy confirmed the presence of a 2-cm hyperattenuated mass in the left parapharyngeal space with no evidence of neoplasm. Combined PET-CT is useful in correlating anatomic and physiologic findings; however, care should be taken when evaluating patients who have had Teflon injections for treatment of head and neck disorders.
Case Report
A 55-year-old woman with history of a left pET presented to her otolaryngologist with an episode of painless left-sided otorrhea. Thirty-five years before, the patient underwent 2 Teflon injections via a Bruning syringe into the eustachian tube (ET) orifice for aural fullness experienced while singing (Fig 1). The patient experienced relief after the 2 injections and requested a third injection from her physician, who declined. Although she experienced mild relief, she subsequently required treatment with 6 pressure equalization tubes in her left ear for recurrent effusions. Physical examination revealed a small left tympanic membrane perforation with thick brown otorrhea. Flexible nasopharyngoscopy demonstrated no masses or obstruction at the torus tubarius. The patient underwent a PET-CT scan in April 2006 demonstrating a 2-cm markedly hypermetabolic mass in the left parapharyngeal space, which was initially interpreted at an outside institution as suspicious for a “skull base tumor” (Fig 2). On CT scans, hyperattenuated material was located just inferior and medial to the left foramen ovale (Fig 3). On MR imaging, the mass was isointense to muscle on both T1- and T2-weighted imaging and demonstrated only rim enhancement (Fig 4A and B). Biopsy confirmed no tumor cells present and that the hypermetabolic mass within the left parapharyngeal space on PET-CT and MR imaging was consistent with a Teflon granuloma.

Bruning syringe for Teflon injection.

PET-CT with 2-cm hypermetabolic mass in the left skull base.

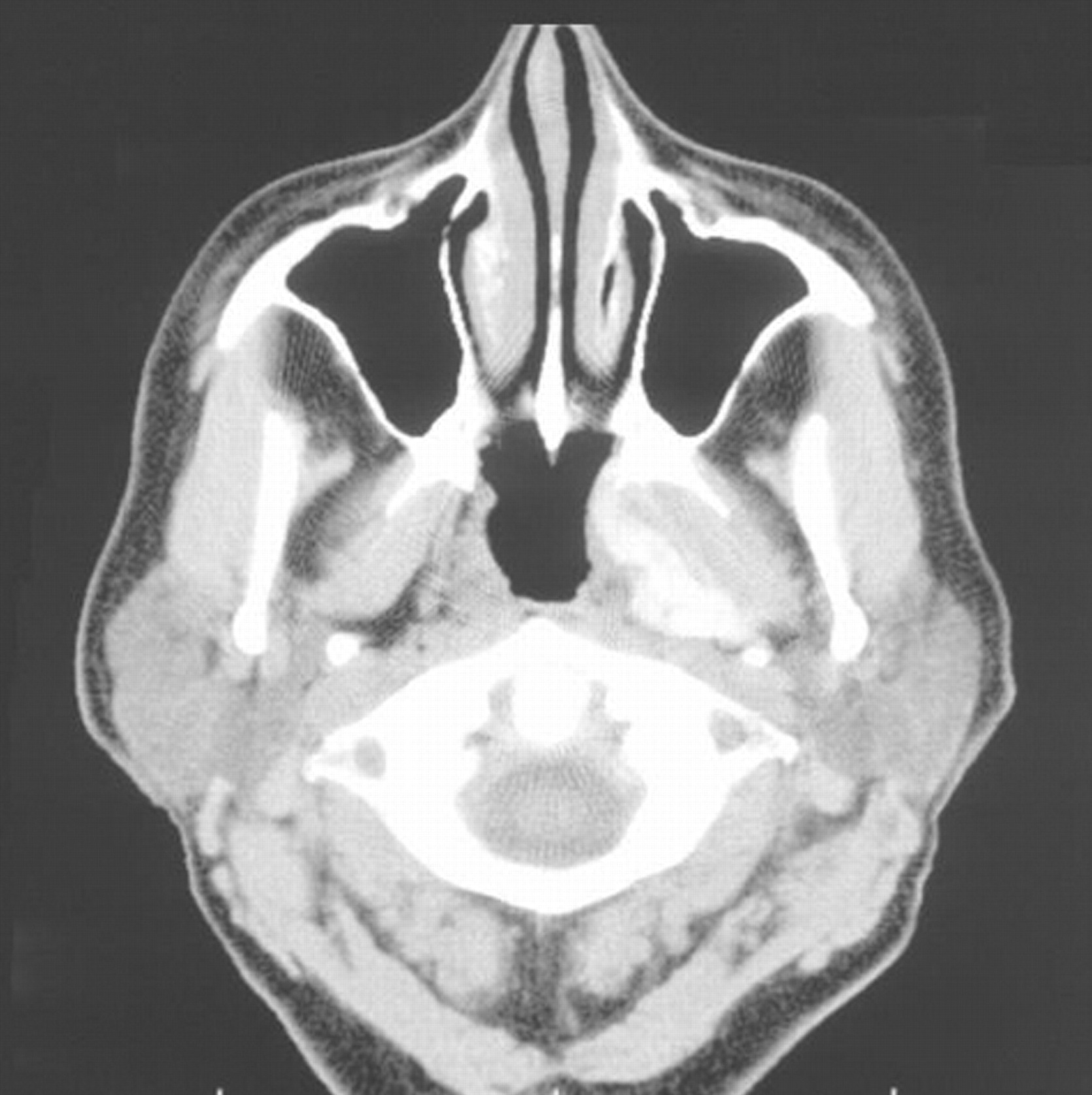
CT scan demonstrating hyperattenuated material within the left parapharyngeal fat.

T1 pregadolinium (A) and postgadolinium (B) with fat saturation demonstrating a mass isointense to muscle in the left parapharyngeal fat with peripheral rim enhancement.
Discussion
The pET first described by Schwartze in 18641 is a rare disorder where the ET remains abnormally patent, creating aural fullness, tinnitus, audible respiratory sounds, and autophony or the sensation of hearing one's own physiologic sounds, speech, respiration, and occasionally pulse. In some patients, the symptoms are so disruptive and disturbing that they lead to psychosis or depression.2 The pET is associated with depletion of soft tissue surrounding the cartilaginous medial two thirds of the ET.2 On otoscopic examination, the tympanic membrane moves freely in and out with respiration, enhanced by obstructing a nostril. Patients often have a hyponasal voice from subconsciously trying to close the ET by closing their velum.2 Recent literature notes that the pET is caused by an incompetent tubal valve from a longitudinal scaphoid defect in the anterior lateral cartilaginous lumen, which does not allow the valve to close completely. This defect can be observed endoscopically and confirmed with CT imaging.1 Although many medical and surgical treatments are described in the literature, no definitive treatment is noted.1,2 In this patient, Teflon was injected into the ET via a Bruning syringe to create mass effect and obstruct the ET.
Teflon
Polytetrafluoroethylene was discovered in 1938 as an inert polymer.3 It was used in the 1960s for vocal cord dysphonia.4 Reports from that time noted foreign body granuloma formation at the sites of injection and of local and distant migration.5,6 Teflon causes a marked inflammatory reaction with formation of giant cells and active phagocytosis. After 2 months, the acute inflammatory reaction may subside, whereas giant cells may persist, actively phagocytosing the Teflon particles. An encapsulating granuloma may start to form at 3–6 months.7 This foreign-body reaction with granulomatous formation and fibrosis may lead to a markedly false-positive PET-CT scan secondary to the propensity of FDG accumulation in both lymphocytes and macrophages.7,8 Although Teflon granulomas in the true cords and nasopharynx occurring secondary to treatment of vocal cord and velopharyngeal insufficiency are reported, this is the first case to our knowledge of a Teflon granuloma in the parapharyngeal space occurring after treatment for a pET. Because PET-CT is now increasingly used in the evaluation of head and neck malignancies, awareness of clinical history of Teflon injections is necessary to avoid a potential false-positive misinterpretation.
Footnotes
Paper previously presented at: Annual Meeting of the American Society of Head and Neck Radiology, September 27–October 1, 2006; Phoenix, Ariz.
References
- Received October 12, 2006.
- Accepted after revision December 1, 2006.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.