
Abstract
BACKGROUND AND PURPOSE: To evaluate the CT characteristics of focal hyperostosis in patients with sinonasal inverted papilloma and to correlate these characteristics with the detection of the origins of tumors.
MATERIALS AND METHODS: Paranasal sinus and nasal cavity CT images of 76 patients were reviewed retrospectively to detect areas within which there was focal hyperostosis. We correlated the sites on the CT scans within which there was focal hyperostosis with the origin of the tumors described in the corresponding patient's medical records. We also evaluated the CT features of focal hyperostosis according to the origin of tumors.
RESULT: Surgical evaluation of 55 lesions with focal hyperostosis in CT images revealed that 49 of these lesions coincided with the actual origin of tumor. The CT-based determination of the locations of the areas of focal hyperostosis corresponded to the actual tumor origin in 89.1% of cases. Especially in cases with focal hyperostosis within the frontal, maxillary, sphenoid, and posterior ethmoid sinuses, areas of focal hyperostosis corresponded to the origin of tumor without exception. In the evaluation of the CT features of focal hyperostosis, 2 patterns of localized bone thickening were noted. Plaquelike bone thickening was seen mainly when focal hyperostosis involved the lateral wall of the nasal cavity. On the other hand, cone-shaped bone thickening was seen only in the walls of the paranasal sinuses or the bony septum.
CONCLUSIONS: A high correlation between the origin of the inverted papilloma and focal hyperostosis on CT might facilitate preoperative prediction of tumor origin by radiologists and rhinologists.
Inverted papilloma is an uncommon tumor of the sinonasal cavity. Due to a high rate of recurrence and an association with squamous cell carcinoma, inverted papillomas are clinically aggressive despite the pathologic benign nature of this type of tumor. Aggressive surgical approaches, such as medial maxillectomy via external incision, have been used to treat inverted papilloma. Since the 1990s, with the accumulated experiences of endoscopic sinus surgical techniques, many surgeons have used relatively less invasive intranasal endoscopic approaches to resect sinonasal inverted papilloma.1 Accurate preoperative evaluation with CT and MR imaging has also influenced the trend toward the use of less invasive surgical approaches.
To date, the radiologic characteristics of sinonasal inverted papilloma have been described.2–8 However, in most of the studies, emphasis has been placed on the diagnostic significance of inverted papilloma. Some of the studies have also focused on the identification of the extent of disease or tumor recurrence. To our knowledge, few studies have been carried out to determine whether image-based characteristics can be used to detect the origin of tumors, and the results of the studies were disappointing.9,10
The identification of the origin of an inverted papilloma is very important for the complete extirpation of such tumors, because most recurrent tumors were localized to the same site as the primary tumors.4 The purposes of this study were to evaluate the CT characteristics of focal hyperostosis in patients with sinonasal inverted papilloma and to correlate these characteristics with the detection of the origins of tumors.
Materials and Methods
From 1994 to 2005, 93 patients with pathologically diagnosed sinonasal inverted papilloma were treated at Samsung Medical Center in Seoul, Korea. Recurrent lesions were identified in 15 of the patients, all of whom had previously undergone either endoscopic surgery or a Caldwell-Luc operation in other institutions. Because sinonasal bone thickening may occur postoperatively, we excluded the patients with a history of sinonasal surgery. Two patients who had undergone MR imaging rather than a CT scan during preoperative evaluation were also excluded. Finally, CT images of 76 patients were reviewed retrospectively. Men outnumbered women 61 to 15 (age range, 25–85 years; mean age, 53.4 years). Squamous cell carcinoma was associated with inverted papilloma in 3 patients.
Endoscopic tumor removal was performed in all patients, not only to obtain tissue for biopsy but also to control the tumor. An adjunctive transantral approach was also used in 15 patients. In 2 patients, tumor positive frontal sinuses were managed with an additional osteoplastic flap.
Either single or multidetector row CT scanners (HiSpeed Advantage, LightSpeed QX/i, LightSpeed Ultra, or LightSpeed 16; GE Medical Systems, Milwaukee, Wis) were used because the patients were scanned over a period of 10 years. Coronal and/or axial CT imaging was performed without administrating a contrast agent. Contrast enhanced CT images, which were excluded from the image analysis in our study, were additionally obtained in some patients. Only coronal CT images were available for 14 patients. The CT scans were obtained with 5 mm collimation and a table speed of 5 mm/s. The reconstruction interval was 2.5–3.0 mm.
Image analysis was performed by a radiologist who had 4 years of experience in head and neck imaging and a rhinologist who had 18 years of experience in endoscopic sinus surgery; both of these analysts were blinded to the medical history of the patients. The CT images of the paranasal sinuses and nasal cavity were examined with bone window setting, to detect areas within where there was focal hyperostosis. When evaluating hyperostosis in the paranasal sinuses (except for the ethmoid sinuses), we considered only focal hyperostosis to be a positive finding. Focal hyperostosis was defined as eccentric bone thickening and sclerosis that involved only a limited portion of the wall of a given paranasal sinus. Concentric, diffuse thickening of bone that involved all sinus walls was considered diffuse hyperostosis; this was not considered a positive finding. We defined focal hyperostosis of the ethmoid sinus as thickening of the bone and sclerosis that involved only a portion of the cells of the ethmoid sinuses. In cases that involved the lateral nasal wall, localized bone thickening and sclerosis of a certain structure, such as the uncinate process or a turbinate, was considered focal hyperostosis. We also evaluated the pattern of localized hyperostosis associated with the location of bony lesions.
We correlated the sites on the CT scans within which there was focal thickening of bone on CT with the origin of the tumors described in the corresponding patient's medical records. The actual origin of a tumor (that is, the area within which the bulk of the tumor was attached) was confirmed by the intraoperative endoscopic evaluation. During the surgery, histopathologic confirmation was used for suspicious mucosa and margins obtained from the sinonasal cavities.
Results
Analysis of CT images revealed a total of 55 areas within which there was focal hyperostosis in 48 of 76 patients. The incidence of focal hyperostosis in patients with inverted papilloma was 63.2%. The most common site of tumor origin was the lateral nasal wall (52.6%). Tumors originated less frequently within the maxillary sinus (25.0%), anterior ethmoid sinus (21.1%), sphenoid sinus (6.6%), frontal sinus (6.6%), septum (2.6%), and posterior ethmoid sinus (2.6%) (Table 1). There was no evidence of bilateral tumor involvement in any patients. In 12 patients, tumors were attached in more than 1 compartment.
CT relationship between the origins of inverted papilloma and areas of focal hyperostosis
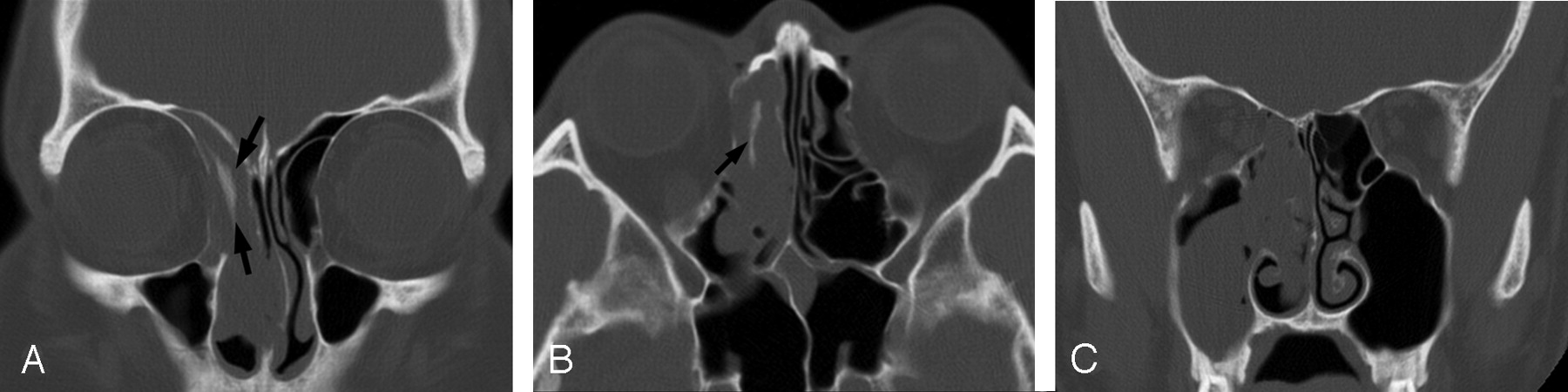
Surgical evaluation of 55 lesions associated with focal hyperostosis in CT images revealed that the location of hyperostosis for 49 of these lesions coincided with the actual tumor attachment site. Therefore, the CT-based determination of the locations of areas of focal hyperostosis corresponded to the actual (surgically determined) tumor origin in 89.1% of cases. In many cases, although tumor masses extended to adjacent sinuses or the nasal cavity, focal bone thickening was limited to the tumor origin as long as the origin did not extend to adjacent sinuses or the nasal cavity (Fig 1).

CT images of a patient with inverted papilloma.
A and B, Axial and coronal CT images show focal plaquelike hyperostosis in part of right ethmoid sinuses (arrows).
C, Although tumor extends to the right maxillary sinus and nasal cavity, no additional foci of hyperostosis are seen. Intraoperative endoscopic examination confirmed the limitation of tumor origin to the ethmoid sinuses.
Areas of focal hyperostosis detected in CT scans were not associated with the actual site of tumor attachment in 6 cases. In these cases, areas of focal hyperostosis were observed in the ethmoid bulla (2 cases), uncinate process, superior turbinate, and middle turbinate. By contrast, in all cases with focal hyperostosis within the nasal septum or frontal, maxillary, and sphenoid sinuses, these sites corresponded to the origin of the tumor.
Our study revealed 2 patterns of localized bone thickening in cases with inverted papilloma (Table 2). When focal hyperostosis involved the walls of the paranasal sinuses or the bony septum of the nasal cavity, the areas of hyperostosis were often highly localized. In 12 such cases, the difference in thickness between the hyperostotic area and the adjacent, unaffected bony wall was highly prominent and resulted in a cone-shaped thickening of the bone (Figs 2 and 3). By contrast, the thickness of focal plaquelike hyperostosis that involved the lateral nasal wall or anterior ethmoid sinus appeared to be relatively even compared with the cone-shaped pattern of hyperostosis (Fig 1). Plaquelike hyperostosis was seen irrespective of the location of tumor origin. However, cone-shaped hyperostosis was seen only when the tumor originated from the walls of the paranasal sinuses except for anterior ethmoid sinuses.

CT and MR images of patients with inverted papilloma of the maxillary sinus.
A, Axial CT image of a patient with inverted papilloma shows cone-shaped focal hyperostosis involving the posterior wall of the left maxillary sinus (arrows).
B, Sagittal T2-weighted MR image of the patient clearly shows the centrifugal pattern of tumor growth with a hyperostotic focus (white arrow) at the posterior wall of the left maxillary sinus, which was confirmed to be a tumor origin by surgery.
C, Axial CT image of another patient shows cone-shaped hyperostosis (arrow) involving the anterior wall of the left maxillary sinus, which was proved to be the origin of inverted papilloma by intraoperative endoscopy.

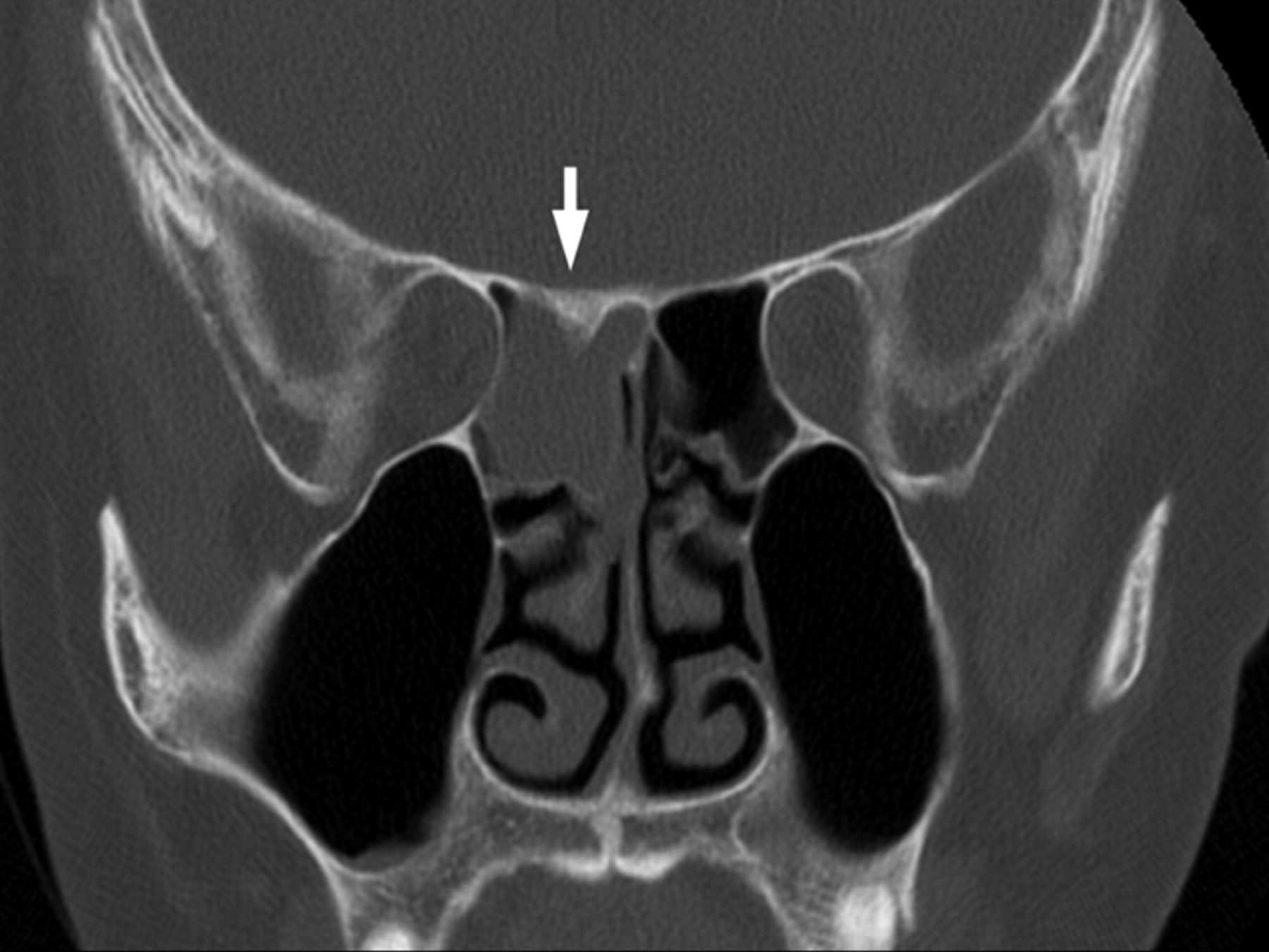
Coronal CT image in a patient with inverted papilloma shows localized cone-shaped hyperostosis of the superior wall of the posterior ethmoid sinus (white arrow). Intraoperative endoscopic examination confirmed that the origin of tumor was located at the superior wall of the right posterior ethmoid sinus.
CT patterns of focal hyperostosis in inverted papilloma
When the origins of inverted papilloma were correlated with the areas of focal hyperostosis on CT, areas of cone-shaped hyperostosis always coincided with actual tumor origin, without exception. On the contrary, some of plaquelike hyperostotic area failed to predict the origin of inverted papilloma.
Discussion
Inverted papilloma is characterized by frequent recurrence and a potential for malignancy. Therefore, accurate preoperative mapping of tumor locations is crucial to facilitate the effective resection of this type of tumor. CT and MR imaging can provide valuable information that can be used to delineate the extent of inverted papilloma. MR imaging can distinguish soft tissue tumors from adjacent areas of inflammation, and this imaging technique is superior to CT imaging for defining the location of a tumor.11 On the contrary, CT imaging is superior to MR imaging for evaluating changes in bone, such as hyperostosis, bone erosion, and bone destruction. In addition, for most rhinologists, CT imaging in the coronal plane is the method of choice to create roadmaps in planning for endoscopic sinus surgery.12 However, CT imaging has been reported to be of limited use in detecting the origin of tumors. Because of these limitations in the imaging of sinonasal inverted papilloma, endoscopic evaluation during surgery has been regarded as the only reliable method for determining the areas in which tumors are attached.9,10
Changes in bone that have been detected using CT scanning in patients with inverted papilloma include intratumoral calcification, thinning, bowing, erosion, and sclerosis.4,5,7 CT findings of bone thinning, bowing, and erosion might be due to an increase in the pressure exerted by the tumor as the tumor grows. Therefore, it is unlikely that such changes in bone are associated with the origin site of tumor. In our study, however, there was a correlation between CT-based detection of areas within which there were sclerotic changes or hyperostosis and endoscopic determination of the tumor origin. Although sclerotic changes of bone in the sinonasal inverted papilloma have been described previously,4,5,13 the relationship between these findings and the origin of tumors has not been examined in detail.
In general, the origins of sinonasal inverted papillomas are localized to focal areas within the walls of the sinonasal cavity, despite the fact that these tumors usually have a large volume. Inverted papillomas are well known to exhibit centrifugal growth pattern.3,14 For example, even if the tumor of nasal cavity also extends to the medial wall of the maxillary sinus and fills the antrum, endoscopic medial maxillectomy is not required, provided the tumor origin is still localized in the nasal cavity. On the contrary, when the hyperostosis of the sinus wall is associated with maxillary sinus tumor, endoscopic medial maxillectomy must be planned preoperatively, because the tumor origin would be highly expected to be in the maxillary sinus. Lee et al10 emphasized that it is important to initially determine the location of the tumor attachment site during surgery. Therefore, preoperative identification of the tumor origin would be helpful in choosing a proper surgical approach. Preoperative CT-based detection of tumor origin may be especially helpful in case of frontal sinus disease, in which we often have difficulty in observing the origin of tumor.
The mechanism that underlies the thickening of bone at the tumor origin of inverted papilloma is unknown. We could not determine the cause of the difference in the pattern of hyperostosis according to the tumor origin, either. Hyperostosis at the tumor attachment site is a characteristic of meningiomas, and Pieper et al15 provided several possible explanations of hyperostosis at the attachment site of meningiomas. Some of the explanations might also apply to hyperostosis in inverted papilloma, and they are tumor-induced vascular disruption within the underlying bone, irritation of the bone by the tumor, and so forth. A large bulky tumor volume associated with a relatively small area of attachment might result in hypervascularization at the attachment site, which could affect bone growth within the site. Indeed, we have often encountered substantial bleeding at sites where the cone-shaped hyperostotic bone has been removed during surgery in cases with inverted papilloma that originated within the paranasal sinuses. Eisen et al16 proposed that an increase in vascularity due to sinonasal inverted papilloma may cause tinnitus.
Bone resorption or neogenesis is also associated with in chronic paranasal sinusitis,17,18 and some authors have reported that sclerotic bone changes in inverted papilloma were related to accompanying or previous sinusitis.4,13 On the contrary, Lund and Lloyd5 reported the different patterns of hyperostosis between inverted papilloma and chronic paranasal sinusitis. According to our study, hyperostosis in inverted papilloma was usually localized and eccentric, which was different from even, diffuse, and concentric pattern of sclerotic change in chronic paranasal sinusitis. Therefore we concur with Lund and Lloyd and believe that hyperostosis in inverted papilloma might have nothing to do with chronic paranasal sinusitis.
Inverting papillomas commonly originate from the lateral nasal wall or middle meatus and extend to adjacent paranasal sinuses or other nearby structures.19 However, our series showed relatively lower rate of tumor origin from the lateral nasal wall and the septum compared with other studies. Our institute is a tertiary care center; usually, relatively difficult cases for surgery are referred from other hospitals. Therefore, the discordance between our study and other studies might be a result of selection bias.
Because sinonasal inverted papillomas have a high probability of recurrence and are locally aggressive, appropriate preoperative assessment of these tumors is crucial for successful treatment. Most recurrences occur at the same site at which the tumor originated and are frequently attributable to incomplete local resection.20,21 Furthermore, tumoral multiplicity has not been demonstrated conclusively to be the cause of tumor recurrence.22 Therefore, to prevent postoperative recurrence of tumors, precise preoperative identification of the tumor origin might be at least as important as detecting the extent of tumor invasion.
Not all patients with inverted papilloma showed the CT finding of focal hyperostosis in our study. In those cases without focal hyperostosis, we could not find any radiologic finding that helped in the detection of the origin of tumor. However, when the finding of focal hyperostosis was seen, we could predict the origin of inverted papilloma with a high probability. Therefore, CT-based preoperative detection of tumor origin, though not possible in all cases, might facilitate the planning of surgery and prevent unnecessary resection of unaffected anatomic structures.
Conclusions
Focal hyperostosis visible in CT scans is associated frequently with sinonasal inverted papilloma. CT scans can be used to differentiate focal hyperostosis from diffuse bone thickening, which is usually associated with chronic paranasal sinusitis. Two distinct patterns of focal hyperostosis are associated with inverted papilloma. A high correlation between the origin of the inverted papilloma and focal hyperostosis might facilitate preoperative prediction of tumor origin by radiologists and rhinologists.
References
- Received March 30, 2006.
- Accepted after revision June 28, 2006.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}