
We read with interest the report by Mitchell et al1 of 4 cases of ectopic posterior pituitary lobe and periventricular heterotopia on MR imaging studies. The authors suggested that ectopic posterior pituitary lobe with growth hormone deficiency is part of a spectrum associated with septo-optic dysplasia and concluded that the coexistence of periventricular heterotopia dysplasia implies a common underlying genetic mechanism. Further, in 1 case, they found the presence of a heterozygous HESX1 mutation, a gene associated with ectopic posterior pituitary lobe and septo-optic dysplasia, and suggested that this gene is important in the development of both ectopic posterior pituitary lobe and periventricular heterotopia.
We report a case of a 4-year-old boy with a history of seizures. The patient had an episode of convulsive seizure in March 2006, with a left focal onset. His medical history included panhypopituitarism and optic atrophy of the right eye. Physical examination was significant for a pale right optic disk. MR imaging revealed ectopic posterior pituitary lobe, a hypoplastic pituitary, and a hypoplastic optic chiasm on the T1-weighted sagittal images (Fig 1A, -B). Incidentally, the pituitary stalk could not be visualized. T2-weighted axial and coronal fluid-attenuated inversion recovery (FLAIR) images showed bifrontal cortical dysplasia and a strip of ectopic gray matter extending from the head of the right caudate nuclei to the orbitofrontal lobe (Fig 2A, -B). T2-weighted axial images also revealed small optic nerves, especially on the right side.
The syndrome of septo-optic dysplasia consists of a combination of malformations including hypoplasia or absence of a septum pellucidum or corpus callosum, optic nerve hypoplasia or dysplasia, pituitary-hypothalamic dysfunction, and occasionally other cerebral abnormalities such as schizencephaly or cortical dysplasia. This heterogeneity of features has resulted in some disagreement as to how septo-optic dysplasia is to be defined and categorized. For example, both Barkovich et al2 and Miller et al3 attempted to define and classify septo-optic dysplasia into distinct anatomic subsets. However, Polizzi et al4 suggested that septo-optic dysplasia should be recategorized as a heterogeneous malformation syndrome encompassing multiple brain, endocrine, and systemic anomalies, rather than a single, precisely defined entity. Our patient did not have hypoplasia or absence of the septum pellucidum; however, the presence of an ectopic posterior pituitary lobe, optic nerve hypoplasia, optic chiasm hypoplasia, cortical dysplasia, and ectopic gray matter suggests features of septo-optic dysplasia.
We, therefore, agree with Mitchell et al1 that the presence of ectopic posterior pituitary lobe is often associated with other important cerebral malformations, even in the absence of classic features of septo-optic dysplasia. Like the cases presented by Mitchell et al,1 our patient had an ectopic posterior pituitary lobe. One difference is that the pituitary stalk in our patient could not be well visualized. We are curious as to whether the etiology of this finding had a common mechanism with the other abnormalities or if this was secondary to trauma or some other cause. In addition, our patient presented with bifrontal cortical dysplasia and an ectopic strip of gray matter in the right frontal lobe. These entities are due to abnormalities in neuronal cell migration, as is periventricular heterotopia seen in all 4 of Mitchell’s patients.
Thus, we support the theory that these cerebral malformations may have a common mechanism in the development of ectopic posterior pituitary lobe and suggest that they are part of a complex of features seen in septo-optic dysplasia.

A, Sagittal T1-weighted image shows a hyperintensity corresponding to an ectopic posterior pituitary lobe located in the hypothalamic area. The pituitary is small.
B, Paramedian sagittal T1-weighted image reveals a thin optic chiasm and a small pituitary.
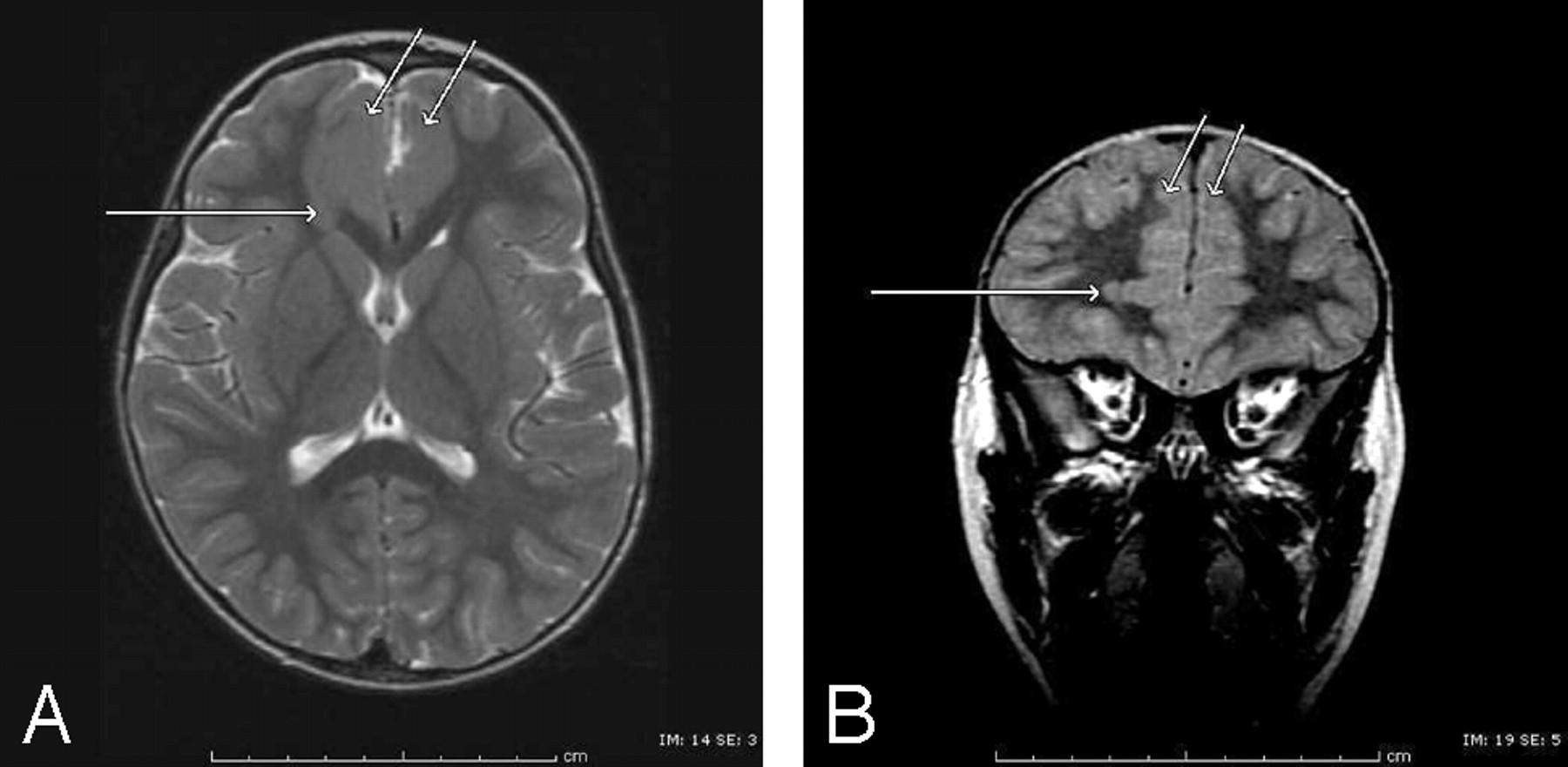
A, Axial T2-weighted image reveals thickening of the cortical gray matter at the medial aspect of both frontal lobes, compatible with bifrontal cortical dysplasia (short arrows). Also seen is a strip of ectopic gray matter extending from the head of the right caudate nuclei to the orbitofrontal cortex (long arrow).
B, Coronal FLAIR image shows a strip of ectopic gray matter extending from the head of the right caudate nuclei to the orbitofrontal cortex (long arrow) as well as bifrontal thickening of the cortical gray matter (short arrows).
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.