
Abstract
SUMMARY: Pleomorphic adenomas (PAs), also known as benign mixed tumors, are common tumors of the parotid gland. These tumors occasionally undergo malignant transformation, with potentially devastating consequences. This case report presents the clinical and radiographic features of a rare case of biopsy proved brain and spinal cord metastases arising from carcinoma ex PA of the parotid gland.
Pleomorphic adenomas (PAs), also known as benign mixed tumors because of the presence of both epithelial elements and mesenchymal tissue, are the most common neoplasms of the major salivary glands. They account for approximately 65% of all salivary gland neoplasms and 70%–80% of all benign tumors of the major salivary glands.1,2 Between 65%–85% of PAs arise in parotid glands, 8% in submandibular glands, and only 6%–7% in minor salivary glands.1 Approximately 65%–75% of all parotid tumors are thought to be PAs.3 Most of these parotid PAs occur lateral to the plane of the facial nerve in the parotid gland.4,5 Generally thought to be indolent and slow-growing tumors, they typically present as a well-demarcated, solitary, painless mass in middle-aged patients. It is not uncommon for PAs to recur, and, though benign, a subset will undergo malignant transformation. We report a case of an adult male patient who, despite parotidectomy, experienced recurrence of a parotid carcinoma ex PA that resulted in death because of development of widespread metastatic carcinoma within the central nervous system (CNS).
Case Report
A 36-year-old Somali male physician, who previously specialized in the care of patients with tuberculosis before immigrating to the United States, was initially diagnosed and treated for a grade 4 carcinoma ex PA of the right parotid gland with local nodal and extranodal extension (Fig 1). At the time of his diagnosis, he underwent a right total parotidectomy with right modified radical neck dissection and postoperative adjuvant radiation therapy. Shortly after his initial diagnosis, the patient was also diagnosed with prostatic tuberculosis. Nineteen months after completion of radiation therapy for the parotid carcinoma ex PA, he presented to the emergency department with a 3-week history of malaise, fever, gait imbalance, and fatigue. He was diagnosed with and treated for pneumonia. His symptoms progressed, however, and he began to experience generalized weakness and a decline in his mental status. On physical examination, he was found to have palpable nodules in the left submandibular region and the right supraclavicular region. He was admitted for further work-up, including fine needle aspiration of a left submandibular lymph node, which revealed metastatic grade 4 (of 4) adenocarcinoma. Because of his decline in mental status, he also underwent MR imaging of the brain (Fig 2), which demonstrated numerous enhancing nodular lesions with surrounding vasogenic edema. There was involvement of the cerebral hemispheres, the cerebellum, and the brain stem. Several of the lesions demonstrated an atypical targetoid, lamellated appearance. None of the lesions demonstrated diffusion restriction. These findings on the MR imaging of the brain prompted subsequent MR imaging of the spinal cord (Fig 3). Within the spinal cord, a single enhancing nodule was identified at T1. There was associated patchy T2 signal intensity hyperintensity involving most of the cervical spinal cord. The clinical presentation and the patient’s history of extrapulmonary tuberculosis involving the genitourinary tract suggested the possibility of disseminated tuberculosis as the etiology for the patient’s brain and spinal cord lesions; however, in light of his history of a high-grade parotid malignancy, CNS metastases were also a diagnostic consideration. Consequently, a stereotactic biopsy of a right frontal lobe lesion was performed. The biopsy revealed high-grade carcinoma consistent with a metastasis from carcinoma ex PA of a parotid primary (Fig 4). Two months after this diagnosis, the patient died consequent to metastatic disease.

A, Axial image from noncontrast CT examination of the head demonstrates a heterogeneous mass involving the superficial right parotid gland (arrow).
B, Photomicrograph of tumor in A demonstrates nests of basophilic tumor cells arising from a PA. (H&E stain × 100).

A, Postgadolinium T1-weighted MR images demonstrate multiple enhancing nodular lesions throughout both cerebral and cerebellar hemispheres, several of which have an unusual lamellated pattern of enhancement.
B, T2-weighted and FLAIR MR images with paired postgadolinium T1-weighted images demonstrate significant vasogenic edema associated with several of these lesions.

MR imaging of the cervical spine. T2-weighted image demonstrates patchy increased T2 signal intensity in the cervical cord (A). Postgadolinium T1-weighted image demonstrates an enhancing intramedullary nodular lesion at the T1 level (B, arrow).
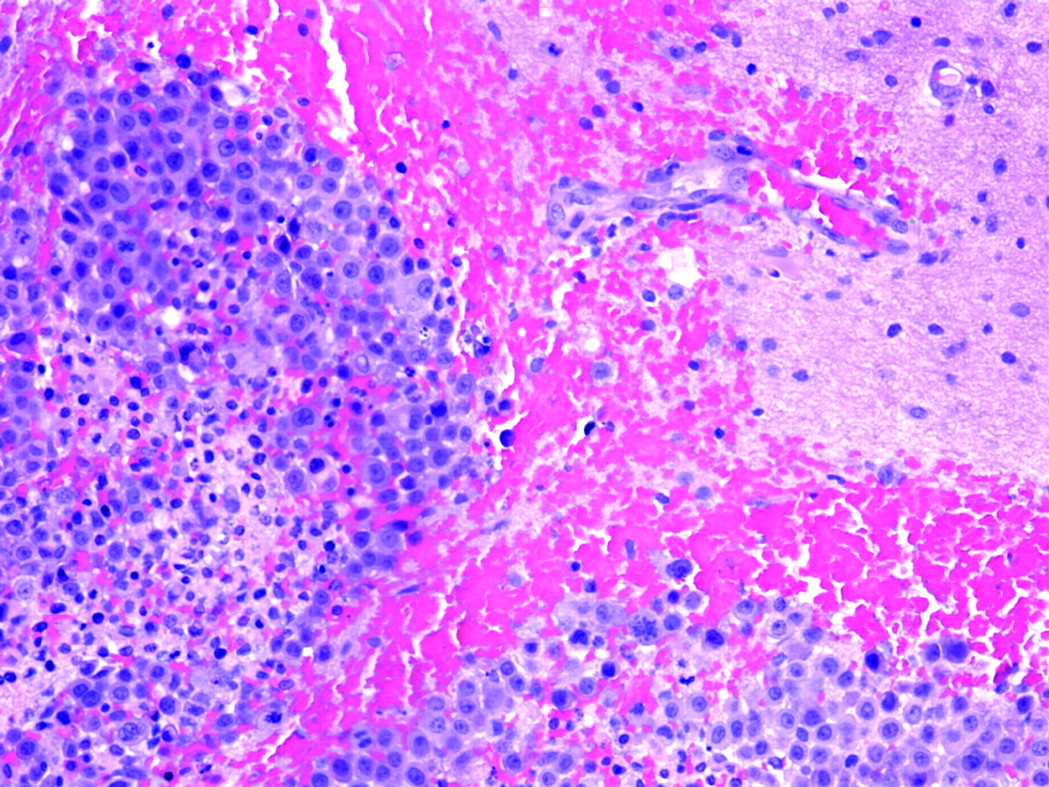
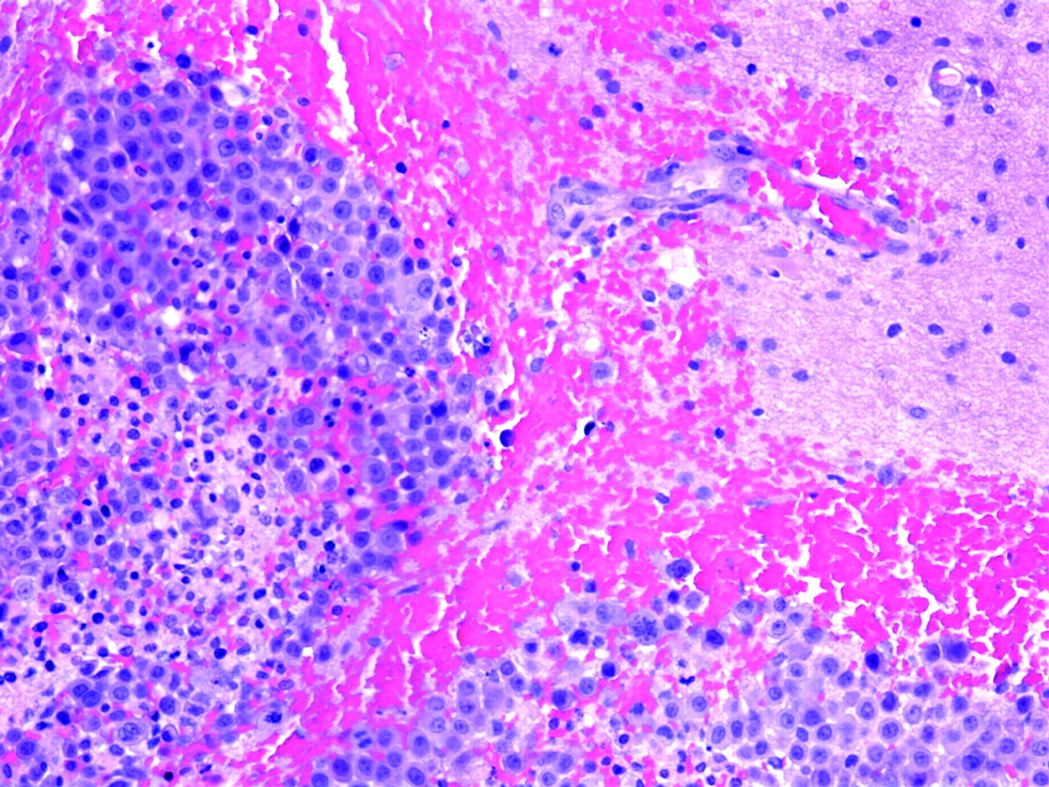
Photomicrograph of brain biopsy specimen shows metastatic grade (4/4) carcinoma (left) invading normal brain parenchyma (right) (H&E stain × 100).
Discussion
PAs are frequently encountered tumors of the parotid glands. Although benign, as many as 25% undergo carcinomatous transformation if left untreated.4,6,7 Carcinomatous transformation within a benign mixed tumor in which the initial benign elements are still identifiable is termed carcinoma ex PA. The carcinomatous element is typically adenocarcinoma not otherwise specified or salivary duct carcinoma.8 A number of additional rare carcinoma subtypes, however, are also known to occur in these tumors. Carcinoma ex PA may also arise as a recurrence in a patient in whom a benign mixed tumor was previously resected. The typical patient with carcinoma ex PA has a longstanding history of PA and suddenly experiences an increase in size, pain, or facial nerve involvement. These tumors account for about 12% of all malignant neoplasms of the salivary glands.9,10 The carcinoma ex PA is usually a more poorly circumscribed mass than the benign PA, is most likely to occur within the major salivary glands, and typically occurs in patients in the 6th–8th decades of life. Carcinomas ex PAs are prone to frequent recurrence and commonly metastasize. These tumors are associated with a 5-year survival rate of about 50%.1 The development of associated metastatic disease is considered preterminal.1
Two other types of malignancies are also associated with PAs, though they are even rarer. Carcinosarcoma, a “true” malignant mixed tumor, is composed of both carcinomatous and sarcomatous elements. This is in contrast to the carcinoma ex PA in which only the epithelial element undergoes malignant transformation. Carcinosarcoma arises most commonly in the parotid gland and carries a grave prognosis. One third of carcinosarcomas occur in patients with previous or coexisting PAs.11 Metastasizing “benign” mixed tumor (MZMT) is an extremely rare sequela of PAs. Although no malignant features are identified within a benign mixed tumor, distant metastases occur. These metastatic implants are also histologically benign in appearance.9,12 Patients with MZMT invariably have a history of having a benign mixed tumor removed, and they typically have had multiple recurrences before metastatic involvement.13
Because of the potential for malignant transformation, surgical excision is currently the most widely accepted treatment of PAs.14 Benign PAs have a tendency to recur at a rate of 1%–50%, depending largely on the surgical technique of excision.1 Enucleation of the adenoma results in a higher rate of recurrence versus superficial or total parotidectomy. The configuration of the tumor, which has multiple pod- or finger-like extensions, also contributes to the high rate of recurrence. The tumor extensions may reach beyond the confines of the main tumor bulk and the surgical margin, resulting in undetected residual tumor, and subsequent multinodular “recurrences” in the region of origin. In addition, PAs have a false-capsule composed of compressed surrounding normal salivary tissue. Recurrence (or residual tumor) tends to be more likely in patients in whom capsular rupture occurs at the time of surgical resection and in patients in whom the podlike extensions of tumor extend beyond the capsule.1,14 Similarly, if a focus of malignant transformation is confined within the fibrous capsule, it tends to behave in a more benign manner and carry a better prognosis, which is similar to that of a benign mixed tumor.8,9,15–17 Conversely, malignancies extending beyond the tumor capsule tend to behave more aggressively and are associated with a poor prognosis with the 5-year survival rate of 25%–65%.9,10 According to LiVolsi and Perzin15 and Tortoledo et al,17 the extent of tumor infiltration beyond the capsule is the most reliable prognostic marker. Although containment within the tumor capsule has been found to be an indicator of benign clinical behavior, Felix et al recently reported a case in which a completely encapsulated carcinoma ex PA presented with regional lymph node metastatic dissemination.18
Our case demonstrates a rare, end stage complication of parotid PA, malignant conversion followed by diffuse CNS metastases. Although local lymphatic spread is the most common means by which these tumors metastasize, hematogenous distant metastases have been reported to occur in as many as 44% of patients with carcinoma ex PA.8 Previously reported sites of hematogenous metastases include the lung, pleura, kidney, and ocular choroid. In our case, both regional lymphatic and distant hematogenous spread were identified. This case is exceptional because, to our knowledge, the combination of brain and spinal cord metastases from a parotid carcinoma ex PA has not previously been reported. From a practical standpoint, however, the true importance of this case is that it poignantly illustrates the devastating outcome that may result consequent to delay in diagnosis and treatment of a benign parotid PA. Because of the significant risk of malignant conversion, the presence of a PA should always be regarded as a premalignant condition and treated aggressively with appropriate surgery. Observational follow-up is an inappropriate management strategy in light of the high mortality rate associated with the unpredictable occurrence of malignant transformation.
Conclusion
The fact that PAs are classified as benign tumors should not overshadow the wide range of biologic behaviors associated with these neoplasms. This report illustrates a rare but deadly outcome, CNS metastases, due to malignant transformation of a PA. Consequently, this case strengthens the argument for complete surgical excision of all parotid PAs.
Footnotes
Presented as an excerpta extraordinaire at the 43rd annual meeting of the ASNR, Toronto, Ontario, Canada, May 21–27, 2005.
References
- Received August 29, 2005.
- Accepted after revision September 22, 2005.
- Copyright © American Society of Neuroradiology
In this issue









{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.