
Abstract
BACKGROUND AND PURPOSE: Several techniques, including chymopapain, mechanical aspiration, laser-based disk decompression, and endoscopic keyhole surgery, have been proposed as minimally invasive alternatives to fusion for treating cervical disk herniation, though none has gained wide acceptance. The purpose of this study was to assess feasibility, safety, and preliminary clinical results of percutaneous plasma-mediated radio-frequency–based diskectomy for cervical disk herniation.
METHODS: Patients (N = 55) with cervical soft disk protrusion were treated over a 29-month period. They had radicular pain; 3 patients also had moderate myelopathy. The procedure was performed with the Perc-DC SpineWand by using an anterior approach. Most cases were conducted with local anesthetic on an outpatient basis. Clinical outcomes were graded by using the Macnab criteria.
RESULTS: At 2 months, outcomes were good or excellent in 44/55 (80%) patients; the success rate was similar at 6 months, when 44 (85%) patients (n = 52/55) had good or excellent results. One clinically relevant complication (infectious diskitis) occurred within the first month postprocedure and was successfully treated. One technical complication (in situ rupture of the device tip) was observed; however, the patient remained asymptomatic during the 2-year follow-up. The 3 patients with clinical myelopathy experienced regression of cord compression symptoms; MR imaging in 2 patients showed morphologic evidence of reduction of cord compression.
CONCLUSIONS: Plasma radio-frequency–based diskectomy in the cervical spine appears to be a minimally invasive low-risk approach, which is easy to perform, associated with only minimal discomfort to the patient, and effective in the short term.
Open surgery for cervical disk herniation is a well-established highly successful procedure, though it possesses the usual drawbacks of almost any surgical intervention, including damage to bone and muscle; risk of neural, parenchymal, and vascular lesions; and a potentially long postoperative recovery. Consequently, psychologic acceptance of cervical disk open surgery by most prospective patients is low. Surgical techniques entailing an interbody fusion are also burdened by the longer term risk of stress overload, chronic damage to the adjacent disks, and other complications.1–5 For these reasons, a number of minimally invasive intradiskal methods for treating cervical disk herniation, most commonly involving mechanical or energy-based removal of some portion of the nucleus pulposus, have been developed over the last few years.6–13
Percutaneous plasma radio-frequency–based diskectomy, or the Nucleoplasty procedure (ArthroCare, Sunnyvale, Calif), was initially used to treat symptomatic contained protrusion in the lumbar spine. This procedure was reported to be safe and was associated with acceptable clinical success.14–16 It is conducted by using a bipolar radio-frequency–based device, which functions via a plasma-mediated process,17–19 to perform precise removal of disk tissue. In this process, bipolar voltage pulses at 100 kHz are applied to the active electrode at the distal end of the device, which produces a strong electric field region around the electrode. The electrolytes in the surrounding conductive medium (eg, sodium ions resident within the nucleus pulposus) respond to the electric fields, and if the voltage is sufficiently large, a localized finely focused plasma field (ionized vapor) is produced between the electrode and adjacent tissue. The plasma field comprises a complex mixture of gas-phase radical chemically reactive and nonreactive molecules and a very small fraction of ionized particles (predominately positive ions and electrons), some of which can break molecular bonds in the adjacent tissue by energetic particle bombardment and chemical reactions. Usually, visible light emissions are observed coincidentally with onset of the plasma formation. The organic molecules in the disk material (particularly long-chain molecules such as collagen and the like) are thought to be susceptible to fragmentation by the plasma particles, resulting in their conversion into liquid and gaseous products that subsequently desorb from the targeted site.19 The net result is a reduction of soft-tissue volume and effective excision of the soft tissue within the nucleus. The plasma radio-frequency–based process has been reported to have minimal histopathologic effect on tissue immediately adjacent to the treated site.20,21
In February 2003, we began an outcome research study of percutaneous plasma radio-frequency–based diskectomy for treating patients with symptomatic cervical disk herniation. The surgical technique was derived from our previous experience in the minimally invasive treatment of such pathology6 by using the Nucleotome procedure22 (Clarus Medical, Minneapolis, Minn) and on our wide experience in the use of plasma-mediated radio-frequency–based diskectomy to treat contained disk protrusion at the lumbar levels (G. Bonaldi, papers presented at the Italian Society of Neuroradiology, September 22–25, 2004, Milan, Italy; and at the Stroke and Spine Meeting, April 26–27, 2006, Naples, Italy). The aim of this study was to determine the feasibility and the safety of an energy-based approach for diskectomy when used in the cervical spine. Preliminary clinical results were also collected and examined with the aim of evaluating the efficacy of the procedure compared with the results of other minimally invasive procedures, as reported in the literature.6–13
Materials and Methods
This was an uncontrolled prospective case series study. The study received approval of the Institutional Review Board of Riuniti Hospital. All patients provided informed consent before undergoing the procedure.
Patients
Between February 2003 and July 2005, 55 patients (30 men and 25 women), with ages ranging from 27 to 64 years (mean, 41.7 ± 8.3 years), received plasma radio-frequency–based percutaneous diskectomy. At presentation, all patients had cervical and upper limb pain, in most cases radiating down to the hand and often to the scapular, occipital, or auricular regions. None of these patients had neck pain alone. Preoperative clinical evaluation included a neurologic examination, which was performed by both the treating physician and an independent neurologist or neurosurgeon. Twenty-six patients had only pain, sometimes accompanied by paresthesias; none of these patients demonstrated neurologic deficits. At the neurologic examination, 10 patients showed hypoesthesia, disesthesias, or hyporeflexia consistent with the radicular level compressed by the herniation. Fourteen patients also showed hyposthenia associated with mild-to-moderate hypotrophia of the muscular territory involved. In 1 patient, the neurologic examination of the upper limb was obscured by the presence of multiple sclerosis and in another, by sequelae of an intervention for humeral osteoid osteoma with radial injury. In 3 patients, moderate myelopathy was detected, which was characterized by lower limb hyposthenia with pyramidal signs and sensory disturbances.
All patients underwent at least 1 preoperative CT and 1 MR imaging diagnostic study. Patients receiving plasma radio-frequency–based disk decompression had a bulging, protruding, or extruded disk, which was not sequestrated or migrated;23–25 the herniation compressed the exiting nerve root, the thecal sac, or, in 3 patients, the spinal cord. Only soft disk herniations, as determined by MR imaging and CT studies, were treated. Disk herniations were encountered in our series at 3 disk levels: C4–5 (n = 5), C5–6 (n = 37), and C6–7 (n = 33). Thirty-six patients received treatment at 1 level, 18 patients were treated at 2 levels, and 1 patient was treated at 3 levels. At all attempted levels the procedure was successful.
Sonography of the neck was performed the day before the procedure to rule out possible anatomic variants or pathologic conditions that could obscure the percutaneous surgical pathway and prevent a safe approach into the disk nucleus. In particular, we assessed the following: 1) the thyroid, to determine presence of normal echotexture and to rule out focal alterations such as nodules or cysts; 2) the lymph nodes, to confirm normal appearance; and 3) the arteries (superior and inferior thyroid and carotid) and recurrent laryngeal nerve, to confirm normal position.26–27
Percutaneous Diskectomy Procedure
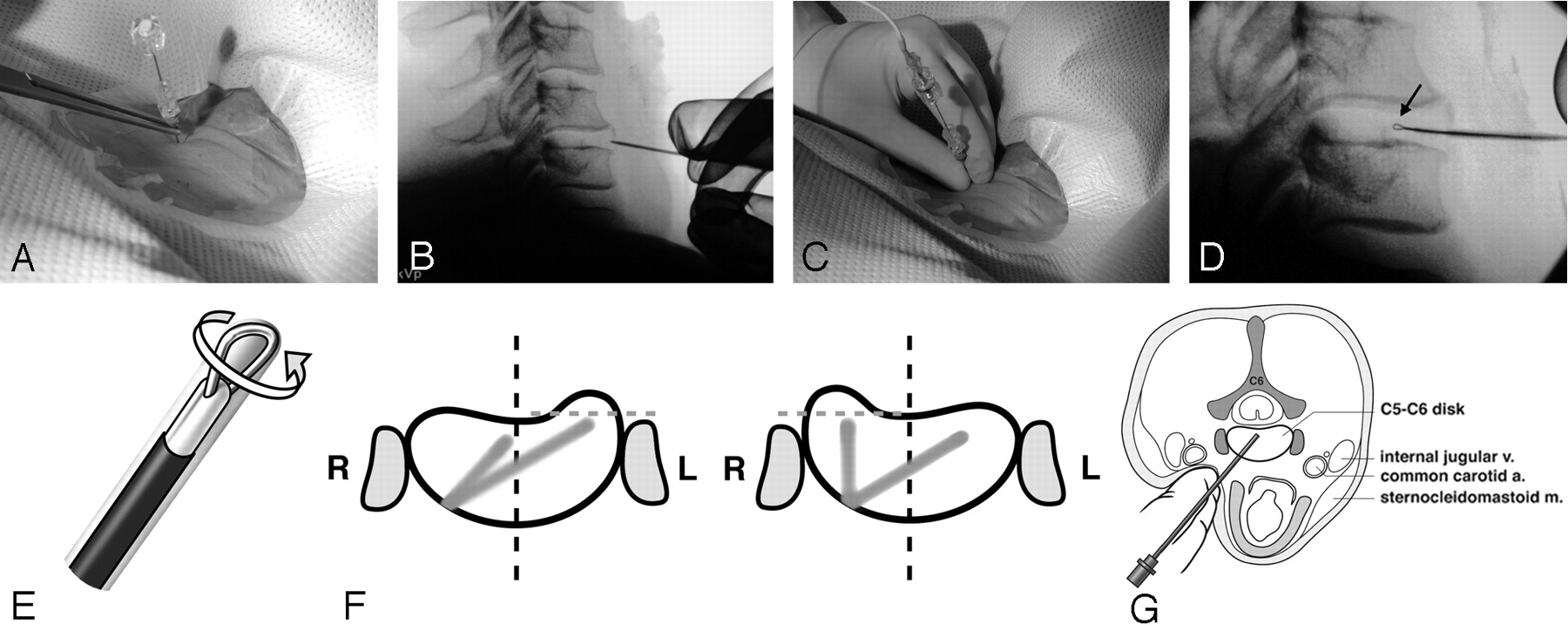
Patients received a prophylactic intramuscular injection of 1.5 g of cephalosporin 1 hour before we conducted the procedure. The procedure was performed under fluoroscopy by using a C-arm unit, with the patient placed in supine position. Patients received light sedation as necessary. The plasma diskectomy procedure was performed by using an anterior approach, in similar fashion to that described for a previous prospective series of patients by using the Nucleotome procedure.6 The head and neck were slightly hyperextended to facilitate access to the cervical disks. For better visualization of the lower cervical disks, it was beneficial to stabilize the shoulders. In these patients, traction was achieved by tying a belt to the patient’s wrists, and the belt was fixed to the end of the table near the patient’s feet. The entry point for the port cannula was placed off-midline toward the patient’s right side to make an anterolateral approach. Local anesthetic was administered by using a 22-gauge needle, inserted as deep as the annulus fibrosus; the anesthetic needle was positioned by using an extended holder to reduce x-ray exposure to the surgeon’s hands. While palpating vital structures away from the surgical pathway (the trachea was pushed across the midline, while the neurovascular bundle, the carotid artery in particular, and sternocleidomastoid muscle were maneuvered laterally and protected manually), we positioned a 19-gauge cannula with an internal mandrel against the anterior surface of the annulus fibrosus (Fig 1). Because the esophagus resides to the left of the midline, a relatively more right-sided approach was deemed safer at the more caudal cervical levels. The C-arm was positioned to gain a lateral view of the surgical field, and the cannula and mandrel were advanced under fluoroscopic guidance into the disk. The mandrel was replaced with the Perc-DC SpineWand (ArthroCare).
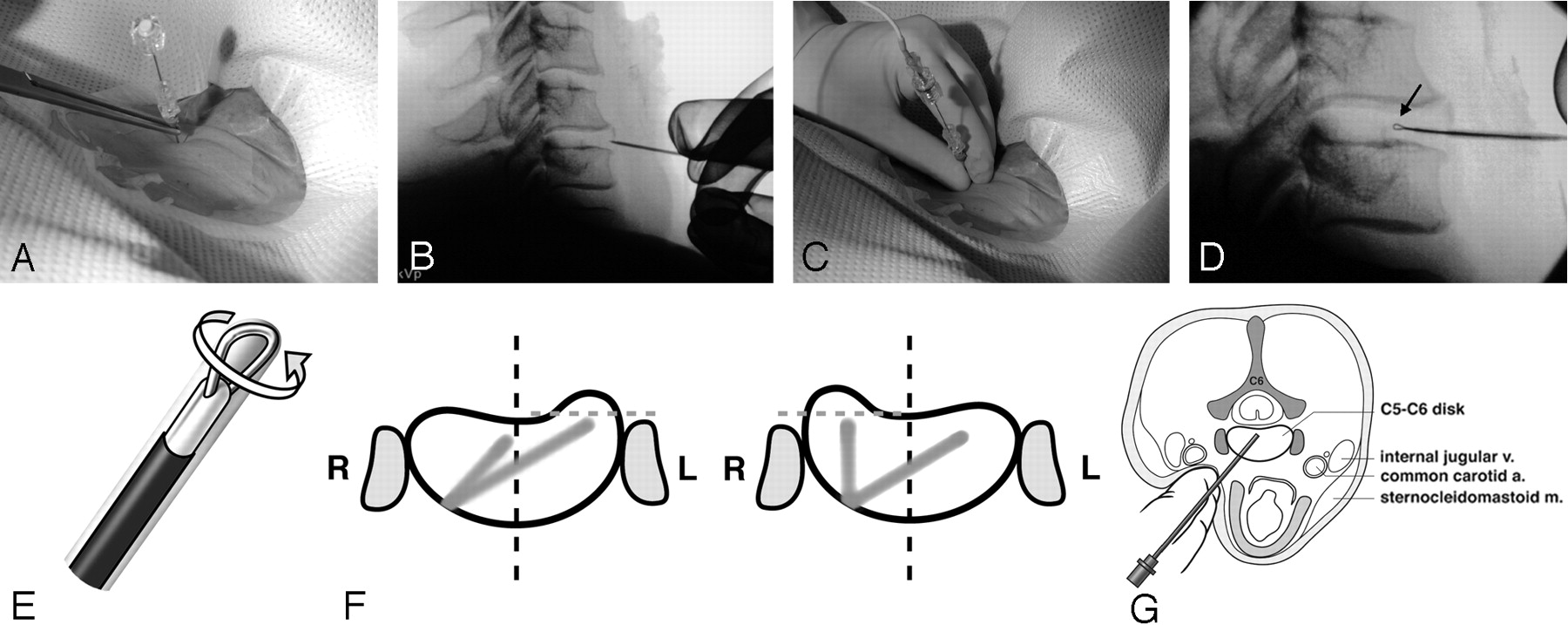
A, The 19-gauge cannula with an internal mandrel is positioned against the anterior surface of the annulus fibrosus. The cannula is held by a surgical forceps to minimize x-ray exposure of the surgeon’s hand.
B, Cannula placement as observed under fluoroscopy.
C and D, The cannula is advanced into the disk, and the SpineWand device (D, arrow) is introduced into the nucleus pulposus via the cannula.
E, The device is activated and then rotated 360°(E) to create a spheric void by means of the loop-shaped active electrode (arrow). Between 2 and 4 voids are ablated in a linear direction to create a channel.
F, After the first channel into the disk is completed, the device is repositioned to a different part of the nucleus, with the placement depending on the topography of the herniation. For left-sided herniations, the first channel is made in an oblique direction, from the right anterolateral entry point toward the left posterolateral herniation; the other channel is made on the midline and directed toward the posterior profile of the disk. For a right-sided lesion, the first channel is directed obliquely toward the center of the disk; the second channel is directed toward the right paramedian, along the medial surface of the uncal process to reach the herniation in the posterior aspect of the disk.
G, A schematic drawing shows the entry route, with the clinician’s fingers pushing the trachea across the midline while protecting the neurovascular bundle.
With the radio-frequency controller set at 3′ (approximately 150 volts rms), the SpineWand device was activated and then rotated 360° to create a spheric void. The selected controller setting was that specified by the manufacturer as the most efficient for producing a plasma field in this application. The plasma radio-frequency–based process removes a small amount of tissue within the nucleus pulposus to achieve disk decompression. After 8 seconds of ablation, the device was repositioned to a different part of the nucleus, with the placement depending on the topography of the herniation. For both left- and right-sided lesions, voids were created along 2 channels. On the left side, the first channel was made in an oblique direction, from the right anterolateral entry point toward the left posterolateral herniation; the other channel was made on the midline and directed toward the posterior profile of the disk. For a right-sided lesion, the first channel was directed obliquely toward the left, crossing the center of the disk; the second channel was directed toward the right paramedian, along the medial surface of the uncal process to reach the herniation in the posterior aspect of the disk. With these maneuvers, a total of 4–8 voids (2–4 voids to make each channel) were made in the nucleus pulposus. After completing the ablation procedure, we withdrew the SpineWand from the disk and removed the wand and cannula simultaneously from the surgical port. The ablation portion of the procedure took less than 5–8 minutes for a single disk level.
Postoperative Care
A prophylactic intramuscular injection of 1.5 g of cephalosporin was also administered 8 hours following the procedure. In contrast to standard practice when performing plasma radio-frequency–based diskectomy in the lumbar spine, steroids were not injected into any of the treated or adjacent disks. The procedure was typically performed on an outpatient basis, though some of the patients from more-distant homes stayed overnight in the hospital for convenience.
When discharged, patients received a prescription for a nonsteroidal analgesic anti-inflammatory drug (to be taken for 7–10 days) and for a rigid neck collar, recommended to be used during the daytime for 2 weeks.
Outcome Measures
Because this was a general outcomes research study, we did not modify normal practice in the clinic. Success of the procedure was mainly based on clinical evaluation. Clinical outcome for each patient was defined as excellent, good, fair, no improvement, or worse, according to modified Macnab criteria (Table 1). In the patients with preoperative clinical and morphologic cord compression, regression of myelopathy symptoms had to be obtained, as well, for outcomes to be determined as good or excellent.
Modified Macnab criteria used to grade overall clinical outcome
Postoperative clinical follow-up also included a neurologic examination. Follow-up MR imaging studies were not performed in all patients, but only when clinically indicated. Consequently, MR imaging was collected from 15/55 (27%) patients following the intervention.
Results
The procedure was successfully completed in every case (N = 55), with very little discomfort for the patient. Thirty-six patients received treatment at 1 level, 18 patients were treated at 2 levels, and 1 patient was treated at 3 levels. In patients with a single level, it took no more than 10–12 minutes from the time the local anesthetic was applied to withdrawal of the SpineWand. Disk herniations were encountered in our series only at 3 disk levels, including C4–5 (n = 5), C5–6 (n = 37), and C6–7 (n = 33). Because pathology was limited to these 3 levels, we have no experience accessing or treating other levels in the cervical spine. At all attempted levels, the procedure was completed successfully.
In our first patient, we experienced a device-related technical complication. While the surgeon withdrew the device from the cannula, after completing the ablation portion of the procedure, the distal loop electrode detached from the tip of the device and remained in the disk space (note that the tip is made of titanium, which is biocompatible). The patient, who was informed of the event, remained completely asymptomatic and had excellent clinical results during the past 29 months of follow-up.
One clinically relevant procedure-related postoperative complication, a case of infectious diskitis, was observed. The patient presented with fever and persisting neck pain 3 weeks after the procedure. MR imaging suggested evidence of diskitis. A tissue biopsy showed positive findings of Staphylococcus organisms and gram-negative bacteria. The patient was treated successfully by using a standard antibiotic regimen and rigid collar therapy. Symptoms of general infection were resolved by 8 weeks following initiation of therapy, and an 8-month follow-up MR imaging study showed regression of aspects of disk infection (hyperT2 signal intensity and contrast enhancement of adjacent vertebral bodies). However, the patient still had neck pain, and consequently, the clinical outcome was graded as poor.
In a few patients, we observed local-anesthetic–related side effects, which in all patients regressed within the first few hours. The first patient had bradycardia, which was attributed to the effect of the anesthetic on the carotid glomus. Two patients showed evidence of Horner syndrome, attributed to the effect of anesthetic on the cervical sympathetic chain. A fourth patient had a bitonal voice, thought to be a result of the effect of the anesthetic on the inferior laryngeal nerve.
At present, the follow-up period extends from 2 to 29 months. All patients were followed up for at least 2 months; results were considered excellent or good in 25 and 19 patients (80%), respectively (Table 2). The success rate remained similar at 6 months (44/52, 85%).
Clinical outcomes according to the modified Macnab criteria at months 2 and 6
All patients who had good or excellent results at 2 months responded fairly quickly following the procedure. All patients reporting a good or excellent regression of pain, with consequent definite improvement of quality of life (all graded 3 or 4), also showed a complete or partial regression of the radicular deficits (hyposthenia and/or hypoesthesia). In no patient was a residual deficit disturbing enough to require CT or MR imaging or to pursue treatment options other than mild physiotherapy. Three patients reported relief of upper limb pain and paresthesias during the intervention itself (while the voids were being created inside the disk). Most patients reported a significant improvement of symptoms the day after the procedure, though in a few patients noticeable improvement required between 2 and 4 weeks’ recovery. Regression of clinical myelopathy symptoms related to compression of the spinal cord was observed in all 3 patients who had symptoms.
Of those followed up for at least 6 months, 5/52 patients (10%) never showed any clinical improvement; 3 have been followed up for longer than 24 months, 1 for longer than 12 months, and 1 for longer than 6 months. Of the failed group, 1 was the patient who had received percutaneous diskectomy at 3 levels simultaneously and another was the patient who experienced the diskitis-related complication. In the patient who was treated at 3 levels, we observed a transitory mild side effect, with no notable clinically relevant consequences. For 3–4 days following the procedure, the patient had intense retrosternal and retrolaryngeal pain. A CT scan performed the day after the procedure showed evidence of edema, with a possible mild hemorrhagic infarction of the prevertebral soft tissues. This new (unusual to the patient) postoperative pain was transient and resolved completely with medical treatment.
Fifteen patients had an MR imaging study between 2 months and 1 year after the intervention. In 6 patients, including 2 of the 3 patients with spinal cord compression, the postoperative MR imaging (at 2-, 3-, 4-, 8-, 8-, and 9-month follow-up) showed regression of the soft disk herniation (Table 3). Five of these patients, including the 2 with cord compression (Fig 2), had a good or excellent clinical outcomes (Macnab grade 3 or 4), whereas 1 had a poor clinical outcome (Macnab grade 1). Of the remaining patients, 1 was the patient with the diskitis complication, whereas 8 showed no modification of the disk herniation after the procedure (at 2-, 2-, 2-, 2-, 4-, 6-, 6-, and 12-month follow-up). Among the latter 8 patients, 3 had a poor clinical follow-up (Macnab grade 1), whereas 5 had a good or excellent clinical result (Macnab grade 3 or 4). No association was detected between selected demographic characteristics and treatment success, with the possible exception of a type of associated pathology (Table 4).

A, MR imaging at baseline for a 34-year-old woman who underwent percutaneous plasma radio-frequency–based diskectomy for a disk (C6–7) herniation compressing the spinal cord and causing clinical signs of myelopathy.
B, A 7-week MR imaging follow-up shows regression of both herniation and cord compression; the patient is almost asymptomatic.
C, An MR image at 9-month follow-up shows almost complete regression of the disk herniation; the patient is completely asymptomatic.
Regression of disk herniation findings in patients who underwent postoperative MR imaging (n = 15)
Outcomes at month 2 stratified by selected demographic characteristics
Discussion
Our preliminary experience with percutaneous plasma radio-frequency–based diskectomy for treating cervical disk–contained herniation was favorable. We found that the procedure took no more than 10–12 minutes to complete (in single-level cases), from administration of the local anesthetic to withdrawal of the SpineWand, and was minimally traumatic to the patient. The patient remained fully awake, in most cases even mild sedation was not necessary, and patient discomfort was minimal. The instrumentation was much less bulky than that used during our previous experience with the Nucleotome procedure in 84 patients treated between 1990 and 2002.6 Of note, with that technique, general anesthesia or heavy sedation was always necessary.
The introducer cannula for the SpineWand device has a 19-gauge caliber, which is smaller than the needles currently used for direct puncture of the carotid artery or for diagnostic and interventional angiography. In contrast, the 2-mm cannula for introducing the aspiration probe into the disk space is more aggressive. In 1 patient during the Nucleotome procedure series, we reported a cervical hematoma resulting from an injury to the inferior thyroidal artery, which required surgical evacuation.6 The 19-gauge cannula for the SpineWand device is easily inserted by means of a coaxial mandrel with a trocar tip. This is an important safety feature. With the more bulky devices, it is necessary to use sharper bevel tips or cutting edges to open the path through the soft tissues to the disk. A trocar point does not have a sharp cutting effect, and structures are more likely to be deflected rather than resected. This feature limits the risk of vessel or nerve injuries. In addition, unlike bevels, the symmetric trocar point follows a straight trajectory, allowing more precise positioning easily, particularly when driving the instrument into a relatively rigid tissue structure like the annulus fibrosus. Nevertheless, a thorough knowledge of the anatomy of the underlying structures of the neck intersecting the treatment pathway and a good quality fluoroscopy system are mandatory.
The day before the procedure, we performed a preoperative sonographic study of the neck to determine whether any normal or pathologic structures residing near the surgical pathway were in a position to increase risk for complications.6,26,27 The only vital structures that cannot be manually displaced from the trajectory of the trocar are the thyroid, particularly its isthmus, and the inferior thyroidal artery. A 19-gauge puncture of the thyroid is of no clinical relevance, as confirmed by the wide experience in thyroid biopsies and carotid angiography. The inferior thyroidal artery, arising from the thyrocervical trunk of the subclavian artery, runs medially to reach the inferior pole of the thyroid gland and crosses the possible surgical trajectory to lower disks; however, it is our belief that the inferior thyroidal artery and the inferior laryngeal nerve are safeguarded by use of the trocar tip and small-gauge needle. This may not be the case when using larger sharper tip devices. We observed no complication associated with direct damage to neck tissues or structures.
Once inserted into the disk, the SpineWand was easily maneuvered under fluoroscopy. It can be moved easily in all directions to reach the protruding pathologically displaced portion of the nucleus pulposus. In this respect, the SpineWand seemed more mobile and effective than the Nucleotome aspiration probe.
One concern we had with this diskectomy technique was x-ray exposure to the surgeon’s hands. The left hand (of a right-handed surgeon) is directly exposed to the fluoroscopy x-ray central beam during the time it took (a few seconds) to shift the neurovascular bundle and trachea away from the treatment pathway when positioning the cannula; this is a necessary maneuver for ensuring patient safety. Although our standard practice is to wear lead gloves for protection, the gloves cannot completely arrest the x-ray central beam. Alternatively, the surgeon could choose to position the cannula under CT guidance and switch to direct fluoroscopy for the remainder of the procedure (Figs 3 and 4).
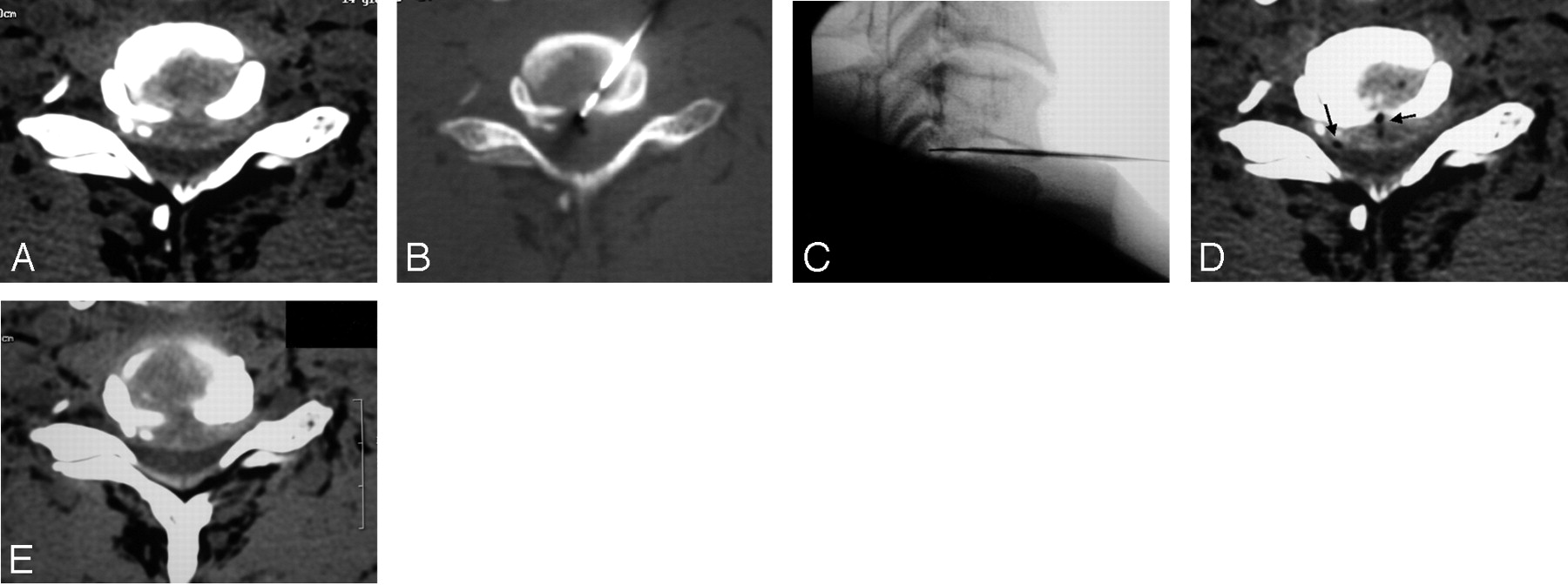
A, Bilateral disk herniation at C6–7 encroaching the spinal canal. The SpineWand device was placed into position by using CT-guidance and switching to direct fluoroscopy for the disk ablation procedure. This allowed activation of the plasma-field energy directly inside the herniation.
B and C, The loop-shaped active electrode was inserted beyond the posterior limit of the vertebral body into the spinal canal.
D, At the end of the procedure, the gas generated from the tissue excision is evident inside the disk.
E, The 5-month follow-up image shows only minimal or questionable reduction of disk size; despite this, the patient reports good clinical improvement (Macnab 3) (see text for discussion).

A, Lateral disk herniation compressing the nerve root.
B, The cannula and SpineWand device are positioned under CT guidance and then safely and precisely directed toward the herniation.
C, Note gas from tissue excision diffusing inside the herniation itself.
D, A 4-month CT follow-up shows partial regression of the lesion; the patient reports a definite clinical improvement (Macnab 3).
We observed excellent or good results in 44 of 52 patients (85%) who were followed up for at least 6 months. Only 5 of these 52 patients never demonstrated any improvement, including the patient who had diskitis as a complication. These are very good results for a percutaneous intradiskal treatment for contained-disk herniation, and these seem to be better than the results usually reported for similar treatment at the lumbar levels.28,29
Because this was a general outcomes research project, we did not modify our current practice. Therefore, we did not perform follow-up MR imaging unless it was clinically indicated. Fifteen patients had an MR imaging study from 2 months to 1 year after the intervention. Eight patients of the 15 did not show any modification of the treated soft disk herniation. Despite this observation, only 3 had a poor clinical outcome, whereas 5 had a good or excellent clinical result (Macnab grade 3 or 4). This suggests that intradiskal decompression treatments act more through a reduction of the pressure on the nervous tissue (nerve roots or spinal cord) rather than, or not always attributed to, a modification of the morphology of the disk. Clinical improvement despite an unobservable lack of volumetric modification of the disk is a common observation with percutaneous lumbar treatments for disk herniations. This finding may be a result of 1 or more pathogenic mechanisms, such as decompression of the nerve root itself, local circulatory improvement due to a reduction of pressure on the periradicular vessels, and elimination of leakage from the inner disk nuclear components that may be eliciting a periradicular inflammation. One patient among the 6 who showed a regression of the disk herniation on MR imaging after the procedure had no clinical improvement; this may be indicative of poor patient selection.
Early in our experience with the SpineWand device, we had a device-related complication due to an incorrect maneuver by the operator (G.B.), who did not realize under fluoroscopy that the distal loop had been bent ∼90° laterally during the procedure. The initial prototype devices had a weaker design than the current device, which was redesigned to prevent this problem. In our case, the tip of the device broke during withdrawal because of the high degree of friction against the edges of the cannula. The patient, who was informed of the complication, is currently completely asymptomatic and satisfied at 29-month follow-up.
In the patient who was treated at 3 levels simultaneously and reported pain during the first few days postoperatively, we thought that the postoperative pain was not related to the device itself but that the 3-level simultaneous approach was probably too aggressive for the prevertebral soft tissues. In reality, this patient was not a good candidate for percutaneous diskectomy: this intervention was principally attempted with the aim of sparing the patient a more aggressive multilevel open-fusion surgery, which the patient continues to refuse.
The reasons percutaneous intradiskal treatment may be more effective at the cervical level than at the lumbar level are not clear. One explanation could be anatomic. The cervical root is confined to a smaller space than its lumbar counterpart. For this reason, the cervical root is more sensitive (ie, more prone to induce symptoms) to even a small amount of compression. Consequently, even a small reduction in the volume of the disk, such as that usually obtained with an intradiskal treatment, may result in root decompression and consequent clinical amelioration. In contrast, a relatively larger herniation is necessary to induce symptoms at lumbar levels; a large herniation is more difficult to treat by using percutaneous intradiskal decompression. At the cervical level, a small focal protrusion can produce marked symptoms, but such a condition can be more easily treated percutaneously. For the same reason, we observed better results in percutaneous lumbar treatments for disk herniations in some subgroups of patients, such as patients previously having undergone surgery (root confined to a smaller space because of scarring) and elderly patients (root confined to a smaller space because of osteophytes).30 Another explanation could be related to the topography of the lesion and direction from which it is approached for treatment. For treatment of cervical herniations, a percutaneous procedure is performed from an anteroposterior direction, whereas in the lumbar spine, the approach is performed from the posterolateral direction. Because a symptomatic herniation is directed posteriorly (both at cervical and lumbar levels), it is much more easily reached from an anterior approach. This difference in approach between the cervical and lumbar spine may affect success rates of the 2 procedures.
Ongoing experimental, theoretic, and modeling research is leading to improved understanding of the varied and complex mechanisms involved in the plasma-mediated radio-frequency–based tissue removal process. For example, from an analysis of the light emitted from the plasma field, it is known that water molecules (which compose a significant fraction of most types of tissue) can be fragmented into excited and ground-state hydroxyl radicals and hydrogen atoms. Both of these species are chemically active and can cleave long chain molecules (eg, collagen) into smaller fragments that are either more easily liquified or gasified.19 Moreover, electrons emitted from the electrodes at the distal end of the device when the voltage is applied can develop sufficiently high energies not only to cause the water molecules to fragment but also to directly dissociate the chemical bonds in the nearby targeted tissue structures (in this case disk tissue) into smaller fragments that are subsequently removed.
In follow-up studies, we found positive MR imaging findings in 2 patients who were asymptomatic 2 months and 1 year, respectively, after the plasma radio-frequency–based diskectomy (Fig 5). It is our opinion that hypo-T1, hyper-T2 modifications of the adjacent vertebral bodies are an expression of an inflammatory condition. We speculate that an inflammatory intradiskal process could be part of healing after the procedure. Disk herniations are known to have a tendency to self-heal. Spontaneous regression of herniated lumbar disks in the lumbar region is well established,31,32 but the same phenomenon is increasingly observed in cervical disks as well.33–36 Spontaneous resorption of lumbar herniated nucleus pulposus is thought to occur more frequently in uncontained rather than contained lesions, because it appears that it is the presence of nucleus material in the epidural space that primes the foreign body inflammatory reaction associated with neovascularization, thought to be related to the healing process.37–41

A and B, The C6–7 disk before undergoing the ablation procedure because of a mostly lateral left intraforaminal herniation (A) with the associated mild central protrusion shown in a sagittal MR image (B).
C and D, MR imaging follow-up at 2 months shows hypo-T1, hyper-T2 modifications of the adjacent vertebral bodies and evidence of an inflammatory condition.
E, Partial reduction of the herniation is observed at the 2-month follow-up. The patient is completely asymptomatic despite only partial reduction of the disk herniation (see text for discussion).
On the contrary, in the cervical disk inflammatory reaction, immunoreactivity and neovascularization are also present in contained-type hernias.36,42 This is probably related to detachment of the cartilaginous vertebral endplate associated with cervical herniations, as observed both in cadavers and in vivo,43 where the detachment promotes neovascularization, and consequently the other related phenomena, from the denuded highly vascularized somatic bone. Alterations in cytokine expression potentially associated with the mechanism of pain relief have been observed after plasma radio-frequency–based diskectomy.44 We could speculate that a self-healing inflammatory response, never observed after mechanical nucleotomy in our experience, could be stimulated by the plasma radio-frequency–based treatment, similar to that proposed with treatment of other chronic pathology.45 This hypothesis may be worthy of more rigorous research. We are following up this finding with further MR imaging studies in additional asymptomatic patients after percutaneous plasma radio-frequency–based diskectomy.
Conclusion
The natural history of symptomatic cervical disk herniation suggests that spontaneous healing may occur: even patients who have a soft disk herniation causing a cervical myelopathy have been treated conservatively with good results.46 Thus, among options for patients with symptomatic cervical disk herniation, the presented treatments must have a low morbidity rate. In this respect, in our preliminary experience, use of percutaneous plasma diskectomy for treatment of this pathologic condition seems encouraging, thanks to the very low morbidity and the good clinical results that are achieved early on following the procedure. Because of its minimally invasive nature, this technique, in our opinion, could be justified as a means to shorten the painful incapacitating period of a disease that has a favorable longer term natural history for spontaneous resolution.
Acknowledgments
The authors thank Debby Holmes-Higgin, MS, MPH, and Kenneth R. Stalder, PhD, for technical contributions to the manuscript.
Footnotes
Presented in part at: Annual Symposium of the American Society of Spine Radiology, February 2004, Miami, Fla.
References
- Received August 12, 2005.
- Accepted after revision February 1, 2006.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.