
Abstract
SUMMARY: Chondrosarcoma of the hyoid bone is rare. Only 14 cases have been reported in the literature, to date. We present a case of chondrosarcoma of the hyoid bone with imaging, surgical, and pathologic correlation, and a review of the literature.
Chondrosarcomas constitute approximately 11% of all primary bone tumors.1 Although it is the third-most-common primary malignant bone tumor (following osteosarcoma and multiple myeloma)2 and the second-most-common sarcoma arising in bone,1 most cases occur in the pelvic bones, proximal femur, proximal humerus, distal femur, and the ribs. Less frequently (range, 1%–12%)1 chondrosarcoma originates in the head and neck region, with the skull base, maxilla, and larynx more commonly involved.
Case Report
A 30-year-old woman presented with a painless, nontender, hard, fixed 7-cm submental mass that had increased in size over a 7-month period and had no signs of inflammation.
Ultrasonography demonstrated a well-circumscribed solid submental mass with calcifications (Fig 1).

An inhomogeneous solid echoic mass within the submental area, slightly more prominent on the left side.
The CT scan revealed a heterogeneous mass at the level of, and replacing, the body of the hyoid bone, which was expanded to the left lesser cornu (hyoid bone consists of 5 segments: a body, 2 greater cornua and 2 lesser cornua). The location of the mass just inferior to the floor of the mouth, with peripheral rim calcification and internal chondroid calcification, suggested a cartilaginous tumor of the hyoid (Fig 2).
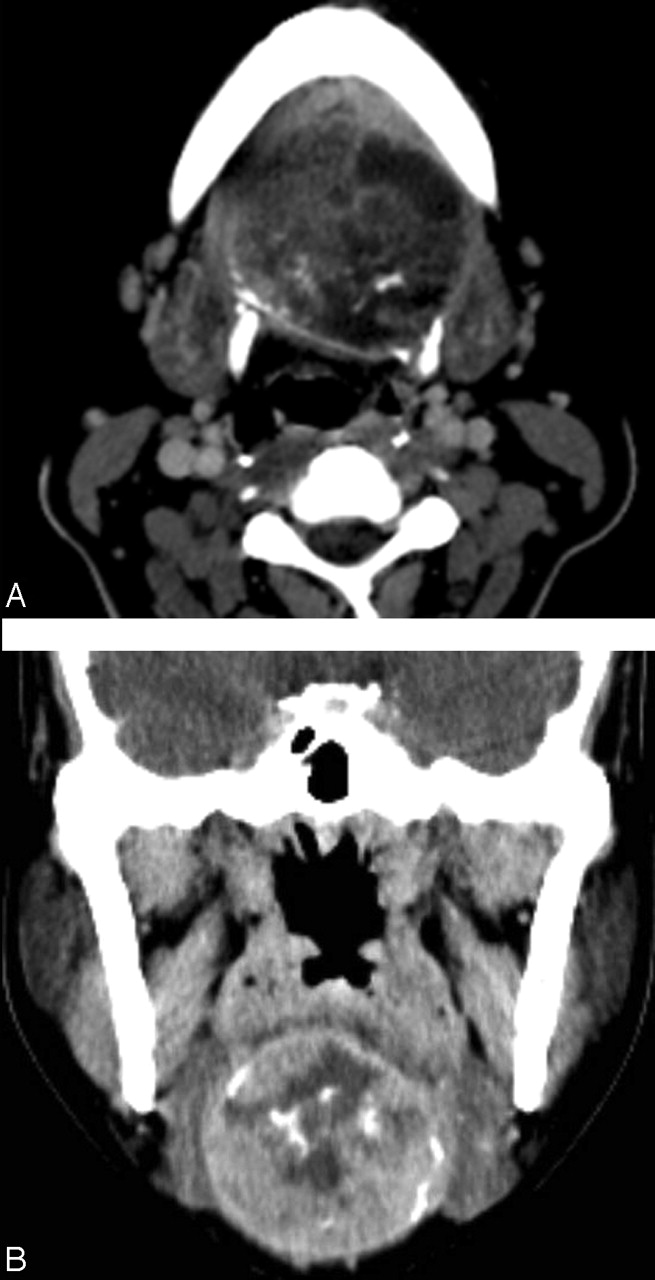
A, Contrast-enhanced axial CT scan at the level of hyoid bone revealed a well- defined mixed attenuation mass that has expanded to the left lesser cornu and has replaced the normal body of the hyoid bone with peripheral rim calcification and internal chondroid calcification. The right lesser cornu cannot be demonstrated.
B, Contrast-enhanced coronal CT scan revealed a round well-defined inhomogeneous attenuation mass with peripheral rim calcification and internal chondroid calcification below the floor of the mouth.
The operative finding revealed a well-capsulated mass originating form the hyoid bone (Fig 3). The mass adhered to the submandibular glands, strap, and mylohyoid muscles, but without definite invasion.

A, The surgical specimen revealed a well-defined, almost-round mass originated from the body, both lesser cornua of the hyoid bone, more prominent on the left side The appearance was concordant with the CT finding.
B, The cut surface of the resected specimen revealed an encapsulated firm, gray-white tissue tumor measuring 7 cm in diameter.
Histopathologically, the neoplasm was composed of mature chondrocytes with minimal nuclear and cytoplasmic atypia compatible with grade I chondrosarcoma (Fig 4, Table).3

Histopathology revealed grade 1 chondrosarcoma seen as mature chondrocytes with minimal nuclear and cytoplasmic atypia.
Discussion
The diagnosis of a chondrosarcoma of the hyoid bone may be missed because of its infrequent occurrence. Solid primary lesions of the hyoid bone are exceedingly rare and the reported cases have included plasmacytoma, osteosarcoma, giant cell tumor, aneurysmal bone cysts, osteoma, chondroma, and chondrosarcoma.3–11 Only 14 cases of chondrosarcoma of the hyoid bone have been reported in the literature.3,12–21
Chondrosarcoma may involve any part of the hyoid bone. Involvement of the body, greater or lesser cornus have already been reported in the literature.3,12–21 The size of the lesions varied from 0.5 cm to 7 cm. The age of patients also varied between 30 and 82 years (average age, 51.69 years).
Ultrasonography can help determine the texture of the mass, but often not the site of the origin. The common associated calcifications may be detected by ultrasonography, but not as well as with a CT scan. It was difficult and may be impossible to suggest the correct diagnosis by sonography.
A CT scan is the imaging technique of choice because it can better clarify a tumor’s extension and origin. The location beneath the mylohyoid muscles and the expansion of the hyoid bone with chondroid calcification should suggest the correct diagnosis. Approximately 75% of chondrosarcomas will demonstrate intrinsic calcification.3,17 The multiplanar capabilities and better tissue contrast of MR imaging can more precisely define the extension of the tumor and its relationship to surrounding structures and aid in planning the surgical approach.17 Chondrosarcoma appears as an inhomogeneous area of low signal intensity on a T1-weighted image and a more inhomogenous mixed high–low signal intensity on T2-weighted image. The calcifications revealed as areas of signal intensity void.3,12 A strongly enhancing mosaic appearance within the high-signal-intensity area on T2-weighted image may be an important diagnostic clue for chondrosarcoma of the hyoid bone; however, osteogenic tumor and aneurysmal bone cysts may have a similar MR imaging appearance.12
It is very difficult and may be impossible to distinguish chondroma from low-grade chondrosarcoma radiographically.2,3,22 Rare cases of chondroma have been reported.23–26 Geirnaerdt et al27 reported that fast contrast-enhanced MR imaging may assist in differentiation between benign and malignant cartilaginous tumors. Early enhancement was seen in chondrosarcoma, not seen in chondroma, and seen in osteochondroma only when growth plates were unfused. Pathologic differentiation between low-grade chondrosarcoma and chondroma can be also very difficult. Higher-grade chondrosarcomas have an increased cellularity, more nuclear pleomorphism, and identifiable mitotic figures.
Chrondrosarcoma can be histologically graded from 1 to 3 on the basis of the mitotic rate, cellularity, and nuclear size (Table).28
Surgical excision is the treatment of choice for chondrosarcoma. Neither radiation therapy nor chemotherapy plays a significant role in either primary or adjuvant treatment. Chondrosarcoma is radioresistant, though a trial of radiation therapy may be considered for patients who decline or are not surgical candidates.12,17
The hyoid bone is the insertion of the musculature of the tongue and also is attached to the thyroid cartilage via the thyrohyoid membrane and the extrinsic muscles of the larynx. Total hyoidectomy to completely excise the tumor may cause abnormal phonation and difficulties in swallowing and respiration. Our patient, however, did not have any abnormal symptoms and was able to return to her normal life and work.
References
- Received November 16, 2004.
- Accepted after revision February 24, 2005.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}