
Abstract
BACKGROUND AND PURPOSE: This study examines whether anatomic extent of pial collateral formation documented on angiography during acute thromboembolic stroke predicts clinical outcome and infarct volume following intra-arterial thrombolysis, compared with other predictive factors.
METHODS: Angiograms, CT scans, and clinical information were retrospectively reviewed in 65 consecutive patients who underwent thrombolysis for acute ischemic stroke. Clinical data included age, sex, time to treatment, National Institutes of Health Stroke Scale (NIHSS) score on presentation of symptoms, NIHSS score at the time of hospital discharge, and modified Rankin scale score at time of hospital discharge. Site of occlusion, scoring of anatomic extent of pial collaterals before thrombolysis, and recanalization (complete, partial, or no recanalization) were determined on angiography. Infarct volume was measured on CT scans performed 24–48 hours after treatment.
RESULTS: Fifty-three patients (82%) qualified for review. Both infarct volume and discharge modified Rankin scale scores were significantly lower for patients with better pial collateral scores than those with worse pial collateral scores, regardless of whether they had complete (P < .0001) or partial (P = .0095) recanalization. Adjusting for other factors, regression analysis models indicate that the infarct volume was significantly larger (P < .0001) and modified discharge Rankin scale score and discharge NIHSS score significantly higher for patients with worse pial collateral scores. Similarly, adjusting for other factors, the infarct volume was significantly lower (P = .0006) for patients with complete recanalization than patients with partial or no recanalization.
CONCLUSIONS: Evaluation of pial collateral formation before thrombolytic treatment can predict infarct volume and clinical outcome for patients with acute stroke undergoing thrombolysis independent of other predictive factors. Thrombolytic treatment appears to have a greater clinical impact in those patients with better pial collateral formation.
Immediately following ischemic stroke, thrombolytic therapy has the potential to rescue brain tissue that exists within a poorly perfused ischemic penumbra surrounding infarcted brain (1–7). Diffusion/perfusion MR imaging, CT perfusion, CT angiography, and single-photon-emission CT (SPECT) have been used to assess this ischemic penumbra. The degree of cerebral blood flow and perfusion as defined on perfusion MR imaging and CT have been linked to clinical outcome. These methods for evaluating the ischemic penumbra are not always available in a timely fashion. Studies of collaterals have shown to have a correlation with outcome similar to the blood flow studies.
In general, collateral blood supply to the brain following vessel occlusion may occur through large vessels found at the circle of Willis or via connections found between small pial vessels found along the surface of the brain. Pial collaterals always exist anatomically as artery to artery connections between different arterial watersheds. They become invoked instantly whenever a major occlusion provides a great difference of source of perfusion to a territory with blood moving along pre-existing connections to fill in the affected territory. The formation of “good” collaterals as seen on cerebral angiography is recognized to influence clinical outcomes and infarct volume following ischemic stroke (3, 4, 7–19). In fact, extent of collateral formation has recently been shown to be correlated to infarct volume during acute stroke (8). Although clinical scales are available, a reproducible method to identify the anatomic extent of pial collateral formation on angiography and define poor versus good collaterals during acute ischemic stroke is not currently available. The studies referred to above define pial collaterals in a subjective manner. One of the unique features of this study is that it attempts to define pial collateral formation in a simple and reproducible fashion in terms of anatomic extent, to help predict outcomes following thrombolytic treatment. Also, patients with complete recanalization have been shown to have significantly better outcomes than patients with no recanalization, and infarct volume was smaller for the recanalization group, which suggests that reconstitution of blood flow can also predict outcome (20).
Because cerebral angiographic evaluation is always performed before intra-arterial thrombolysis and demonstrates arterial blood vessel opacification with contrast in a temporal fashion, this work endeavors to determine whether the evaluation of the anatomic extent of pial collaterals on angiography during acute ischemic stroke can consistently and reproducibly predict infarct volume and clinical outcome relative to other predictive factors, such as age, site of occlusion, time to treatment, and recanalization. Such information can be useful when devising an angiographic grading scheme predictive of patient outcomes following thrombolysis and may help assess the potential benefits of successful thrombolytic treatment.
Patients and Techniques
Clinical information, arteriograms, and CT scans collected prospectively from 65 consecutive patients who underwent intra-arterial thrombolysis between November 1994 and April 2002 at the Ohio State University Medical Center were retrospectively reviewed to determine the extent of pial collateral formation and infarct volume. Patients gave written informed consent as part of a protocol that included screening angiography and thrombolytic treatment. The protocol was reviewed and approved by the Ohio State University Hospital Institutional Human Subjects Review Board, and the procedures followed were in accordance with institutional guidelines. Patients who were seen within 6 hours of symptoms of a carotid or vertebral basilar stroke and were considered thrombolytic candidates according to clinical, laboratory, CT, and angiographic criteria similar to PROACT underwent screening cerebral angiography (4). Unlike the PROACT study, the present study also included patients with ischemic stroke involving territories other than the middle cerebral artery (MCA), and patients >85 years of age. All patients seen between 0 and 3 hours were offered intravenous tissue plasminogen activator (tPA) as an alternative. Presentation and discharge National Institutes of Health Stroke Scale (NIHSS) score, discharge modified Rankin scale score, times from symptom onset until cerebral angiography, and demographic information were recorded. Some patients who met inclusion and exclusion criteria before angiography did not receive treatment either because the angiogram was negative or their symptoms resolved in the interim between clinical assessment and angiography.
Additional exclusion criteria for retrospective review of angiographic data included the following:
Posttreatment cross-sectional imaging study of the brain was not available.
Angiographic evaluation for pial collateral pathways did not include a delayed venous phase.
The internal carotid artery (ICA) was occluded and there was antegrade filling of the M1 segment via either posterior communicating artery (PCOMA), ophthalmic artery or anterior communicating artery (ACOMA) without anterior cerebral artery (ACA) or MCA occlusion or these pathways were not evaluated. Only patients whose collateral blood flow depended on pial vessels were studied.
A complication compromising pial collateral flow occurred such as extracranial dissection of the parent vessel or intraprocedural thromboembolic event.
Patients underwent angiography and thrombolytic treatment by using local anesthesia, aseptic technique, and digital fluoroscopic control in a biplanar angiographic suite. Sedatives were avoided where possible. Methods of thrombolytic therapy for patients included continuous infusion or pulse spray. Microcatheter positioning relative to the thrombus was determined by the operator but was typically in the thrombus. Mechanical methods for clot disruption such as balloon angioplasty or clot retrieval were not used. Thrombolytic agents infused in this study included urokinase (up to one million units), recombinant prourokinase (up to 6 mg), and tPA (up to 90 mg). Other end points for thrombolytic administration included: onset of intracranial hemorrhage, and recanalization or physician to terminate the procedure because of technical difficulties for further treatment or technical complication.
Angiograms of all patients were reviewed by an interventional neuroradiologist (G.A.C.) who was blinded to all clinical information during this review. Occlusion site was scored as follows: occlusions at the internal carotid artery were assigned a score of 1; occlusions at the M1, P1, or A1 segment were assigned a score of 2; occlusions at the M2, A2, or P2 segments were assigned a score of 3; occlusions at the P3, M3, or A3 segment were assigned a score of 4; and more distal occlusions were assigned a score of 5. Cerebral arterial segments are defined elsewhere (13). Scores of 1 and 2 were considered proximal and scores 3–5 distal.
Complete recanalization was defined as no visible occlusion on angiography following thrombolysis. Partial recanalization included patients with branch occlusion following thrombolysis and reconstitution of flow in at least one branch. No recanalization included patients with lack of reconstitution in flow.
Evaluation of pial collateral formation was based on retrograde contrast opacification of vessels within the occluded territory on delayed angiographic images. Collaterals were scored (Fig 1) as follows:
A score of 1 was assigned if collaterals reconstituted the distal portion of the occluded vessel segment (ie, if there was M1 segment occlusion the M1 segment distal to the occlusion reconstituted; Fig 2).
A score of 2 was assigned if collaterals reconstituted vessels in the proximal portion of the segment adjacent to the occluded vessel (ie, if there was M1 segment occlusion with reconstitution to the proximal M2 vessel segments).
A score of 3 was assigned if collaterals reconstituted vessels in the distal portion of the segment adjacent to the occluded vessel (ie, if there was M1 segment occlusion with reconstitution to the distal portion of the M2 vessel segments).
A score of 4 was assigned if collaterals reconstituted vessels two segments distal to the occluded vessel (ie, if there was M1 segment occlusion with reconstitution up to the M3 segment branches).
A score of 5 was assigned if there was little or no significant reconstitution of the territory of the occluded vessel.
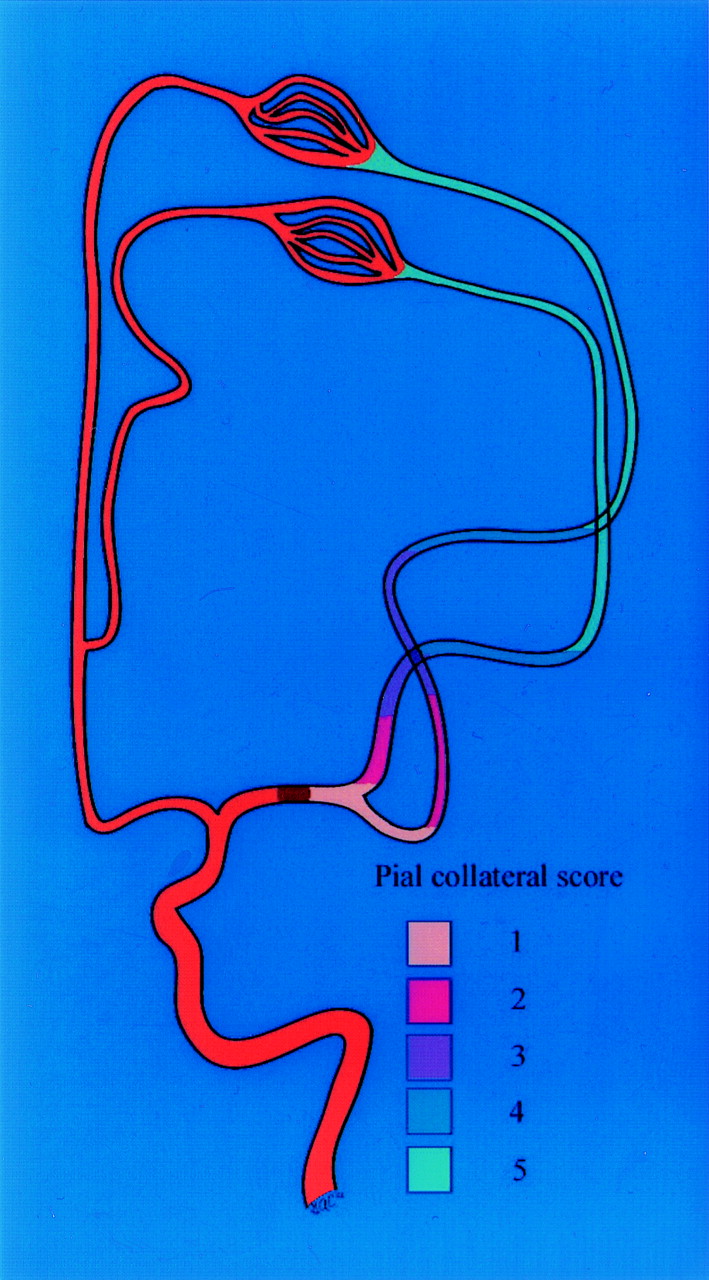
Scoring of the anatomic extent of pial collateral blood flow from the ACA territory to the MCA territory during occlusion of the M1 segment. Scoring corresponds to the angiographically visible retrograde reconstitution of the MCA segments on the delayed venous phase. Each color is depicts the furthest extent of retrograde opacification depicted on anteroposterior cerebral angiograms for each pial collateral score.

Anteroposterior (A and C) and lateral (B and C) images from a left internal carotid artery angiogram obtained during the early (A and B) and delayed angiographic phases (C and D) in a patient with acute ischemic stroke due to occlusion at the M1 segment (arrow). Note the retrograde opacification of the MCA branches via pial collateral vessels extending from the ACA (arrowheads). Because there is reverse opacification of the MCA extending to the distal M1 segment, a pial collateral formation score of 1 was assigned.
For occlusion sites at the ICA bifurcation, the occluded vessel segment was assumed to include the proximal M1 and A1 segments. Therefore, scoring here was similar to an M1 occlusion where a score of 1 is assigned if there was reconstitution of the distal M1 segment. There is no possibility to reconstitute the distal ICA in an ICA bifurcation occlusion.
Acute infarction on 24–48-hour CT was defined as a new hypoattenuated region relative to pretreatment CT. Infarcted regions were traced out on axial cross-sectional images by a CAQ (certificate of added qualification)–certified neuroradiologist (G.A.C.), and areas were calculated by using IMPAX image analysis software (Agfa Corporation, Ridgefield Park, NJ). Infarct volume was calculated by summing the cross-sectional areas multiplied by section thickness.
Pial collaterals were scored for all angiograms, and infarct volumes for the first 25 patients were determined at two different interpretation sessions spaced at least 30 days to test for reliability. Intraobserver agreement was calculated, and in cases of pial score disagreement a third review determined scoring. The interpreter was blinded to all clinical and CT data during the interpretation sessions.
Statistical analyses were performed by using JMP5 software (SAS Institute, Cary, NC). A discharge NIHSS score of 42 was assigned to patients who died. Contingency analysis with two-tail Fisher exact test was used to determine whether there was significant differences in NIHSS score between patients with higher versus lower pial collateral scores. A Wilcoxon rank sum test was used to determine whether there was a difference in infarct volume between patients who had complete recanalization versus no or partial recanalization, dependent upon pial collateral score and occlusion site. Significant differences in discharge modified Rankin scale score among patients with complete recanalization depending on whether they had higher versus lower pial collateral scores were determined with a contingency analysis by using a two-tail Fisher exact test. A similar analysis was also attempted for the group of patients with no or partial recanalization. Differences in infarct volume and pial collateral score relative to time to treatment were analyzed by using Wilcoxon rank sum test to determine whether time to treatment was dependent upon the outcomes of infarct volume and pial collateral score. The influence of age and sex on pial collateral formation was also analyzed with Wilcoxon rank sum test and a two-tail Fisher exact test, respectively. Linear regression analyses were performed separately by using infarct volume and then NIHSS score as the outcome variable. To facilitate linear regression analysis by using discharge NIHSS score, NIHSS score was considered a continuous variable. Clinical outcome at the time of discharge was also analyzed with a multivariate logistic regression analysis by using modified Rankin scale score as the outcome variable. For all regression analyses the variables included age, sex, side of infarction (left or right), time to treatment, presence of hemorrhage on 24–48-hour CT, occlusion site, pial collateral score, and recanalization. Backward selection was then performed. The regression analyses were repeated after rejecting the variables with estimates having a probability of proving the null hypothesis >0.1 based on the Wald test. First, the variable with the largest P value for the Wald test was removed from the model, and a regression was run on the remaining variables. Then, a likelihood ratio test was performed, and the smaller model was tested for predictive power. This was continued with all of the remaining variables with α ≥ 0.1, until the smallest model was determined. During backward selection interaction between variables was evaluated. For all regression analyses, lack of multicollinearity among the independent variables was confirmed by using simple χ2 tests.
Results
Of the initial 65 patients who underwent intra-arterial thrombolysis for acute thromboembolic ischemic stroke at our institution, 34 were given intra-arterial tPA, 28 urokinase, and three recombinant prourokinase. None of the patients chose to undergo intravenous tPA as an alternative to intra-arterial tPA. Twelve of 65 consecutive patients were excluded (five ICA, five MCA, one ACA, and one basilar artery). In four patients, no angiogram was available for review. There was ICA occlusion with antegrade filling of the MCA via the ACOMA and PCOMA in one patient, one patient had a technical complication (dissection of the vertebral artery), in three patients with ICA occlusion potential source of collateral formation via ACOMA or PCOMA was not evaluated, and in two patients delayed venous phase was not acquired. One patient with an angiogram had no CT available for review.
Fifty-three patients with both adequate angiographic data and infarct volume measurements available were entered into the study, 29 female and 24 male. The mean age was 65.5 years (σ [standard deviation] = 15.1 years; range, 33–90 years). Mean time to delivery of thrombolytic agent (symptom onset to initiation of thrombolytic agent delivery) was 262.2 minutes (σ = 89.5 minutes). Median NIHSS score at presentation was 16 (range, 4–30). Median NIHSS score at discharge was 10 (range, 0–31; four patients died). Median Rankin score before symptom onset was estimated to be 0 (range, 0–4); the median discharge Rankin score was 4 (range, 0–6). The mean infarct volume was 79.7 cm3 (σ = 103.8 cm3; range, 0–526.6 cm3).
Intraobserver difference in infarct volumes of 25 randomly selected patients was 7.8% (σ = 4.65%) with an intraobserver variation of 8.6%. Intraobserver assessment of pial collateral score was identical in 46 of 53 patients and different by 1 score point in seven patients (κ = 0.81; SE = 0.065).
Mean infarct volumes divided according to pial collateral score and recanalization are described in Table 1. It is clear that more favorable collateral scores resulted in lower infarct volumes. If one considers only the patients with no infarction, all had pial collateral scores of 1, despite no recanalization. It is also clear that infarct volumes were lower in patients with complete recanalization, regardless of pial collateral grades.
Infarct volumes (cm3) distributed according to pial collateral score and recanalization result
Median presentation NIHSS scores, discharge NIHSS scores, changes in NIHSS score, and discharge-modified Rankin scale scores relative to pial collateral score and recanalization rate are presented on Table 2. Significantly more patients had an NIHSS score <15 on presentation among the group with pial collateral score of 1 or 2 versus those with pial collateral scores of 3–5 (P = .0217; two-tail Fisher exact test). Complete recanalization is shown to be necessary for a better outcome, as seen in the 21 patients with no or partial recanalization with a pial collateral score of 1 or 2, all of whom had poor discharge scores. Among patients with complete recanalization, those who had a pial collateral score of 1 or 2 were more likely to have a discharge-modified Rankin score <3 compared with patients with pial collateral scores of 3–5 (P = .0131; two-tail Fisher exact test). No patients with pial collateral scores of 4 or 5 had modified discharge Rankin scores better than 4, regardless of recanalization. Infarct volumes were smaller in patients with better pial collateral scores (1 or 2) relative to those with poorer pial collateral scores (3–5) when occlusion site and recanalization rate were taken into account, as shown in Table 3.
Clinical outcome (presentation NIHSS, change in NIHSS, discharge NIHSS, and modified Rankin) distribution according to pial collateral score and recanalization
Infarct volume (cm3) distribution according to pial collateral score, occlusion site, and recanalization
Mean infarct volume for the 10 patients whose treatment began <200 minutes after symptom onset was 24.03 cm3 (σ = 28.4 cm3) compared with 92.6 cm3 (σ = 110.8 cm3) in the other 43 patients whose treatment began after 200 minutes (P = .0210; Wilcoxon rank sum test). Regression analyses, however, did not identify a statistically significant association (P > .05) between time to treatment and change infarct volume or clinical outcome when tested against other predictors of outcome, such as recanalization or pial collateral score.
Extent of pial collaterals increased linearly with age (P = .0214, Wilcoxon rank sums test). The mean age of those patients with pial collateral scores of 1 or 2 was 64.7 years (σ = 13.9), whereas the mean age of patients with pial collateral score of 3–5 was 67.2 years (σ = 17.6). This was not statistically significant (P = .33). Percentage of female sex increased from pial collateral grade 1 to 5 as follows: grade 1, 48.2%; grade 2, 55.6%; grade 3, 60.0%; grade 4, 66.7%; and grade 5, 75.0%. Women with pial collateral scores of 1 or 2 accounted for 50.0%, whereas female patients with pial collateral scores of 3–5 totaled 64.5%, which was not statistically significant (P = .38, two-tailed Fisher exact test). The average age was 65.5 years for women and 65.5 years for men, and the median presenting NIHSS scores were 16.0 for women and 11.0 for men.
Linear regression analysis for infarct volumes is shown in Table 4, and demonstrates that age per year, high collateral score, distal occlusion site, and complete recanalization are all significant predictors of infarct volume. Age per year and high collateral score (3–5) are shown to increase infarct volume, whereas distal occlusion site and complete recanalization decrease it significantly. Linear regression analysis also identified age, high pial collateral score, and complete recanalization as significant predictors of the outcome variable, discharge NIHSS, as seen in Table 5. Estimates indicated that high collateral score (3–5) increased discharge NIHSS score, whereas complete recanalization decreased discharge NIHSS score. Logistic regression analysis for poor outcome at the time of patient discharge on the basis of modified Rankin scale score >2 is presented in Table 6. Predictive factors for outcome, based on the modified Rankin score, are age per year, high collateral score, and complete recanalization. High collateral score and complete recanalization improves outcome, whereas age per year slightly worsens outcome.
Linear regression analysis model performed with significant predictive factors for infarct volume (age per year, high collateral score, distal occlusion site, and complete recanalization)
Linear regression analysis model performed only with significant predictive factors for discharge NIHSS score (age per year, high collateral score, and complete recanalization)
Multivariate logistic regression analysis model for poor outcome (modified Rankin scale score > 2) performed with predictive factors (age per year, high collateral score, and complete recanalization)
Discussion
Data presented here indicate that an anatomically based angiographic scoring method that evaluates the extent of pial collateral formation can help predict infarct volume and clinical outcome in patients undergoing thrombolytic treatment for acute stroke. It is evident from this study that patients with favorable pial collateral scores are more likely to have a good outcome at the time of discharge. Modified Rankin discharge scores were the best among patients with both recanalization as well as good pial collateral score (Table 2). All patients with modified Rankin scores of 0 at discharge had good pial collateral scores, and most of these patients also had complete recanalization. A modified Rankin discharge score is, however, shown to be worse among the patients with poorer pial collateral score (4 and 5), regardless of recanalization. It is true, though, that there is a clear benefit to intra-arterial thrombolysis because infarct volume decreases with recanalization even with unfavorable pial collateral scores (Table 1).
Estimates derived from regression analysis models indicate that extent of pial collateral formation has at least as much influence on infarct size and clinical outcome as recanalization does. Furthermore, the presence of good pial collaterals and complete recanalization has a synergistic effect. Other predictors examined in this study did not affect outcomes as significantly as these two variables. This suggests that treatments enhancing collateral formation during acute stroke can reduce infarct volume, whereas treatments restricting collateral vasculature hypothetically enlarge infarct size. Clinical outcome was substantially better in patients with complete recanalization and good pial collateral formation (ie, 1 or 2). It therefore follows that the assessment of pial collateral blood flow on angiography can provide a time efficient, reproducible method to assess the ischemic penumbra at the time of intra-arterial thrombolysis.
Prior Studies
Pial collaterals sustain cerebral blood flow even in the setting of complete occlusion of the MCA or ICA (9, 16). It should be no surprise therefore that infarct size may vary depending on a patient’s ability to form pial collaterals during acute stroke. Saito et al (10) measured the time interval between opacification of the distal internal carotid and the M2 segment via leptomeningial collaterals on 21 angiograms in patients presenting with acute stroke within 24 hours. They found that a time interval <5 seconds (n = 9) resulted in better outcomes with limited infarct size. Although this measurement was not reproduced here, among patients with no recanalization and low pial collateral scores infarct volume varied widely, possibly because of differences in pial collateral transit time. In a different study, collateral circulation semiquantitatively graded as “scarce” or “good” influenced clinical outcome of patients with acute stroke (11). Recently, results from the PROACT II trial semiquantitatively analyzed pial collateral formation on angiography categorized as full, partial, or none and found that presence of good collaterals influences presentation NIHSS score and infarct volume on 24-hour CT scan in a matched subset of patients with MCA occlusions. Results presented here corroborate their findings (8). The present study differs because it provides an objective method of assessing leptomeningeal collateral formation defined on the basis of anatomic extent and demonstrates that this can help predict infarct volume and clinical outcome. Infarct volume and clinical outcome improved significantly independent of recanalization.
Evaluation of collateral blood flow on CT angiography, triphasic perfusion CT (13, 14, 18, 21), xenon CT (22), MR imaging (23, 24), and SPECT (25–27) has correlated with extent of leptomeningeal collateral formation seen on DSA and with clinical outcome (13, 14). The current study corroborates this correlation with clinical outcome. Furthermore, multiphasic helical computed CT has been shown to predict development of severe brain edema in acute ischemic stroke (28). One can therefore infer from the present study—which demonstrates that infarct volume correlates with pial collateral formation—that it should also follow that patients with poor pial collateral formation should go on to develop severe brain edema.
Time to Treatment
Shorter time to treatment is expected to improve outcome, but in this study linear regression analysis indicates that pial collateral score has a greater impact on infarct volume than does time to treatment. Infarct volumes increased significantly with time to treatment in this study. One must consider, however, that in overwhelming numbers (80%) patients were treated beyond 200 minutes of ictus. If one compares the 10 patients with treatment times <200 minutes to those treated >200 minutes the difference in infarct volume is statistically significant. Possibly an ischemic penumbra may be larger and endure longer in patients with better pial collateral scores. This hypothesis is supported by studies indicating that clinical improvement is possible with middle cerebral artery thrombolysis with time to treatment as long as 12 hours in patients with occlusions not involving lenticulostriate vessels (3, 29).
Site of Occlusion
Distal occlusions are expected to result in smaller infarct volumes because the territory at risk is smaller (12). Although there was no significant interaction on regression analysis between pial collateral score and occlusion site, occlusion site had a greater impact on infarct volume with higher pial collateral scores (Table 3). The combination of poor pial collateral formation and distal occlusion site suggested no benefit from thrombolysis in this study; however, the population of patients with this combination is too small to draw such a conclusion. Other investigators have shown that angiographic occlusion site may be an important predictor of recanalization (8, 30–33). This type of interaction may also impact on the significance of occlusion site as a predictor of outcome.
Quereshi’s angiographic grading scheme (12) combines pial collateral formation (subjectively graded as “good” or “bad”) with occlusion site, with a greater emphasis placed on occlusion site rather than pial collateral formation. Although our study grades pial collateral formation, our evaluation of occlusion site graded as proximal or distal indicates that a greater emphasis should be placed on pial collateral formation because, as indicated in our logistic regression analysis, pial collateral formation had a greater impact on outcome. For example, if one compares a patient with excellent pial collaterals at the communicating segment of the internal carotid artery which includes the proximal M1 and M2 segment (so-called carotid T lesion) with one with poor pial collaterals at the M2 segment, the former tends to have a better clinical outcome and lower infarct volume on the basis of our data, especially if there was complete recanalization. Quereshi’s grading scheme would predict that the more proximal the occlusion site, the worse the outcome. Other factors that may need to be taken into account include recanalization.
The source of pial collaterals in patients with ICA bifurcation occlusions differed depending on whether the ACOMA was patent, which could introduce bias. In patients with pial collaterals from occlusions at the internal carotid bifurcation with patent ACOMA, the ipsilateral ACA A2 segment was antegradely reconstituted via the ACOMA, which provides a source for pial collateral supply. In effect, this type of occlusion predominantly affects the MCA territory and spares most of the ACA territory, which is supplied from the contralateral ICA via the ACOM. Therefore, the source of the pial collateral supply here is via ACA pial collaterals and PCA pial collaterals. On the other hand, if the ACOM was not patent during an ICA bifurcation occlusion, the source of pial collateral formation is reduced to the PCA without any supply from the ACA, and, as a result, the affected territory is expected to include both MCA and ACA. In a patient who has a distal ICA occlusion involving the ICA bifurcation and a fetal origin of the PCA with hypoplastic P1 segment and nonfunctional ACOMA the source of pial collaterals includes supply from the meningeal arteries and the posterior circulation perforators.
Age and Sex
The influence of age on pial collateral formation is not clear, on the basis of our data. Whereas average age increased with pial collateral grade, the mean age was lower for those patients with pial collateral scores of 3 compared with the rest of the pial collateral scores. On the basis of linear regression analysis, age was found to have a significant influence on clinical outcome and infarct volumes. Higher pial collateral scores favored women, as did high presentation NIHSS scores. This trend toward higher pial collateral scores in women was not statistically significant.
Study Limitations
Several limitations of this study deserve mention. Evaluations of the extent of pial collateral flow and infarct volumes were derived retrospectively, which could lead to bias. As a result of this, 12 patients who underwent thrombolytic treatment were dropped either because the angiogram or CT was missing, the available angiogram did not include adequate evaluation of pial collateral blood flow, there was antegrade blood flow of the involved territory, or there was a complication. Relatively more ICA occlusions were excluded than any other sites, and ICA occlusions could result in poorer collateral blood flow than MCA occlusions. This is due to the fact that part of the potential pial collateral supply would be restricted at the PCOMA and ACOMA in the former and unrestricted in the latter, where the ICA essentially ends in the ACA and provided a greater potential pressure head than the source of collateral in the case of an occluded ICA. As a result, our patient population would include a few more patients that had poorer collateral blood flow. It would not be reasonable to assume that this would significantly alter conclusions derived from this study regarding the influence of pial collateral flow on outcome. This study also did not analyze anatomic locations corresponding to the so-called eloquent brain regions (ie, Broca’s area, Wernicke’s area, motor strip, visual cortex, etc), which may help explain why clinical outcomes may not always correlate well with infarct volume data.
Conclusion
Findings presented here underscore the importance of evaluating the anatomic extent of pial collateral formation on angiography when assessing the expected outcome in patients undergoing intra-arterial thrombolytic treatment for acute ischemic stroke. Angiographic assessment of the anatomic extent of pial collateral formation can provide reliable ordinal data in a time-efficient method predictive of outcome in patients undergoing intra-arterial thrombolysis for acute ischemic stroke independent of other predictors. This information is especially useful when cross-sectional perfusion studies are not available. Relative to other predictive factors, the extent of pial collateral formation has a significant impact on stroke volume and immediate clinical outcome. In particular, this study defines pial collaterals in terms of anatomic extent on angiography rather than a more subjective assessment of pial collaterals as “good” or “bad” as done in previous studies. Evaluation of pial collaterals may play a dominant role when developing an outcomes grading scheme in acute stroke. Results presented here indicate that good pial collateral formation is a predictor of outcome independent of other factors including recanalization, site of occlusion, age, or time to treatment. It is therefore no surprise that thrombolysis should act to improve clinical outcome at the time of hospital discharge and infarct volume, whether collaterals are poor or good. It is also evident that patients with excellent pial collaterals will have better outcomes than patients with poor pial collaterals, regardless of recanalization.
References
- Received June 2, 2004.
- Accepted after revision January 26, 2005.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Perfusion Collateral Index versus Hypoperfusion Intensity Ratio in Assessment of Collaterals in Patients with Acute Ischemic Stroke
- Endovascular recanalization for symptomatic non-acute middle cerebral artery occlusion: proposal of a new angiographic classification
- Systematic review protocol to assess artificial intelligence diagnostic accuracy performance in detecting acute ischaemic stroke and large-vessel occlusions on CT and MR medical imaging
- Distal Vessel Imaging via Intra-arterial Flat Panel Detector CTA during Mechanical Thrombectomy
- Significance of angiographic clot meniscus sign in mechanical thrombectomy of basilar artery stroke
- Identifying Severe Stroke Patients Likely to Benefit From Thrombectomy Despite Delays of up to a Day
- Predictors of malignant brain edema after mechanical thrombectomy for acute ischemic stroke
- Insula stroke: the weird and the worrisome
- Inter- and intraobserver reliability for angiographic leptomeningeal collateral flow assessment by the American Society of Interventional and Therapeutic Neuroradiology/Society of Interventional Radiology (ASITN/SIR) scale
- Guidelines for evaluation and management of cerebral collateral circulation in ischaemic stroke 2017
- Is bridging therapy still required in stroke due to carotid artery terminus occlusions?
- Value of Quantitative Collateral Scoring on CT Angiography in Patients with Acute Ischemic Stroke
- Pretreatment predictors of malignant evolution in patients with ischemic stroke undergoing mechanical thrombectomy
- CT angiography-based collateral flow and time to reperfusion are strong predictors of outcome in endovascular treatment of patients with stroke
- General Anesthesia Versus Conscious Sedation for Endovascular Treatment of Acute Ischemic Stroke: The AnStroke Trial (Anesthesia During Stroke)
- Complete reperfusion mitigates influence of treatment time on outcomes after acute stroke
- Impact of Pial Collaterals on Infarct Growth Rate in Experimental Acute Ischemic Stroke
- CT perfusion and angiographic assessment of pial collateral reperfusion in acute ischemic stroke: the CAPRI study
- Comparison of four different collateral scores in acute ischemic stroke by CT angiography
- Good Intracranial Collaterals Trump Poor ASPECTS (Alberta Stroke Program Early CT Score) for Intravenous Thrombolysis in Anterior Circulation Acute Ischemic Stroke
- How temporal evolution of intracranial collaterals in acute stroke affects clinical outcomes
- Comparing Vessel Imaging: Noncontrast Computed Tomography/Computed Tomographic Angiography Should Be the New Minimum Standard in Acute Disabling Stroke
- Poor Collateral Circulation Assessed by Multiphase Computed Tomographic Angiography Predicts Malignant Middle Cerebral Artery Evolution After Reperfusion Therapies
- Predictors of Reperfusion in Patients with Acute Ischemic Stroke
- Relative Influence of Capillary Index Score, Revascularization, and Time on Stroke Outcomes From the Interventional Management of Stroke III Trial
- Differential Effect of Baseline Computed Tomographic Angiography Collaterals on Clinical Outcome in Patients Enrolled in the Interventional Management of Stroke III Trial
- Early Mobilization After Stroke: Early Adoption but Limited Evidence
- Diabetic Microangiopathy: Impact of Impaired Cerebral Vasoreactivity and Delayed Angiogenesis After Permanent Middle Cerebral Artery Occlusion on Stroke Damage and Cerebral Repair in Mice
- Impact of Time-to-Reperfusion on Outcome in Patients with Poor Collaterals
- Prediction of Infarction and Reperfusion in Stroke by Flow- and Volume-Weighted Collateral Signal in MR Angiography
- Collateral Score Complements Clot Location in Predicting the Outcome of Intravenous Thrombolysis
- Time and Diffusion Lesion Size in Major Anterior Circulation Ischemic Strokes
- Relative Filling Time Delay Based on CT Perfusion Source Imaging: A Simple Method to Predict Outcome in Acute Ischemic Stroke
- CTA Collateral Status and Response to Recanalization in Patients with Acute Ischemic Stroke
- Arterial Spin-Labeled Perfusion Imaging in Acute Ischemic Stroke
- Thrombus length estimation in acute ischemic stroke: a potential role for delayed contrast enhanced CT
- Relative Cerebral Blood Volume as a Marker of Durable Tissue-at-Risk Viability in Hyperacute Ischemic Stroke
- Expanding the role of NCCT in acute stroke imaging: thrombus length measurement and its potential impact on current practice
- Admission Insular Infarction >25% Is the Strongest Predictor of Large Mismatch Loss in Proximal Middle Cerebral Artery Stroke
- Prognostic Evaluation Based on Cortical Vein Score Difference in Stroke
- Recommendations on Angiographic Revascularization Grading Standards for Acute Ischemic Stroke: A Consensus Statement
- Pathologic validation of clot length determined using thin section non-contrast CT
- Imaging-based selection for intra-arterial stroke therapies
- The capillary index score: rethinking the acute ischemic stroke treatment algorithm. Results from the Borgess Medical Center Acute Ischemic Stroke Registry
- Incidence and outcome of procedural distal emboli using the Penumbra thrombectomy for acute stroke
- Factors Influencing Clinically Meaningful Recanalization after IV-rtPA in Acute Ischemic Stroke
- Factors associated with rapid neurological improvement 24 h following intra-arterial thrombolytic treatment for acute ischemic stroke
- Revascularization grading in endovascular acute ischemic stroke therapy
- Reperfusion Rates Following Intra-Arterial Thrombolysis for Acute Ischemic Stroke: The Influence of the Method for Alteplase Delivery
- Comparison of Arterial Spin Labeling and Bolus Perfusion-Weighted Imaging for Detecting Mismatch in Acute Stroke
- Clot Characterization by Noncontrast CT to Predict IV tPA Failure
- Systematic Review of Methods for Assessing Leptomeningeal Collateral Flow
- Extending the Time Window for Endovascular Procedures According to Collateral Pial Circulation
- Effect of Time to Reperfusion on Clinical Outcome of Anterior Circulation Strokes Treated With Thrombectomy: Pooled Analysis of the MERCI and Multi MERCI Trials
- Regional Leptomeningeal Score on CT Angiography Predicts Clinical and Imaging Outcomes in Patients with Acute Anterior Circulation Occlusions
- Arterial Spin-Labeling MRI Can Identify the Presence and Intensity of Collateral Perfusion in Patients With Moyamoya Disease
- The impact of diabetes on the extent of pial collaterals in acute ischemic stroke patients
- Collateral Flow Averts Hemorrhagic Transformation After Endovascular Therapy for Acute Ischemic Stroke
- Collateral Flow Predicts Response to Endovascular Therapy for Acute Ischemic Stroke
- MRI-Based Selection for Intra-Arterial Stroke Therapy: Value of Pretreatment Diffusion-Weighted Imaging Lesion Volume in Selecting Patients With Acute Stroke Who Will Benefit From Early Recanalization
- Distal hyperintense vessels on FLAIR: An MRI marker for collateral circulation in acute stroke?
- Intra-Arterial Stroke Therapy: An Assessment of Demand and Available Work Force
- Predictors of Hemorrhage Following Intra-Arterial Thrombolysis for Acute Ischemic Stroke: The Role of Pial Collateral Formation
- Determinants of the distribution and severity of hypoperfusion in patients with ischemic stroke
- Impact of collateral flow on tissue fate in acute ischaemic stroke
- Size Matters: Hemorrhage Volume as an Objective Measure to Define Significant Intracranial Hemorrhage Associated With Thrombolysis
- Accuracy of Pre- and Postcontrast 3D Time-of-Flight MR Angiography in Patients with Acute Ischemic Stroke: Correlation with Catheter Angiography