
Abstract
BACKGROUND AND PURPOSE: The appearance of vacuum clefts (VCs) of the vertebral bodies has frequently been considered pathognomonic for avascular necrosis. Until recently, this was considered to be a rare finding that might indicate excessive motion at the fracture site. Our aim in this retrospective study was to determine the occurrence and location of these clefts in patients with osteoporotic vertebral fractures and evaluate the risk factors involved for developing these clefts in such patients.
METHODS: The records of 66 patients with 101 painful osteoporotic vertebral fractures who were treated by vertebroplasty in our department were reviewed. All the fractures with VCs were collected. Age, sex, degree of deformity, and extent of degenerative changes in the adjacent disk space were compared with those found in the patients without clefts.
RESULTS: VCs were found in 26 fractured vertebrae of 26 patients. They were significantly more common in elderly men who had deformed fractures located at the thoracolumbar junction, when compared with fractures without clefts, especially when degenerative changes were observed in the adjacent disk space.
CONCLUSION: This study suggests that VCs, which have long been considered pathognomonic for avascular necrosis (Kümmell disease), are not rare and most probably represent fracture nonunion. Elderly patients who have deformed fractures at the thoracolumbar area have a higher risk for developing clefts, mainly when there is degeneration of the adjacent disk space.
Vacuum clefts (VCs) of the vertebral bodies are radiographically recognized as a vacuum or air-filled cleft inside the vertebral body (1). They are generally considered to be a sign of avascular necrosis of the vertebral body, also known as Kümmell sign, and until recently were not considered to be associated with osteoporotic fractures (2). In the past, the occurrence of these clefts in adult patients with benign and malignant musculoskeletal disorders was considered uncommon (3). Recent studies, however, have shown that these clefts are not so rare (4), are frequently connected with osteoporotic fractures, and have dynamic mobility in different body postures indicating instability within the fracture (5).
Motion within the fracture has been correlated with a high probability of severe, persistent pain, and good results have been reported following percutaneous vertebroplasty. The pain relief is thought to be due to the elimination of the excessive motion as a result of cementing (6). In a recent study, it was suggested that, because motion in a clefted vertebra is greater than in a fractured vertebra without a cleft, patients with a VC of the vertebral body might achieve better pain relief following vertebroplasty (7).
The purpose of this study was to determine the occurrence of VCs in symptomatic osteoporotic vertebral fractures, localize their anatomic location, and evaluate the risk factors for developing these clefts, to offer more aggressive treatment for those at risk.
Methods
All the pre- and postoperative radiographs of 66 patients with osteoporotic vertebral fractures who underwent vertebroplasty at our medical center between the years 2000 and 2002 were retrospectively reviewed. An additional six patients were excluded because their files contained insufficient data or some of the radiographs were missing.
The indications for vertebroplasty were painful osteoporotic vertebral fractures between T5 and L5, in patients >60 years of age, that were refractory to conservative treatment with braces, reduced activity, and analgesics.
The painful vertebra was located by a combination of local tenderness at the fracture site and the typical appearance of such a fracture on bone scan (in all cases) and on MR imaging (in 41 cases). Patients with recent fractures, neurologic deficits related to fracture, or canal compromise by the posterior vertebral wall and those whose general condition prevented them from lying prone were excluded.
Treated vertebrae were subdivided into those with VCs (group 1) and those without VCs (group 2). VCs were diagnosed by radiolucent lines seen on anteroposterior and lateral radiographs of the fractured vertebrae. According to their radiographic appearance we could observe two patterns of clefts:
1. Clefts parallel to the fractured endplate, which could be subdivided into those associated with the upper endplate (Fig 1) and those associated with the lower endplate (Fig 2).
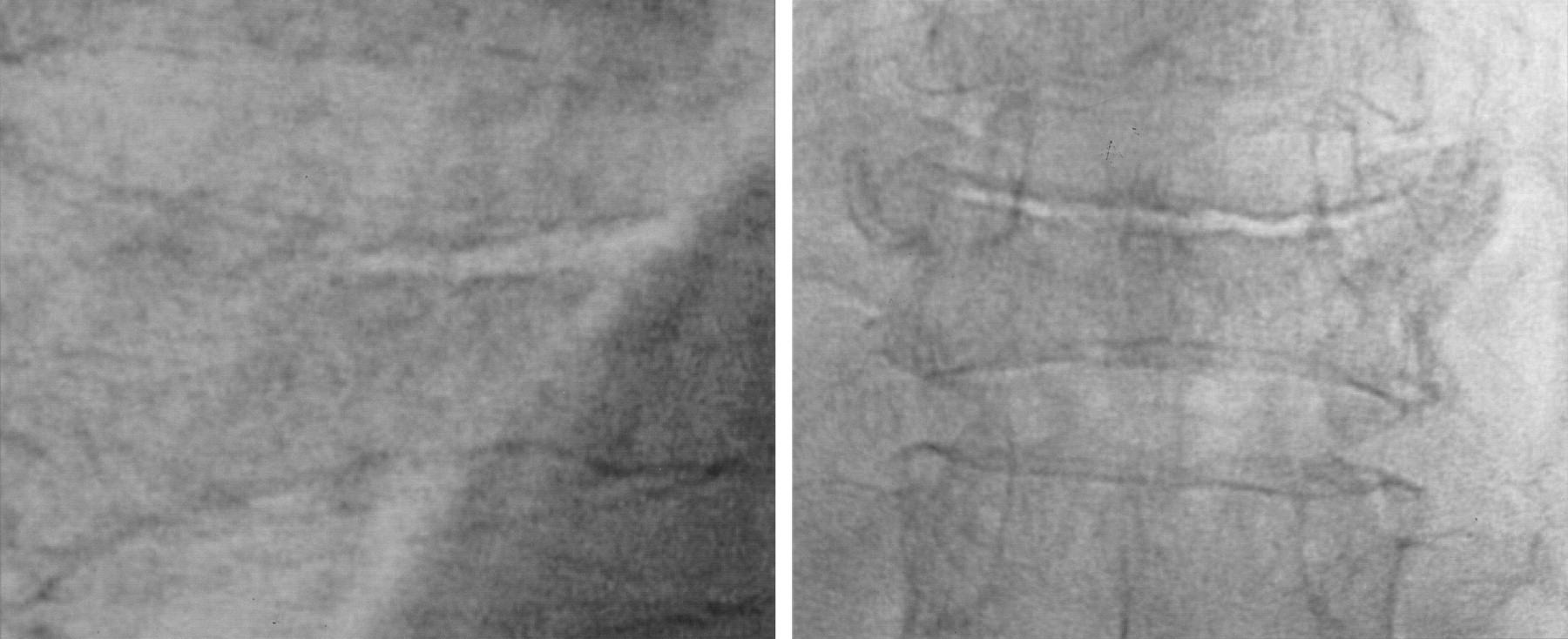
VC associated with an upper endplate fracture.
VC associated with a fracture of the lower endplate.
2. Vertical clefts that were found to pass from the upper to the lower endplate (Fig 3).

VC passing from the upper to the lower endplate.
All vertebroplasties were performed with the patient in a prone position, and to achieve some fracture reduction patients were positioned in slight hyperextension, by inserting pillows under the chest and pelvis. All lateral radiographs taken in this position before vertebroplasty were checked for VCs that were not seen on the standing radiographs. With the exception of the first two patients, the trocar was introduced into the VC in all cases.
The fractured vertebrae in both groups were classified according to Eastell et al (8) as either wedge, biconcave, or compression. Each type was subdivided, according to the severity of deformation, into mild (wedge exceeding 15° or height loss of up to 25%), moderate (wedge of 15°–30°, height loss of 25%–50%) or severe (wedge >30° and height loss of 50% or more).
Degenerative changes at the disk space adjacent to the fractured endplate or the cleft were classified according to Kellgren and Lawrence (9), as either grade 0 (no degenerative changes present), grade 1 (doubtful changes suspected), grade 2 (minimal changes found), grade 3 (moderate narrowing of the disk space observed), and grade 4 (severe disk space narrowing). For the purpose of this article, grades 0 and 1 were classified as normal, grades 2 and 3 as mild to moderate, and grade 4 as severe degenerative changes. If both endplates were fractured, or in the case of VCs, the disk space with the more advanced degeneration was recorded.
In both groups, data concerning patient age, sex, and level of fracture were recorded.
Serial radiographs taken at intervals of <1 month, for at least 4 months during the period of time that elapsed between the first event of back pain and the vertebroplasty, were available from four of the patients in group 2. These images were carefully examined for the presence of a VC during any stage of fracture healing. The pain intensity before vertebroplasty and at follow-up was evaluated by using the visual analog scale.
The statistical workup was done by using the t test for age difference and the Pearson χ2 test for the differences in sex, extent of degenerative changes in the neighboring disk space, fracture type and deformation, fracture level, and pain intensity.
Results
Sixty-six patients underwent 101 vertebroplasties for painful vertebral fractures. Sixty-nine other fractures were identified on the anteroposterior and lateral radiograms, but were not opacified because, according to the pain location and bone scan, they were asymptomatic. In 24 of the 26 patients with VCs, the clefts were opacified. The other two patients were the first two, and we were not aware at that time of the importance of filling the cleft with cement. Age, sex, fracture type, location, and extent of the deformity in both the groups of the cemented clefts and the cemented fractures without clefts are presented in Table 1.
Age, sex, fractured vertebra, fracture type, and amount of deformation presented in the fracture in group 1 (with VCs) and group 2 (without VCs)
Twenty of the VCs were parallel to the endplate, and six were vertical clefts that connected both endplates.
Five of the 26 VCs were identified only on the hyperextension radiographs performed on the operating table. The other 21 were already seen on the preoperative standing radiograph.
Table 2 demonstrates the extent of degenerative changes in the adjacent disk space in both groups of patients who underwent vertebroplasty.
The extent of degenerative changes in the disk space adjacent to the fractured endplate or the VC according to Kellgren and Lawrence classification (9)
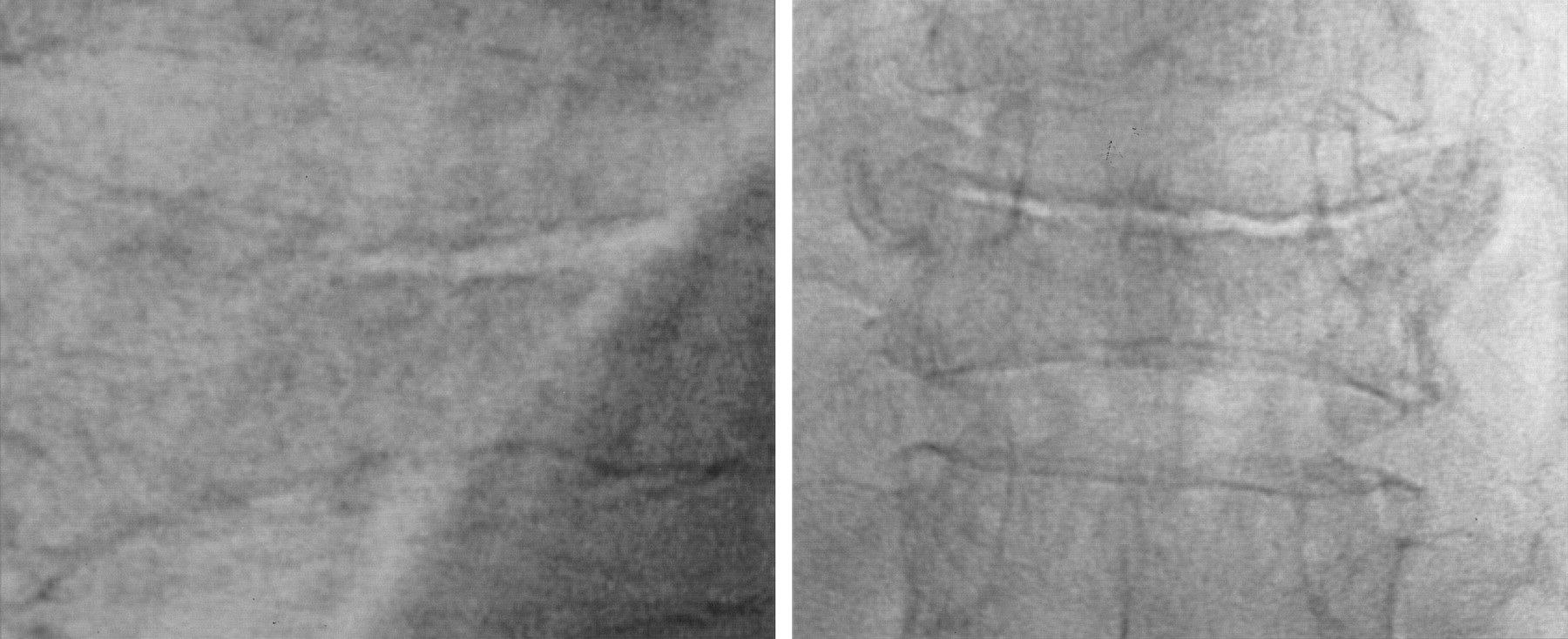
In one patient from group 2, in whom frequent serial radiographs were found for the period between the fracture and the vertebroplasty, a radiolucent line similar to a VC was found during the healing process. In this patient, the fracture was found at the upper endplate. The radiolucence appeared 3–5 weeks after the fracture, was evident on the radiograph, and disappeared on the next one following some further collapse of the upper endplate (Fig 4). In this patient, the adjacent disk space did not show any signs of degenerative changes.

Serial lateral radiographs of a 69-year-old patient from group 2, with severe low back pain following forward bending.
A, Initial radiographs demonstrate mild collapse of the upper endplate.
B, One month later, a radiolucent line is seen below the fractured endplate.
C, Five weeks later, the radiolucent line has disappeared following further collapse of the endplate.
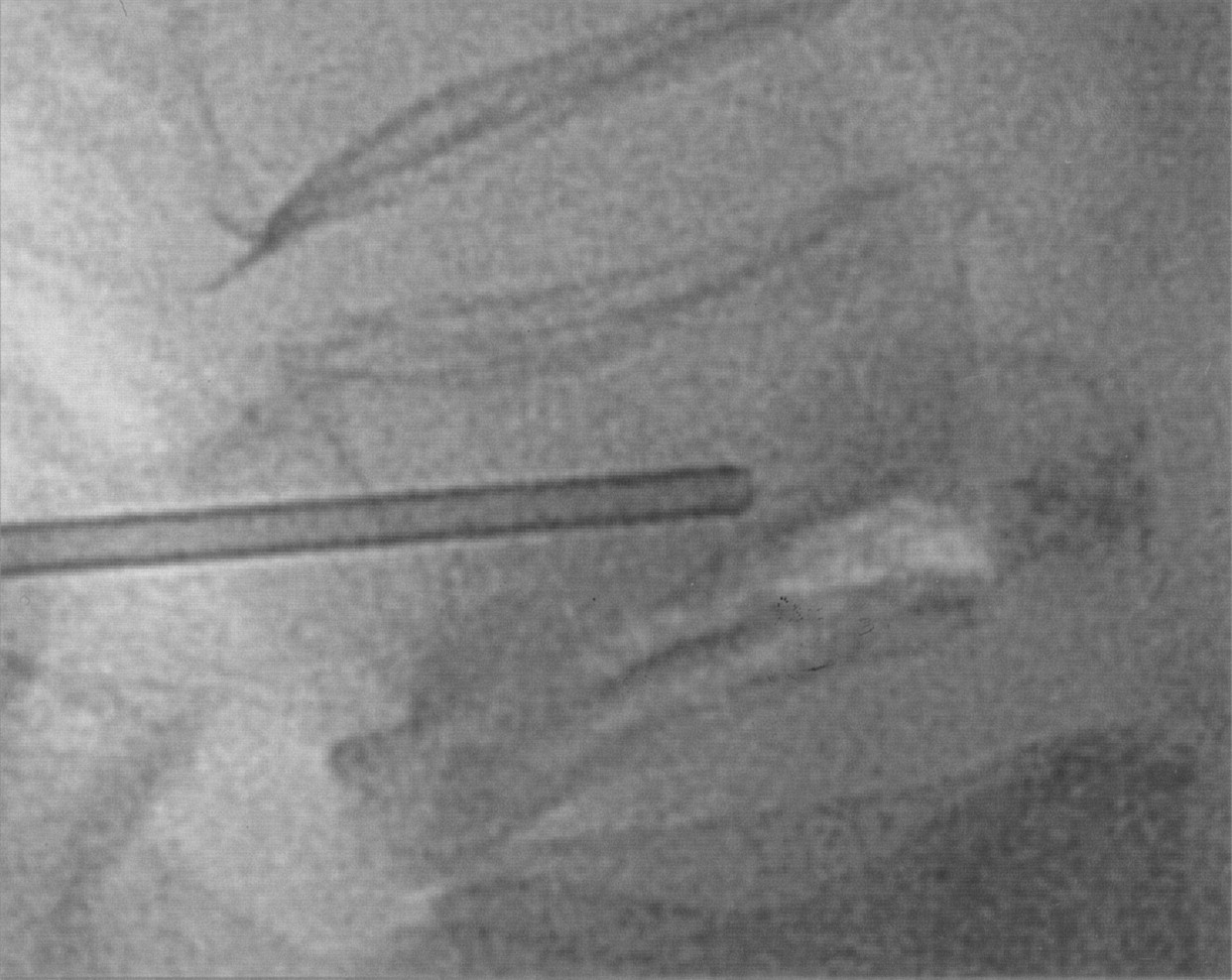
In seven of the VCs, continuation of the gas from the adjacent disk space into the cleft was seen (Fig 5). In all of these patients, the degree of disk degeneration was of Kellgren and Lawrence grade 3 or 4. Five of them were associated with severe and two with moderate deformity of the fractured vertebra. The fractures in this group were biconcave (two fractures), compression (three fractures), and wedge (two fractures). In 16 of the 24 patients with VCs, the cement that was introduced into the cleft remained there (Fig 6); in four patients, cement leakage to the degenerative disk was observed while we were trying to fill the cleft (Fig 7); in one case, a cement leakage lateral to the vertebral body was observed; and in the other three patients cement was found in other parts of the vertebral bodies.

Radiolucent line is visible, penetrating the degenerative disk above.

Lateral radiographs of L3 following selective cementation of the cleft.

Cement leakage to the upper disk via the cleft following cementation of the cleft.
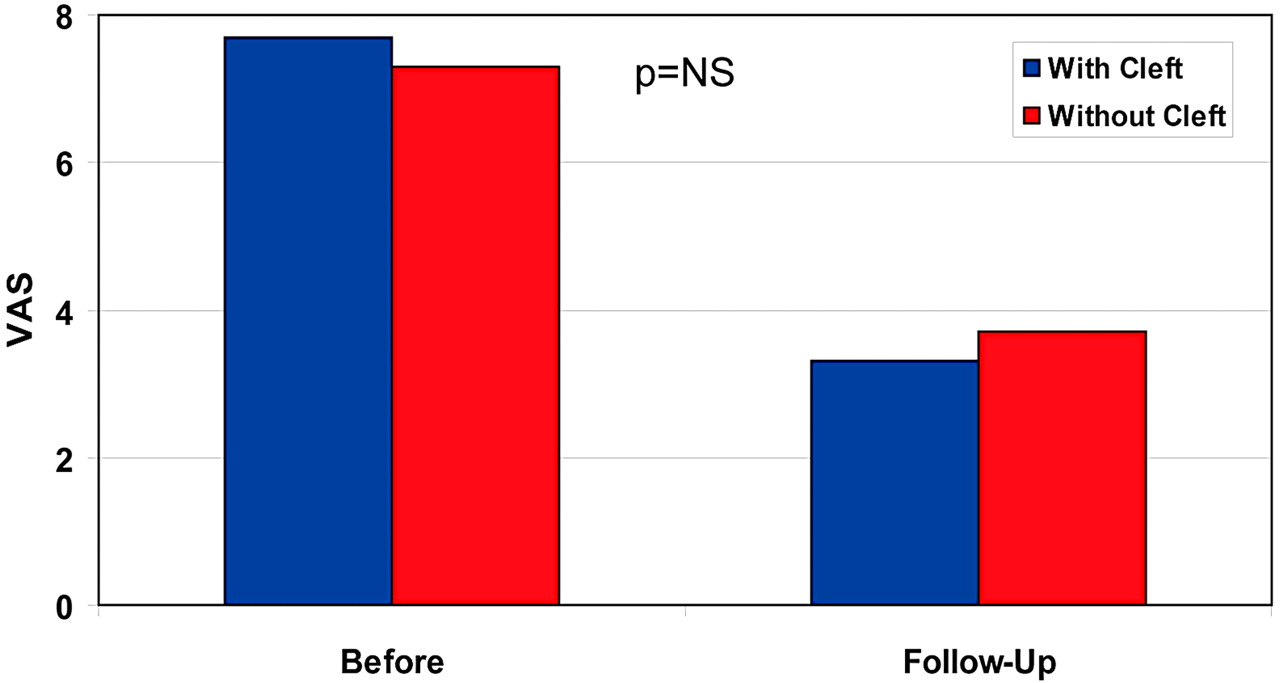
No other complications were observed in the patients of group 2 and none underwent further surgery. The pain intensity before vertebroplasty and at follow-up in the patients with VCs is presented in Fig 8.

Pain score in both groups of patients.
Discussion
In the present study, VCs were found in patients with back pain undergoing vertebroplasty. It appears that these VCs are much less common in the population with asymptomatic fractures, but we were unable to confirm this here because it is beyond the focus of the study. In all 26 patients with a VC, the cleft was found clinically and on bone scan or MR image to be the source of pain, and for this reason vertebroplasty was performed. For comparison, only 52% of the osteoporotic fractures without a VC were painful and hence underwent vertebroplasty.
In one of the patients with sequential radiographs, we found that a radiolucent line appeared as a stage in the healing process of a vertebral fracture. Therefore, it is theoretically possible to postulate that a radiolucent line similar to a VC might appear as a phenomenon of transient bone resorption beneath the fractured endplates during the healing process of a fracture. Such phenomena might frequently be seen in the healing process of any other fracture (10).
Most VCs were found beneath the fractured upper endplate, where the vascular supply is more tenuous (11). As a result, any factor interfering with the healing process of the fracture may result in a nonunion that appears on radiographs as persistence of the radiolucent line of the cleft and on MR image as a hypointense line (Fig 9). Osseous necrosis bounded by fibrocartilaginous membrane, typical in nonunion, was found in biopsies obtained from the region of the clefts (4, 12). As with any nonunion, excessive motion might be found at the fracture site and the fracture margins might be sclerotic. In our patients with persistent VCs, nonunion was made apparent by the fact that, on hyperextension, five additional clefts could be found that were not seen on standing radiograph, a phenomenon that has been described elsewhere (5)and by the fact that in one of our first patients, in whom the cement was injected outside the cleft, it was found to reach the sclerotic margins of the cleft without penetrating it (Fig 10).
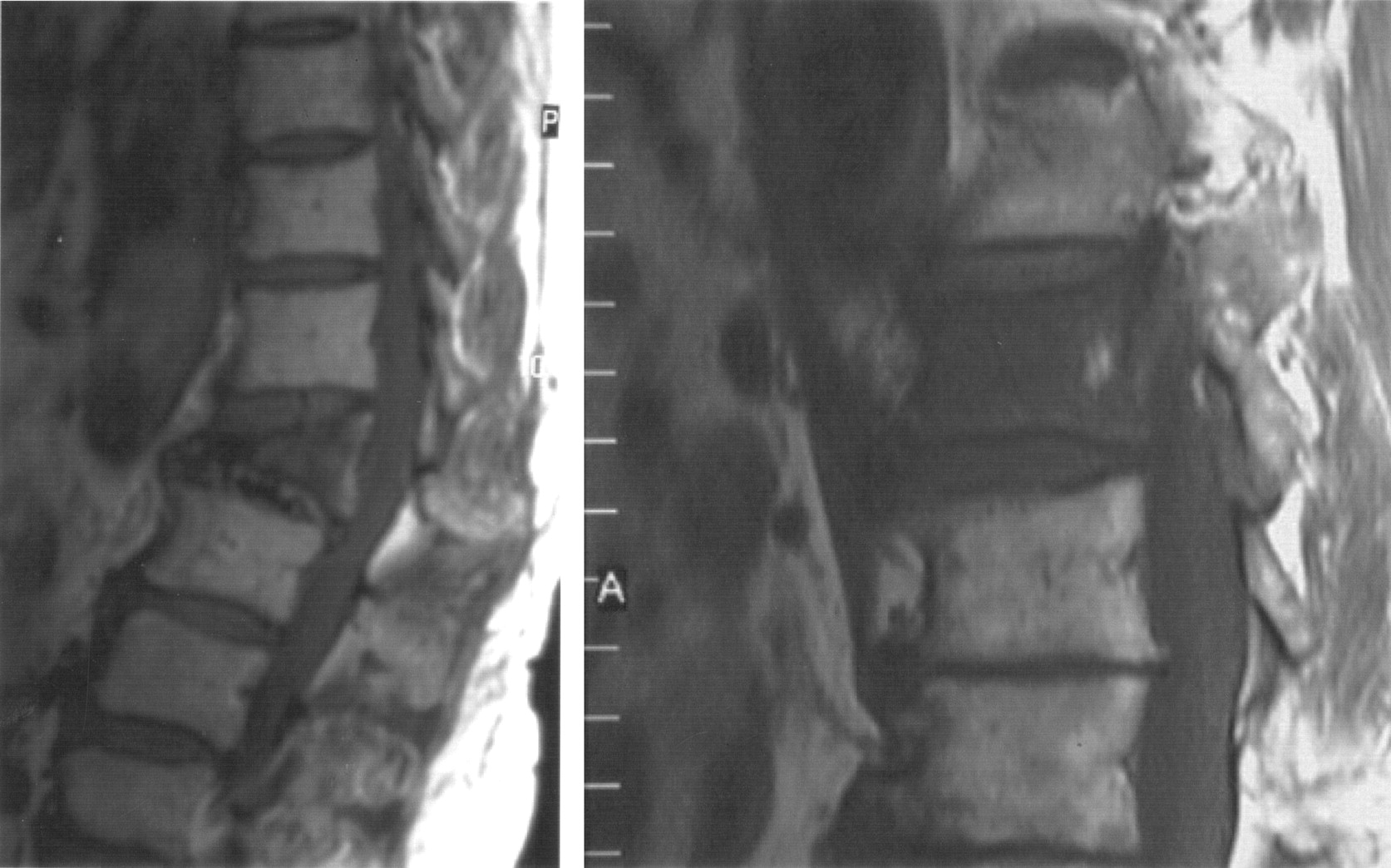
T1-weighted images of fractured vertebrae seen on MR image. On the left, a vertical VC demonstrated as a hypointense line is seen crossing the collapsed vertebra; on the right, no cleft is seen.

CT reconstruction of a fracture in L2 following vertebroplasty. The cement was injected into the vertebral body and surrounds the sclerotic margins of the cleft without penetrating it.
Fracture nonunion in long bones is more common in more severe fractures, in older patients and when the vascular supply at the fracture sight is compromised (13). Indeed, the clefts were found in our study in older patients with the more severe fractures, more significant collapse and angulation, and in an area that already has a poor vascular supply.
In our study, we were also able to demonstrate clearly that degenerative changes in the disk space neighboring the fracture were significantly more pronounced in the group of patients with VCs. This could be due to the diminished blood supply in the degenerated disk, which increases the risk of osteonecrosis in the neighboring fractured endplate, or as a result of excessive motion at the fractured site due to the stiff degenerated segment. A similar problem can be found in type 2 dens fractures, where a combination of excessive motion and impaired vascular supply in older age, leads to high rates of nonunion (14, 15). With continuation of motion in the cleft, the adjacent endplate might be fractured, and continuation of the radiolucent line of the cleft into the disk space was found in 26% of the patients with the clefts, thereby increasing the risk of cement leakage into the disk space, as indeed occurred in some of these patients (Fig 7).
We were able to locate different types of VCs according to their radiologic appearance. The most common clefts were those accompanying the fracture lines at the endplates, in particular the upper one. If significant collapse was present, the clefts were found to take on a more vertical orientation. Recognizing the different patterns of VCs is not merely of academic interest, but has practical applications. In our study, filling the clefts (group 1) was found to produce similar results to cementation of the vertebrae (group 2) (7). Identification of the different patterns and their association to the fracture lines might contribute to better results and to a lesser risk of cement leakage into the adjacent disk following vertebroplasty.
The characteristics of VCs are almost indistinguishable from those associated with Kümmell disease (16). In Kümmell disease, the clefts are considered to be posttraumatic avascular necrosis of the vertebral body that occurs primarily in elderly, female patients with osteoporosis, most frequently at the thoracolumbar junction, and usually involves the upper endplate (3, 16). We agree with McKieman et al (4) that the characteristics of this disease are similar to those found in our patients with VCs. Among our patients with painful fractures who underwent vertebroplasty, those with clefts were compared with those without clefts and were found to be older, with fractures more often at the upper endplate. In addition, the clefts were associated with more severe deformation and, as stated elsewhere, were located mainly at the thoracolumbar junction (4), whereas in patients without clefts the fractures were found more commonly at the lumbar area. The only difference between our patients and those with Kümmell disease was that we found significantly more men in the group of patients with VCs, a finding not reported in Kümmell disease.
Conclusion
The results of this study indicate that elderly patients, with a severely collapsed or deformed fracture at the thoracolumbar junction, have a high risk of developing a nonunion of the fracture that will present on radiography as a VC. This risk increases when the disk space adjacent to the fractured endplate is severely degenerated. When a cleft is present, it will most probably be painful, and, if treated by vertebroplasty, the patients should be carefully monitored for signs of sclerotic margins that might prevent filling of the cleft. Furthermore, continuation of the cleft into the adjacent disk space might result in cement leakage into this space.
References
- Received October 18, 2004.
- Accepted after revision January 20, 2005.
- Copyright © American Society of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}