
Abstract
Summary: The “prong deflector” tool improves accuracy and ease of access to the cervical disk spaces for use in cervical diskography. The tool allows control, deflection, and stabilization of vital neck structures (carotid artery, thyroid cartilages and pharynx) while allowing fluoroscopic visualization during needle insertion without direct operator radiation exposure. Use of the prong deflector resulted in marked reduction of fluoroscopy per cervical level studied because of more rapid access to disk space.
Cervical diskography is a challenging and difficult interventional spine procedure. Vital structures such as the vertebral artery and spinal cord must be avoided, making fluoroscopic inspection during needle placement essential. The thyroid cartilage and carotid artery frequently overlap the approach to individual disk spaces requiring identification and displacement. Patient motion can present a problem because of needle deflection caused by swallowing during intermittent fluoroscopic inspection.
Although the larynx and carotid artery can be manually displaced with the fingers and the anterior vertebral column palpated to feel for the targeted disk, it remains difficult to visualize fluoroscopically the needle approach during insertion without excessive operator radiation exposure. In addition, direct palpation of the vertebral column can be difficult in larger patients.
To address these issues we recently instituted the use of a self-constructed “prong deflector” tool to achieve control of neck structure during needle insertion while allowing fluoroscopic inspection without direct operator radiation exposure. This report describes our recent experience with this technique.
Description of Technique
Cervical diskography was performed with the assistance of the self-constructed prong deflector tool in 15 consecutive patients (42 cervical levels) between March 2003 and May 2004. For comparison, the previous 15 consecutive cervical diskograms performed without the use of the deflector (32 cervical levels) were identified and the clinical/procedure features of these two groups were reviewed. Institutional review board approval was obtained for this retrospective evaluation.
Fifteen patients were male and 15 were female (average age, 46.7 years; age range, 32–62 years). Clinical problems prompting cervical diskography included axial neck pain, headache, upper thoracic pain, shoulder pain, and radiating arm pain, alone or in combination. Patients’ physical characteristics were not considered a barrier to performing diskography. Average weight was 176 pounds (range, 125–242 pounds) and average height was 5 feet 7 inches (range, 5 feet 1 inch–6 feet 1 inch) with patients commonly presenting significant challenge to disk space access due to moderate neck girth with combined short stature and moderate weight (5 feet 1 inch, 195 pounds; 5 feet 5 inches, 242 pounds; 5 feet 6 inches, 210 pounds).
Cervical disk spaces studied with the prong deflector tool are summarized in Table 1. Overall, cervical diskography was performed at one cervical level in 5 patients (all predeflector), two cervical levels in 8 patients, three cervical levels in 13 patients, and four cervical levels in 2 patients.
Number of levels studied by cervical discography
The Prong Deflector Tool
The prong deflector tool is demonstrated in Figure 1. It consists of a plastic-covered metallic prong that simulates the size and curvature of the operator’s index and middle fingers attached to an 8-cm-long aluminum handle for operator control. Prong gap is approximately 3 cm. The prong is cleansed before each procedure with disinfectant and alcohol wash and inserted into a sterile surgical glove for use in the sterile field. This simulates the operator’s gloved hand and fingers.

The prong deflector tool has an aluminum handle for operator grasp and control attached to a plastic covered steel two tine active end that is shaped to resemble the operator’s fingertips with slight tine curvature and a 3–3.5-cm gap.
Cervical Diskogram Technique with the Prong Deflector Tool
Several authors have previously described the technique of cervical disk space access (1–3). The technique is minimally modified when using the prong deflector. The cervical disk spaces are accessed by using C-arm fluoroscopy for needle guidance. Conscious sedation is administered along with preprocedure antibiotics. Comfortable neck extension and 20–30° of the leftward head turn is established for right-sided patient access. After the neck is cleansed and fluoroscopy positioned for the targeted disk spaces, the carotid artery and thyroid cartilage are palpated to identify ultimate position of the prong deflector. Mobility of anterior neck soft tissues is also tested to assess achievable tissue displacement. The carotid artery is displaced laterally and the operator’s fingers are replaced with the prong deflector. Soft-tissue pressure and thyroid cartilage displacement are further performed with the applied prong deflector.
The lateral margin of the thyroid cartilage is assessed fluoroscopically by moving the larynx with the prong (Fig 2). With gentle pressure, the thyroid cartilage is displaced toward the midline to establish a clear access pathway to the targeted disk space (Fig 2B). After the trajectory has been identified and a pathway cleared, the 25-gauge spinal needle (BD Medical Systems, Franklin Lakes, NJ) is inserted into the neck soft tissues at the appropriate position between the prongs of the deflector (Figure 3A, -B). With intermittent fluoroscopic guidance the needle is progressively advanced to the targeted disk space. The intended target location is just medial to the right uncinate process, directing the needle toward the center of the disk and avoiding the vertebral artery. Depth is assessed by tactile sensation of the disk annulus and confirmed with PA and lateral fluoroscopy. Diskogram is performed with a 0.1–0.3-mL injection of nonionic contrast material (Iohexol 240 mgI/mL; Amersham Health, Princeton NJ). CT imaging of the injected cervical levels was obtained following diskography in all patients.
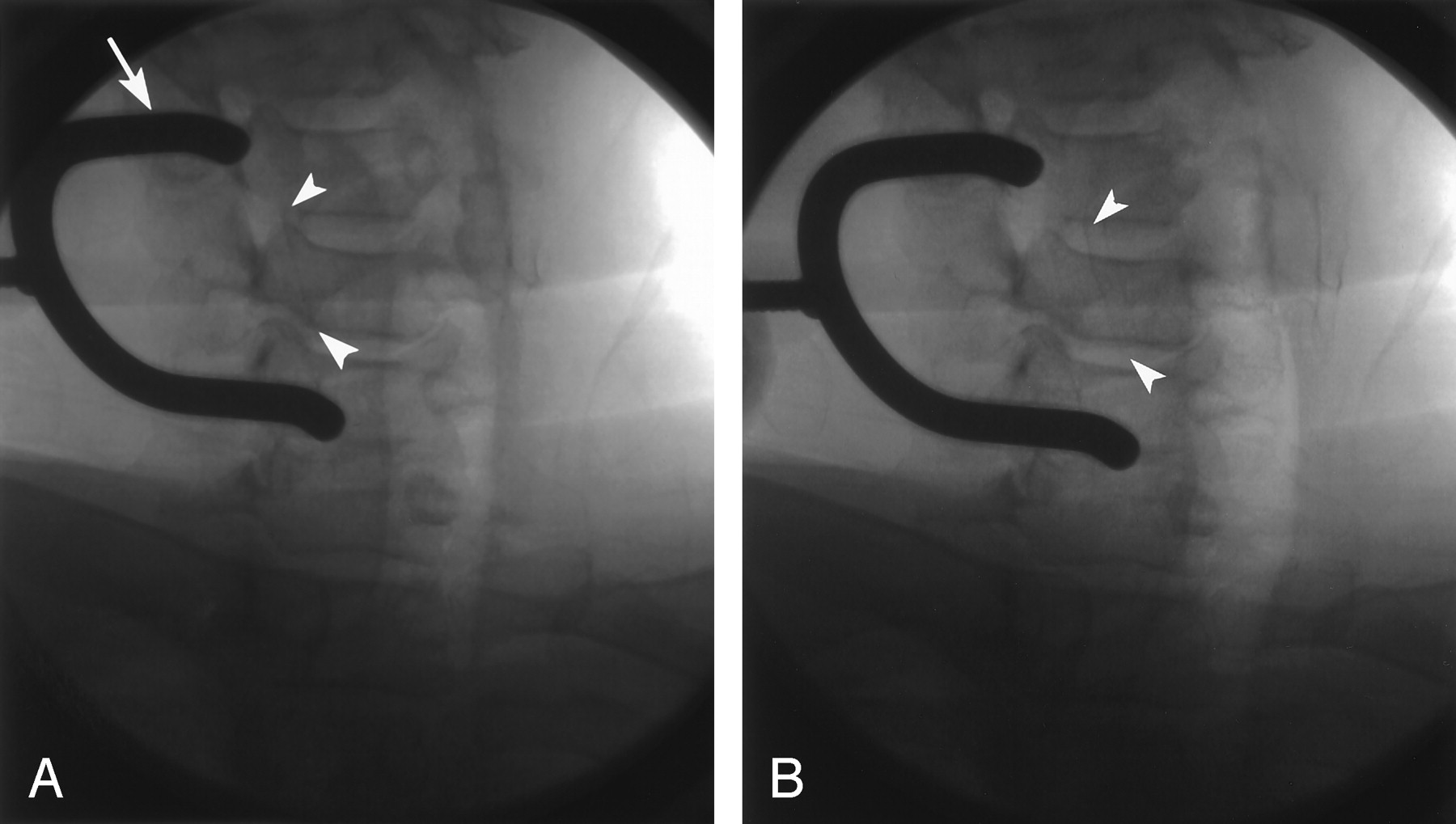
Example of thyroid cartilage displacement visualized at fluoroscopy during cervical diskography in a 49-year-old man with severe neck pain radiating to his left arm and shoulder.
A, The prong deflector (arrow) lies adjacent to the right lateral margin of the thyroid cartilage (arrowheads). The cartilage is difficult to visualize as it overlies the disk spaces, uncinate processes and Lushka’s joints on the patients right.
B, With displacement of the thyroid cartilage toward the midline, the lateral margin of the cartilage is now visible (arrowheads) and can be seen, no longer overlying the lateral aspect of the disk space and no longer overlying the intended target.
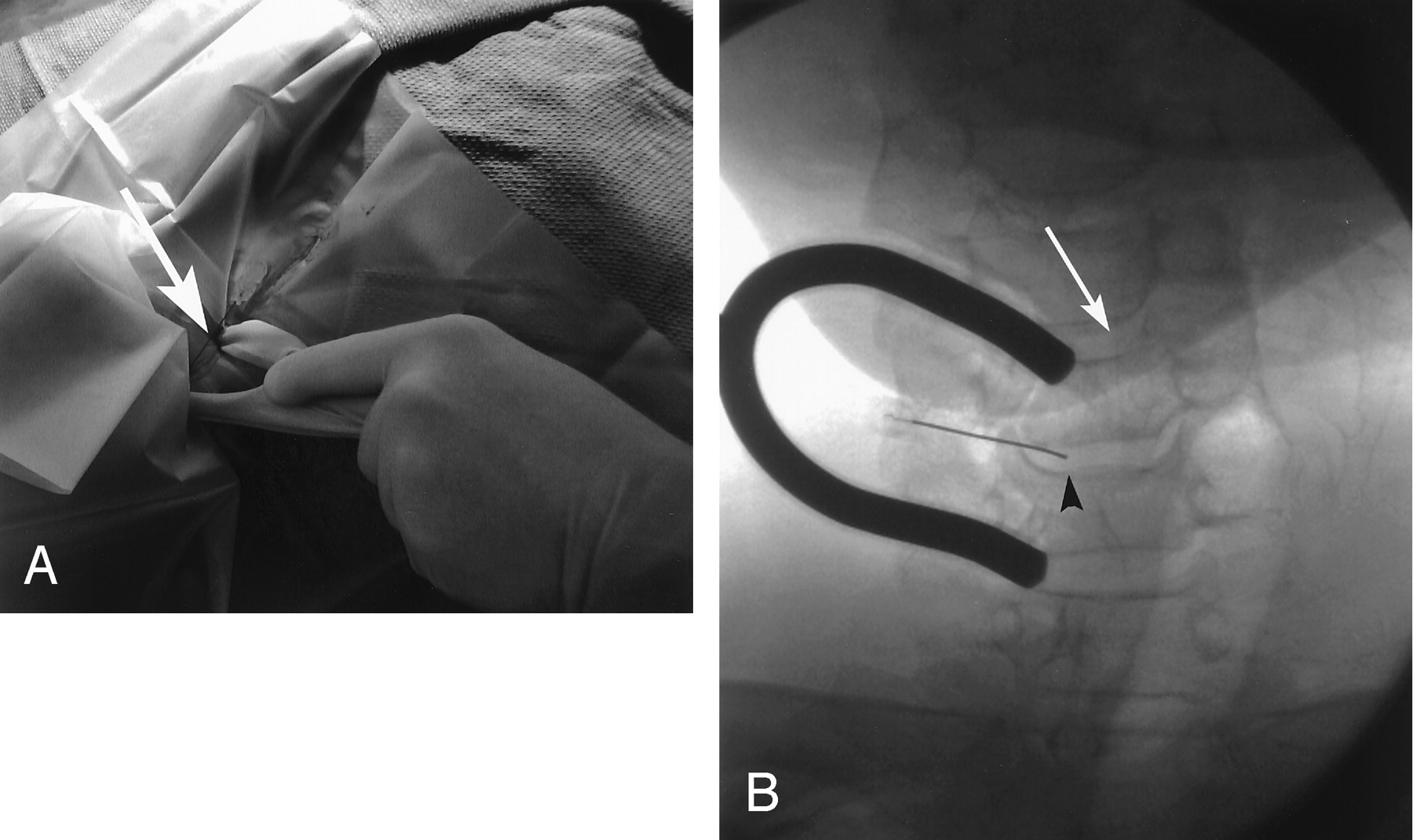
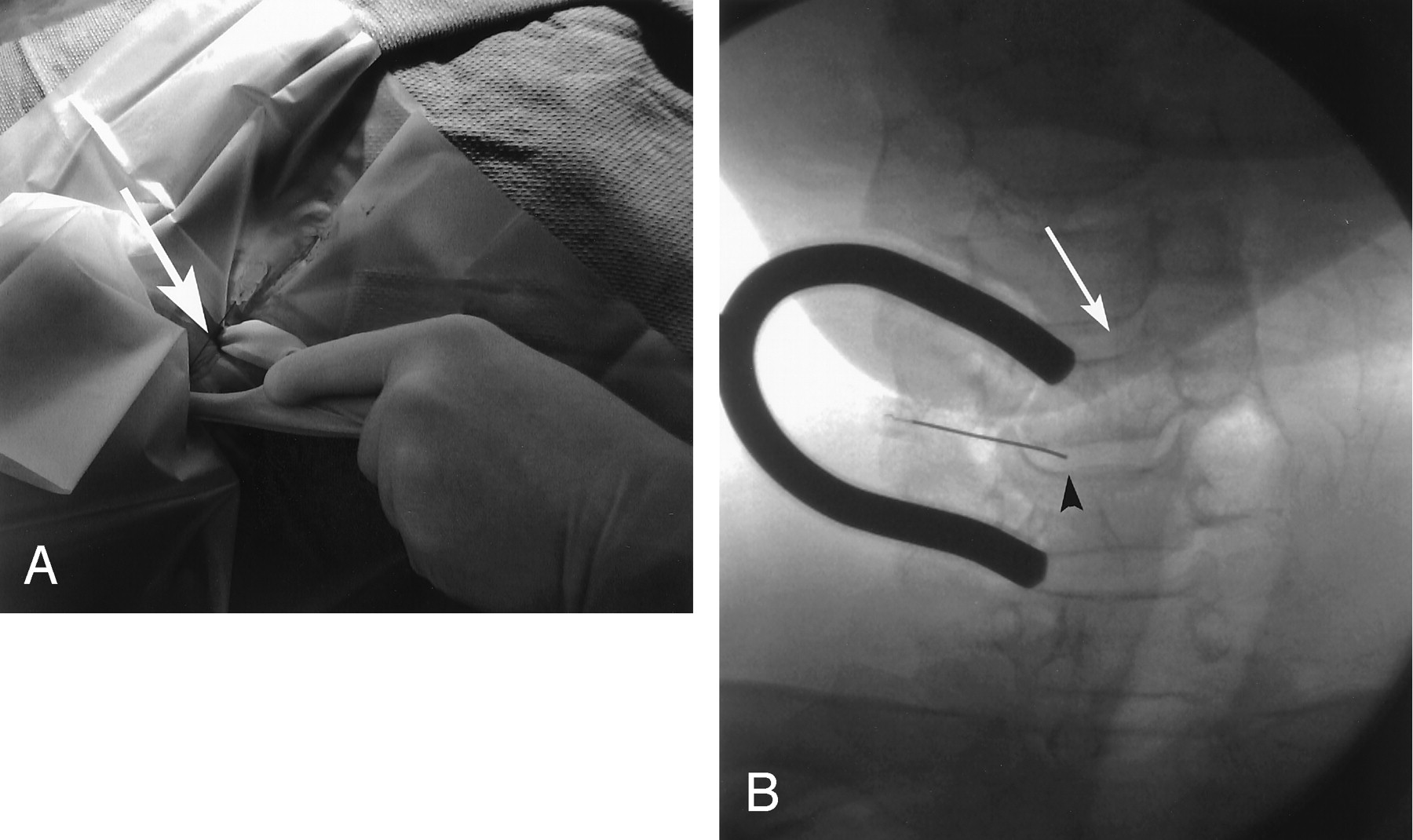
Operator insertion of the 25-gauge needle by using the prong deflector for neck tissue control.
A, The prong deflector maintains control of the neck structures while the needle is inserted (arrow). Fluoroscopic inspection of the needle position and trajectory can be obtained without direct operator exposure of the central beam.
B, Example of fluoroscopic visualization of needle insertion during cervical diskography with assistance of the prong deflector tool in a 44-year-old man with persistent neck pain radiating to his posterior left shoulder. The prong deflector is being used during needle insertion of the C5–6 disk space with thyroid cartilage displaced medial to the prong deflector tines (white arrow) and clear access to the disk space established (black arrowhead).
Parameters Evaluated
In the 15 cervical diskograms performed with the prong deflector, neutral and prong displacement images were fluoroscopically visualized and recorded to identify position of the thyroid cartilage and define clear disk space access. Position of thyroid cartilage was identified and disk spaces covered by cartilage in the procedure position were assessed. Levels where cartilage covered a disk space were recorded and clear access to the disk space after larynx displacement was identified and tabulated.
Thyroid cartilage position and relationship to the neurovascular bundle was assessed on the postdiskogram CT images. Sedation doses required for comfortable completion of the procedure were tabulated from the conscious sedation nursing record. Recorded total procedure time and fluoroscopy time was tabulated and compared for both the prong deflector and “traditional” cervical diskogram groups.
Observations
Cervical Diskogram Technique
In the prong deflector group, the margin of the thyroid cartilage partially or completely covered the approach to the disk space at 38/42 levels studied. Overlap of the disk spaces and the effects of cartilage displacement in these diskograms are summarized in Table 2. Partial overlap of the thyroid cartilage was present at 11/38 levels (29%), with complete coverage of disk space access noted in 27/38 levels (71%). At all 38 levels, the operator was able to employ the prong deflector effectively to deflect the thyroid cartilage for adequate disk space access.
Thyroid cartilage overlap of disc spaces in the “prong deflector” group: observations at discography
No procedural complications were encountered in either the prong deflector or traditional cervical diskography groups. In the prong deflector group, a single attempted cervical disk space (C4–5) could not be engaged because of persistent obstruction by the thyroid cartilage related to unusual limitation of larynx displacement despite the prong deflector. This disk space was therefore not studied by diskography. In the traditional group, failed access at a single attempted cervical level (C4–5) was also encountered because of obstruction by thyroid cartilage, and this level was not studied. Therefore, a similar incidence of disk space access failure was encountered in both groups.
Postdiskogram CT Imaging
On postdiskogram CT imaging, thyroid cartilage or hyoid bone overlapped access to the cervical disks at C3–4 (17/22 [77%] levels imaged), C4–5 (27/28 [96%] levels studied), C5–6 (22/28 [78%] levels studied), and C6–7 (9/22 [41%] levels studied). Thyroid cartilage calcification was faint in 4/30 (13%) patients, likely affecting fluoroscopic recognition. In addition, the neurovascular sheath containing the carotid artery was positioned adjacent to the thyroid cartilage in 27/30 (90%) patients, most typically at the C4–5 and C5–6 levels (Fig 4).

Postdiskogram CT image in a 46-year-old woman with unrelenting neck pain radiating down both arms that demonstrates close proximity of the carotid artery and neurovascular sheath to thyroid cartilage (arrow) as is typically seen in most patients.
At the failed C4–5 level in the prong deflector group, postdiskogram CT images demonstrated a wide hyoid bone that significantly overlapped the anterior vertebral body of C4 (Fig 5), preventing displacement of the hyoid bone and thyroid cartilage and thus blocking the disk space. At the single failed C4–5 level in the traditional group, the thyroid cartilage was relatively wide and the right uncinate process significantly hypertrophic, obscuring disk space access.

Postdiskogram CT images in the 48-year-old man with chronic neck and right arm pain where difficulty was encountered in access to the C4–5 disk space despite attempted displacement of the larynx with the prong deflector tool. The hyoid bone is wide and the anterior aspect of the C4 vertebral body (black arrow) projects deeply into the gap between the hyoid cornua (arrowheads), preventing displacement of the hyoid and thyroid cartilages across the midline. Without hyoid and thyroid cartilage displacement, clear and safe access to the disk space could not be obtained.
Procedure Parameters
Fluoroscopy time, procedure time and sedation requirements are summarized in Table 3. Overall average fluoroscopy time was 1.7 minutes per cervical level examined. Fluoroscopy time per level was significantly lower in the prong deflector group (1.4 minutes) as compared with the traditional group (2.1 minutes). This likely reflected reduced time required for disk space access at any individual level in the prong deflector group. Sedation requirements and overall procedure time were similar in both groups with minor variation because of either number of levels studied per patient or time required for disk space access.
Procedure sedation, disc access and fluoroscopic time
Discussion
Cervical diskography is typically used in the complex patient to evaluate for significant disk-origin pain before surgery. Cervical disk surgery is most commonly performed for cervical radiculopathy and less frequently for spondolytic myelopathy (4). The targeted cervical disk spaces typically present with radicular pain along with a variable contribution from level specific evidence of root compression (distribution of pain pattern, weakness, deep-tendon reflex loss, and/or local sensory loss) and imaging evidence of level specific disk degenerative changes or disk herniation (4). The number of segments affected and presence or absence of instability influences the added use of interbody fusion and metallic hardware fixation (5).
Axial neck pain frequently accompanies this presentation but its response to surgical intervention is less certain (4). Studies focusing on cervical diskectomy for axial neck pain demonstrate excellent outcome results when objective testing is used to indicate the involved levels (6–11) Cervical diskography is the only available test that can directly challenge the disk space to determine whether the disk contributes to axial neck pain and target which levels are symptomatic (1, 2, 12). But cervical diskography is a challenging interventional spine technique with the carotid artery lying in the approach path and access to the disk spaces physically obstructed at many levels by the thyroid cartilage.
The prong deflector serves several helpful functions in performing cervical diskography. Typically, the procedure is performed with deflection of neck structures by the operator’s fingers with fluoroscopy used only for initial entry point determination and judgment of position of the needle tip in the deep neck (1, 2). Continuous or intermittent fluoroscopy is not usually performed because the operator’s hand and fingers remain in the fluoroscopic field. The prong permits intermittently fluoroscopic visualize of the needle while deflecting and securing the larynx and carotid artery. This allows the operator to make quick minor adjustments in needle trajectory during insertion with more rapid access the disk space and reduced patient fluoroscopic exposure. In addition, in light of the variability of thyroid cartilage calcification, visualization at fluoroscopy is often difficult and displacement of the cartilage with the prong helps with its identification. Fluoroscopy is also important to observe the course and ultimate end point of the needle. Although the initial trajectory can be directed medial to Lushka’s joint, direct visualization with larynx deflection by the prong is helpful to avoid the neural foramen and the vertebral artery (3). Ultimately, proper positioning in the disk space is important, and it is critical not to enter the spinal canal and cervical cord.
The prong is also helpful in limiting motion of the pharynx. When a cervical disk space is engaged, the spinal needle frequently courses adjacent to the pharynx, and significant needle motion with patient swallowing can present difficulties in disk access. Through firm but persistent pressure, swallowing is restricted by the prong and unwanted errant needle motion minimized during needle insertion.
New technical approaches to the cervical disk spaces may affect the importance of cervical diskography. Disk replacement prosthetics or the recently improved percutaneous diskectomy devices could ultimately be directed at disk origin pain in the cervical spine. Accurate targeting of the affected painful disk spaces will be essential in proper selection of patients for this procedure.
Conclusion
The prong deflector tool is useful in improving access to the cervical disk spaces for cervical diskography. The tool assists in controlled displacement of the carotid artery and thyroid cartilages while allowing intermittent fluoroscopic visualization of the needle during insertion without direct operator radiation exposure. The prong helps stabilize pharyngeal motion and reduce or eliminate needle deflection caused by patient swallowing. Fluoroscopy time per cervical level studied is markedly reduced secondary to more rapid disk space access.
- Received November 22, 2004.
- Accepted after revision January 5, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.