
Dynamic brain stem compression due to unsuspected Chiari malformation (CM) may mimic a meningeal process and can pose a diagnostic challenge to both the neuroradiologist and the clinician. CM usually goes undetected on the axial CT examination, where severe beam hardening creates difficulty in evaluating the craniocervical junction (Fig 1). In the setting of CM, the craniospinal pressure dissociation can be worsened if CSF is removed from the spinal canal.
A 23-year-old woman with a clinical diagnosis of Ehlers-Danlos syndrome presented to our emergency room (ER) with increasing nausea, vomiting, and what she described as the worst headache of her life, which radiated to the skull base. There were no visual symptoms or cranial nerve dysfunction. A nonenhanced CT brain study was reported as normal. The patient underwent lumbar puncture (LP) in the ER to exclude subarachnoid hemorrhage. Approximately 14 mL of clear, colorless CSF was removed. The CSF pressures were 21 cm of water on opening and 13 on closing. There were no immediate complications from the LP. She was transferred to the medical ward in a stable condition. Ten hours after the LP, the patient experienced acute worsening of her initial symptoms and had a witnessed episode of apnea lasting 20 seconds. She fully recovered from the episode without any sequela. CM was diagnosed later that afternoon on an MR imaging study, which showed significant stenosis of the foramen magnum evidenced by complete obliteration of the CSF (Fig 2). No focal lesion or abnormal signal intensity was seen in the brain stem.
In a previously reported case of acquired CM, declining visual function was described after placement of a lumboperitoneal shunt. The condition improved after ventriculoperitoneal shunt surgery (1). Clinically, CM is not regarded as an absolute contraindication for an LP. In our patient, it was difficult to establish a definite correlation between the LP and the acute clinical episode described 10 hours later, although there was concern for a causal relationship between the two events. The response to an LP likely depends on the degree of tonsillar herniation and the amount of CSF removed. In our institution, opinion of whether to proceed with LP in the setting of known CM was divided among the clinical staff (neurologists and neurosurgeons). Life-threatening conditions such as subarachnoid hemorrhage or meningitis will always be strong justifications for the LP. In known cases of CM, better visualization of the craniocervical junction with MR imaging should probably be attempted to assess the severity of compromise at the foramen magnum. For undiagnosed cases, the radiologist needs to remain vigilant, because CT will likely remain the standard imaging technique before the LP. High index of clinical suspicion for dynamic brain stem compression remains the key factor for accurate detection of CM by imaging studies.
It is difficult to predict the true incidence of this presentation and its medicolegal implications. We would be interested in the experiences of others in this particular situation.

Axial CT image at the level of foramen magnum. It is difficult to visualize the true extent of foramen magnum crowding, because of beam-hardening artifact.
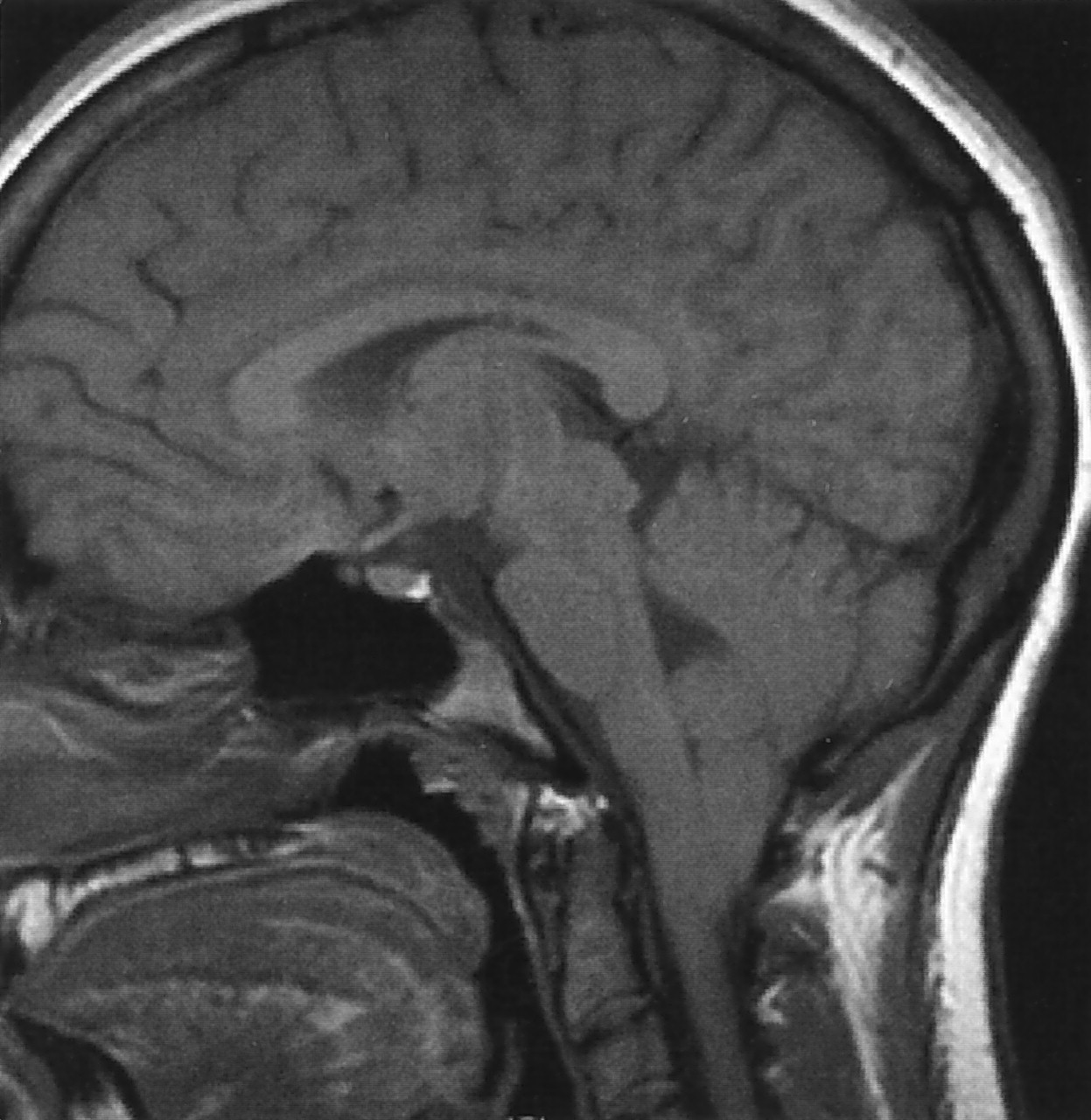
Sagittal T1-weighted image (TR/TE, 500/4 ms) reveals severe inferior herniation of cerebellar tonsils into the upper cervical canal effacing the CSF at the foramen magnum.
- American Society of Neuroradiology





{kind=link}
{kind=link}