
Abstract
Summary: We describe two cases of hypothalamic hamartoma associated with arachnoid cysts. One case was initially documented on prenatal MR images. Because of the rarity of the association and resultant distortion in regional anatomy, the solid component of the mass may be overlooked. This would certainly be true when using lower-resolution diagnostic studies such as fetal MR imaging. The lesion could also be confused with a cystic tumor such as pilocytic astrocytoma. Thorough evaluation is required in patients with precocious puberty, gelastic seizures, and the presence of a suprasellar arachnoid cyst.
Hypothalamic hamartomas are benign tumors consisting of ectopic neural tissue presumably congenital in origin. A hypothalamic hamartoma is typically a solid, nonenhancing mass that has similar MR signal intensity characteristics to those of gray matter (1–3). Associated cystic components have been described but are rare (4–7). We report two patients with hypothalamic hamartomas associated with arachnoid cysts, including one with prenatal MR imaging. This confirms that these lesions form in utero. To the best of our knowledge, prenatal depiction by MR imaging has not been reported.
Case Reports
Case 1
A 16-month-old female patient presented with vaginal bleeding. Physical examination revealed accelerated sexual maturation (Tanner stage II) with breast development and pubic hair. MR imaging done at 1.5 T by using standard T1-, T2-, and gadolinium-enhanced T1-weighted sequences showed a solid lesion that was nearly isointense relative to cortex on all images and did not enhance. The nodule projected into the prepontine cistern. There was an associated cyst, which appeared to be arising from the floor of the third ventricle (Fig 1). No additional intracranial abnormalities were present. Depo-lupron was administered to halt further development of secondary sexual characteristics. The nodule was felt to be remote from the floor of the third ventricle, so surgical resection was attempted. Pathologic analysis revealed scattered neurons and normal glial cells in the solid portion of the tumor consistent with a hypothalamic hamartoma. Histologic evaluation of the cyst wall showed glial and meningeal components.
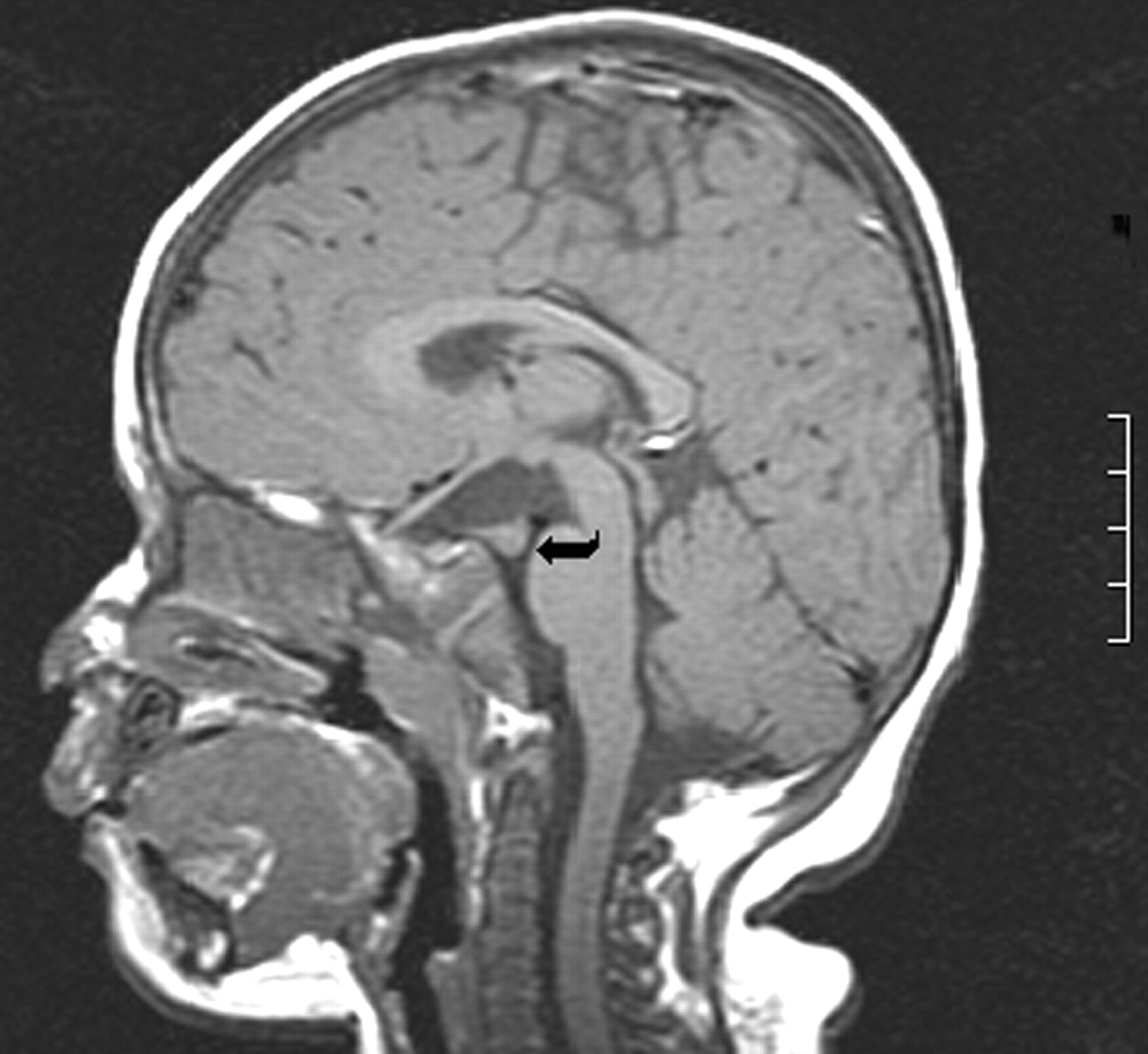
Case 1. Nonenhanced sagittal T1-weighted image (460/11/2 [TR/TE/NEX]). A solid-appearing nodule projects into the prepontine cistern on the right (curved arrow). The nodule is isointense relative to cortex. No enhancement is present after contrast medium administration (not shown).
Case 2
A 20-year-old gravida 1, para 1 female patient was referred for fetal MR imaging after sonography showed an enlarged head circumference, ventriculomegaly, and a midline defect. Fetal MR imaging with heavily T2-weighted single-shot spin-echo (SE) sequences revealed an anterior suprasellar soft tissue lesion with cysts in the suprasellar and prepontine cisterns as well as extension into both middle cranial fossae (Fig 2A and B). The patient was delivered at term by cesarean section and was neurologically intact. Head circumference was enlarged at 38.5 cm (95th percentile). Postnatal MR imaging was performed at 1 month by using T1-weighted SE, T2-weighted fast SE, gadolinium-enhanced T1-weighted SE, and diffusion-weighted images. Extension of extra-axial fluid collections of high signal intensity, which were presumably arachnoid cysts, extended into both middle cranial fossa and elevated the floor of the third ventricle. The third and lateral ventricles were enlarged. The solid portion of the mass was suprasellar, isointense relative to cortex, and demonstrated no enhancement after gadolinium administration (Fig 2C). No additional intracranial malformations were visible, and the corpus callosum and pituitary gland appeared normal. Surgery was performed to decompress the cystic portion of the mass while biopsy of the solid component was carried out. Pathologic analysis revealed scattered neurons and normal glial cells within the solid portion of the mass. No cellular atypia was noted, and the MIB-1 index was low. The cyst wall consisted of meninges on one side and glial cells on the other.
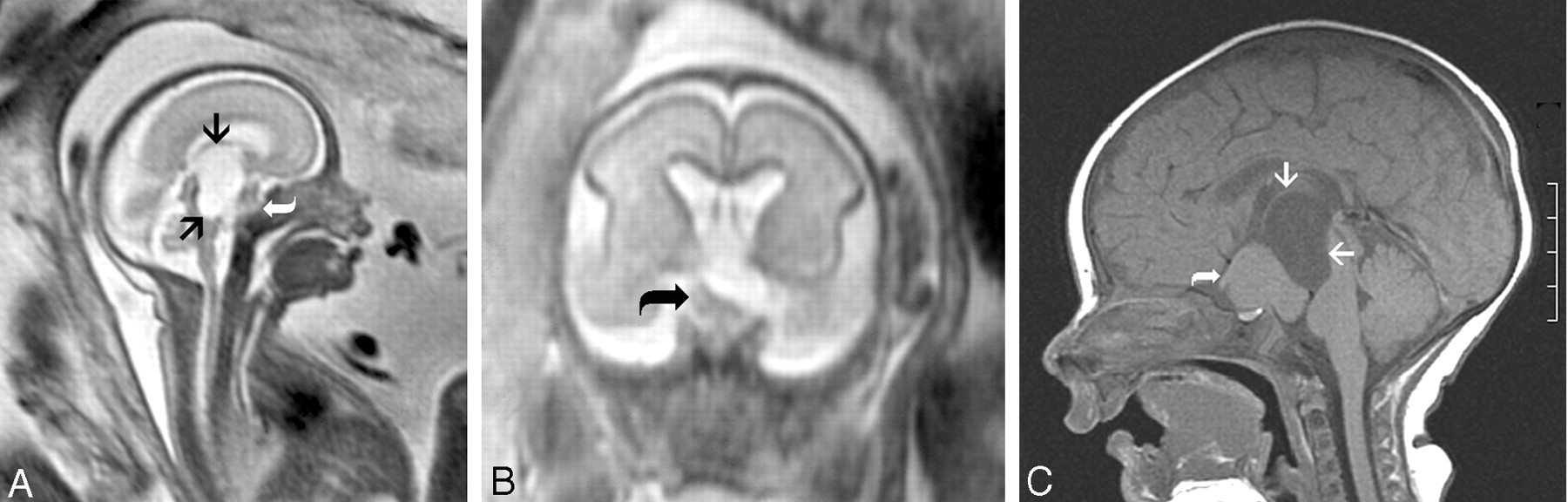
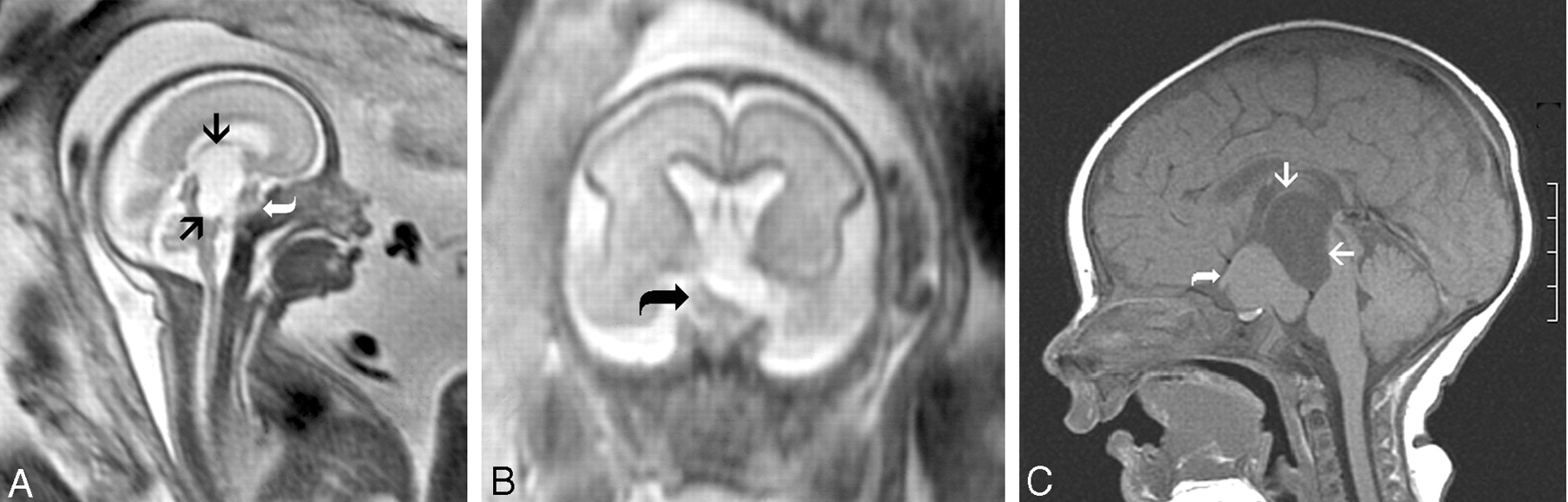
Case 2. Pre- (A and B) and postnatal (C) MR images.
A and B, Sagittal and coronal single-shot rapid acquisition SE images (∞/60–80). A mass isointense relative to cortex is present within the suprasellar cistern (curved arrow). High-signal-intensity fluid-filled cysts project superiorly and posteriorly (arrows). There is elevation of the floor of the third ventricle and compression of the midbrain and pons.
C, Nonenhanced sagittal T1-weighted image (450/11/2). The nodule is isointense relative to cortex and lies in the suprasellar cistern (curved arrow). Associated fluid-filled cysts are of high signal intensity (arrows). No enhancement is present after contrast medium administration (not shown).
Discussion
A hypothalamic hamartoma arises from the region of the tuber cinereum and is commonly associated with isosexual precocious puberty. Efferent pathways that allow modulation of gonadotropins and contain releasing hormones and secretory granules are present within the floor of the third ventricle (8). Precocious puberty may either result from a physical pertubation of inhibitory pathways by the hamartoma or, more likely, are a direct neurosecretory process of the hamartoma itself (9). Although MR imaging findings are usually normal in patients with isosexual precocious puberty, a hypothalamic hamartoma is the most common identifiable abnormality. Differential diagnosis includes hypothalamic and chiasmatic glioma, germ cell tumor, arachnoid cyst in the absence of a hamartoma, and isolated hydrocephalus (10, 11). Only one of our patients presented with central isosexual precocious puberty.
Seizure activity, most commonly described as gelastic, is the other common clinical presentation in children with a hypothalamic hamartoma. Theories for the pathogenesis of seizures are either connections with the limbic system and subsequent propagation of the seizure activity or possibly the presence of associated malformations (12). Neither of our patients had seizures. In the literature, one patient with a hamartoma and arachnoid cyst did present with seizures of temporal lobe origin (6).
This report describes the first case of a hypothalamic hamartoma seen by use of fetal MR imaging. This directly confirms that hamartomas form in utero before 26 weeks’ gestation. Because of the known association with other congenital anomalies of the central nervous system, hypothalamic hamartoma is thought to form as early as 4 weeks and may in fact be part of a developmental anomaly spectrum (12, 13). Two theories have been proposed to explain the coexistence of an arachnoid cyst and a hypothalamic hamartoma. The formation of the subarachnoid space begins at 14 weeks with the intracellular space expanding as the meninx privativa degenerates. The space is first seen ventral to the mesoencephalon, which would include the suprasellar cistern (14). The presence of the hamartoma may disrupt the formation of the subarachnoid space leading to the formation of an arachnoid cyst. Alternatively, arachnoid or meningeal tissue could be within the hamartoma, resulting in the formation of an associated arachnoid cyst (4, 6).
MR imaging has been proved to be the optimal imaging study for evaluating the presence of hypothalamic hamartomas. The lesions are isointense on T1-weighted images and iso- to more commonly slightly hyperintense on T2-weighted images and do not enhance (1–3). The presence of increased T2 signal intensity and progressive growth may suggest malignant transformation or, more likely, a different tumor. Hypothalamic hamartomas are usually small and may be sessile or pedunculated. Pedunculated and smaller lesions tend to present with precocious puberty, whereas sessile and larger lesions are more commonly associated with seizures (15). MR spectroscopy has shown increased concentration of myo-inositol and relatively normal n-acetylaspartate and choline levels (16).
Atypical features of hypothalamic hamartomas have been reported in the literature and include giant hamartomas, lipomatous content, cystic necrosis, and prominent T2 prolongation (17–20). An arachnoid cyst is rarely reported in association with a hypothalamic hamartoma with, to the best of our knowledge, only four previous cases in the literature (4–7). The development of a hypothalamic hamartoma has been closely associated with duplication of the pituitary gland. The presence of a hamartoma has been attributed to abnormal splitting of the rostral notochord, which explains the association with pituitary duplication and the duplicated floor of the third ventricle and aqueduct. Early insults may lead to abnormal development of the facial structures (13). Normal pituitary glands and facial development were present in both our patients. Additional associated congenital abnormalities of the olfactory tracts, corpus callosum, cerebral cortex, and posterior fossa have been described (14, 21, 22).
The presence of prominent cysts associated with a hamartoma can lead to significant alteration in regional anatomy and incorrect preoperative diagnosis, especially in the absence of a typical clinical presentation. The presumptive diagnosis of hamartoma associated with arachnoid cysts should be made when MR imaging features of the solid component are typical for a hypothalamic hamartoma. These features should be sought in any patient presenting with precocious puberty or seizures and the presence of a suprasellar arachnoid cyst. Even in the absence of a typical clinical presentation, as was the case in one of our patients, an arachnoid cyst may be associated with a hamartoma. Arachnoid cysts and their association with precocious puberty are well documented in the literature. We suggest careful evaluation of every suprasellar arachnoid cyst for the presence of associated an associated hamartoma, particularly in prenatal MR imaging.
Footnotes
Presented at the 41st Annual Meeting of the American Society of Neuroradiology, April 28–May 2, 2003; Washington, D.C.
References
- Received August 28, 2003.
- Accepted after revision November 18, 2003.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}