
Abstract
Summary: A 75-year-old Asian man presented with two episodes of chorea associated with nonketotic hyperglycemia. His chorea rapidly resolved after restitution of a normal serum glucose level, although an MR image obtained at the time of acute symptoms demonstrated high signal intensity on T1-weighted images, low signal intensity on T2-weighted images, and restricted diffusion, all involving the left putamen. A CT scan obtained 1 month later demonstrated faint hyperattenuation of the involved putamen. The reported pathophysiologic considerations for these imaging features are reviewed, and an original explanation is proposed.
Abnormalities of the putamen on CT and MR images have been reported elsewhere (1–4) as being associated with new-onset chorea, typically in elderly Asian patients (1). It has been most often reported among diabetic patients with nonketotic hyperglycemia (2). The process is either unilateral or bilateral. If unilateral, the imaging findings are typically contralateral to the symptomatic body side (2). The pathophysiologic mechanisms underlying the imaging findings remain controversial (2–4). High signal intensity on T1-weighted and low signal intensity on T2-weighted images is consistent with petechial hemorrhage or microcalcifications, although the latter is thought less likely because the imaging findings have been reported to resolve within a few months in some cases (2). Some authors (2) have suggested that the imaging findings are secondary to myelin destruction and the presence of myelin breakdown products, whereas others assert that the imaging changes are related to hyperviscosity (4), accounting for the lowering of the diffusion coefficients.
Case Reports
A 75-year-old Asian man was seen in the emergency room of our institution with right-sided chorea that had developed 2 days before admission. The patient had been treated for diabetes mellitus type II for 1 year and for hypertension for the prior 2 years. His serum glucose on admission was 694 mg/dL (normal values, 70–199 mg/dL). There were no ketones in the serum, and the calculated serum osmolarity was 298 mOsm/kg. No family history of movement disorders was elicited, nor was the patient taking medication such as neuroleptic drugs that could cause chorea. Other causes of chorea, such as thyroid disease, were also excluded. MR imaging of the brain was performed to rule out stroke. The left putamen was hyperintense on T1-weighted images (Fig 1A) and hypointense on T2-weighted (Fig 1B) and fluid-attenuated inversion recovery (FLAIR) images (Fig 1C). The anterior limb of the left internal capsule was spared. The apparent diffusion coefficients (ADCs) were low in the left putamen (0.58 ± 0.13 × 10−3 mm2/s versus 0.82 ± 0.18 × 10−3 mm2/s for the normal contralateral side). The left putamen appeared hyperintense on the exponential diffusion-weighted (DW) images (b = 1000 s/mm2 images divided by b = 0 s/mm2 images [5]; Fig 1D) and hypointense on the ADC maps (Fig 1E). A subtle focus of reduced ADC was possibly present in the posterior portion of the right putamen. A lipoma of the corpus callosum was incidentally noted. The chorea rapidly resolved after restoration of a normal serum glucose level, and the patient was followed up as an outpatient.

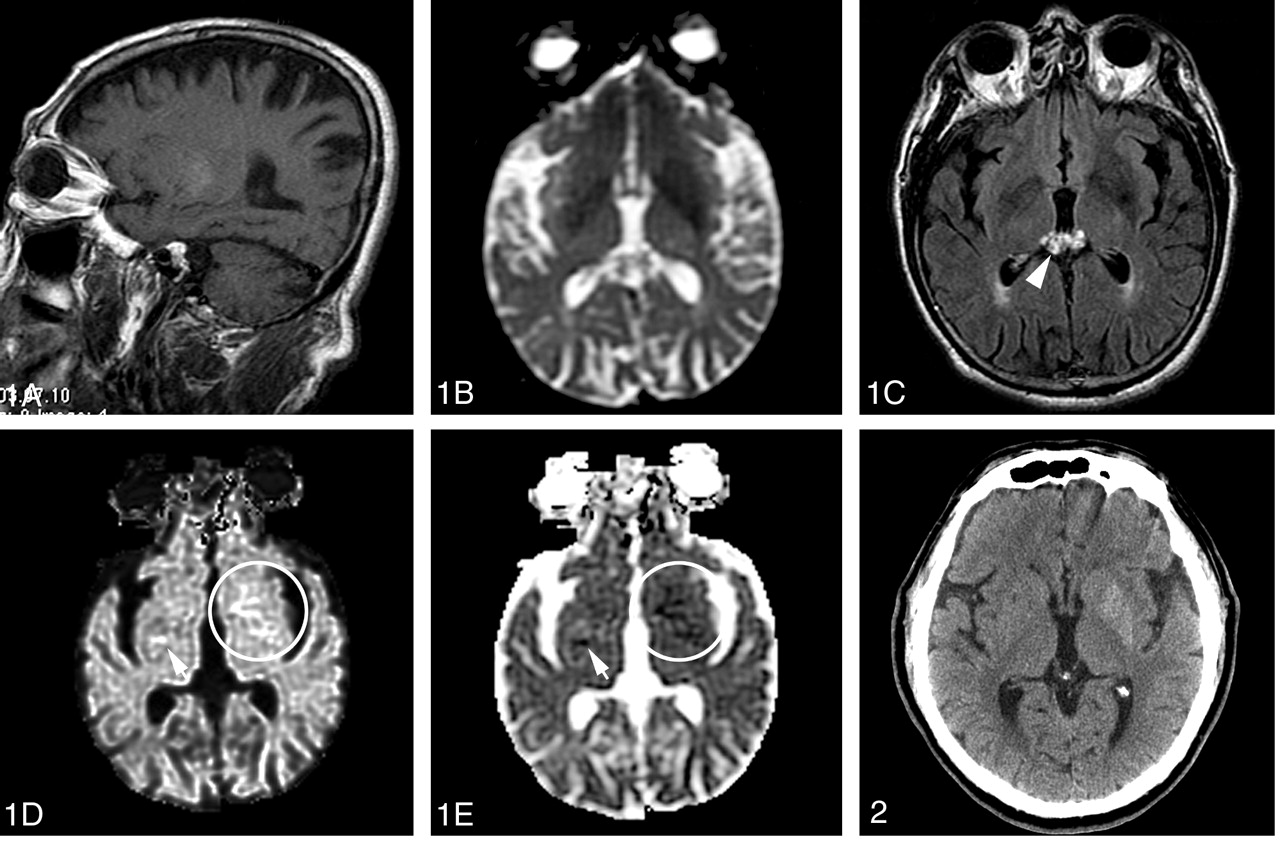
MR images of the brain obtained during the patient’s first admission. The left putamen is hyperintense on T1-weighted images (A) and hypointense on T2-weighted (B) and FLAIR images (C). The left putamen (circles [D and E]) appears hyperintense on the exponential DW images (b = 1000-s/mm2 images divided by b = 0-s/mm2 images [5]) (D) and hypointense on the ADC maps (E). A subtle focus of reduced ADC is also present in the posterior aspect of the right putamen (arrows). Lipoma of the corpus callosum is incidentally noted (C, arrowhead).
One month later, however, the patient was readmitted with the same symptoms of unilateral chorea. His serum glucose on admission was then 547 mg/dL. A noncontrast cranial CT obtained at that time showed no sign of brain ischemia. Instead, the entire left putamen demonstrated faint hyperattenuation, without evidence of mass effect, edema, or volume loss (Fig 2). Again, his symptoms resolved 2 days later, after stabilization of his serum glucose level. The patient was discharged at his request and returned home.

Noncontrast cranial CT scan obtained during the patient’s second admission shows faint hyperattenuation of the entire left putamen, without evidence of mass effect, edema, or volume loss and with no sign of brain ischemia.
Discussion
Without a follow-up imaging study of our patient, it is impossible to ascertain whether the CT hyperattenuation resolved and whether it corresponded to blood or calcification. Whether the substrate to the CT hyperattenuation was present at the time of the initial MR imaging is also impossible to determine, because they were obtained 1 month apart. It may have been present, accounting for the T1 hyperintensity and the T2 and FLAIR hypointensity. (Note that a lenticular T1 hyperintensity may be encountered in healthy subjects, but not T2 and FLAIR hypointensities.) There was, however, no evidence of significant susceptibility on the DW images obtained with a b value of 0 s/mm2 that would suggest the presence of either calcium deposit or hemorrhagic products. Nonetheless, restricted diffusion is not accounted for by blood or calcification. Conversely, ischemia or hyperviscosity may explain the restricted diffusion, but neither of these hypotheses is consistent with the CT hyperattenuation observed 1 month later. None of the reported pathophysiologic considerations of the CT attenuation changes and MR signal intensity changes (changes in water content or viscosity or both, myelin breakdown products, blood products, and deposition of calcium and other minerals) is completely satisfactory. One possible explanation could be acute putaminal dysfunction, secondary to hyperglycemic or hyperosmolar insult and featuring restricted diffusion. This functional alteration could be associated with some degree of Wallerian degeneration of the internal white matter of the putamen. Protein desiccation occurring in the course of Wallerian degeneration could explain the CT hyperattenuation and the MR and DW imaging patterns in the early phase (6, 7), as well as the variable evolution of imaging features with time.
Unilateral putaminal CT hyperattenuation, MR signal intensity abnormality, and restricted diffusion in the setting of nonketotic hyperglycemia together are an entity to be recognized and distinguished from acute ischemic stroke in patients with acute neurologic symptoms. Although nonketotic hyperglycemia mimics stroke in clinical presentation and DW imaging findings, the pathophysiologic mechanisms of this entity are not clearly ischemic, which may affect treatment options.
References
- Received September 8, 2003.
- Accepted after revision October 29, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Diabetic striatopathy: a rare condition and diagnostic dilemma
- Hyperglycaemic chorea-ballism or unmasking of Huntingtons chorea in a patient with diabetes
- Unilateral striatal CT and MRI changes secondary to non-ketotic hyperglycaemia
- Neuroimaging in Patients with Abnormal Blood Glucose Levels
- Non-ketotic hyperglycaemia hemichorea-hemiballismus and acute ischaemic stroke
- Diagnostic approach to restricted-diffusion patterns on MR imaging