
Abstract
Summary: A case of acute subdural hematoma over the tentorium secondary to rupture of an anterior communicating artery aneurysm is reported. A 42-year-old female patient presented with acute-onset, severe bifrontal and retro-orbital headache. CT revealed only symmetric thickening of the tentorium. MR imaging revealed the presence of a 10-mm anterior communicating artery aneurysm, which was confirmed by digital subtraction angiography. The radiologic findings and possible mechanisms of this hemorrhage are discussed.
Approximately 3% of ruptures of intracranial aneurysms result in subdural hematomas. Seventy percent of these aneurysms arise from either the internal carotid artery or the middle cerebral artery. Subdural hematoma from intracranial aneurysm rupture without radiographic evidence of subarachnoid hemorrhage, however, is rare.
Case Report
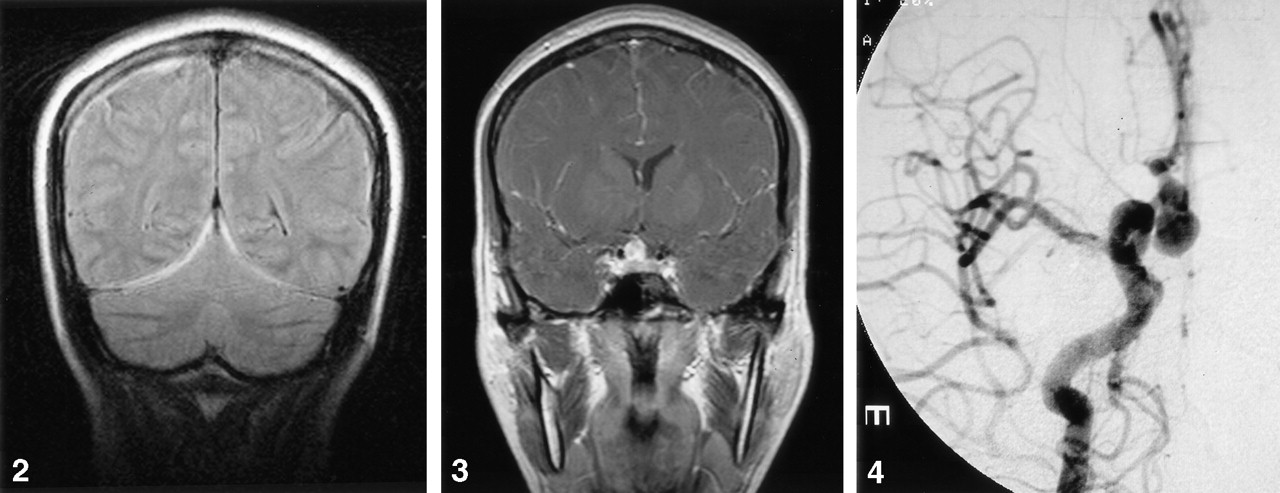
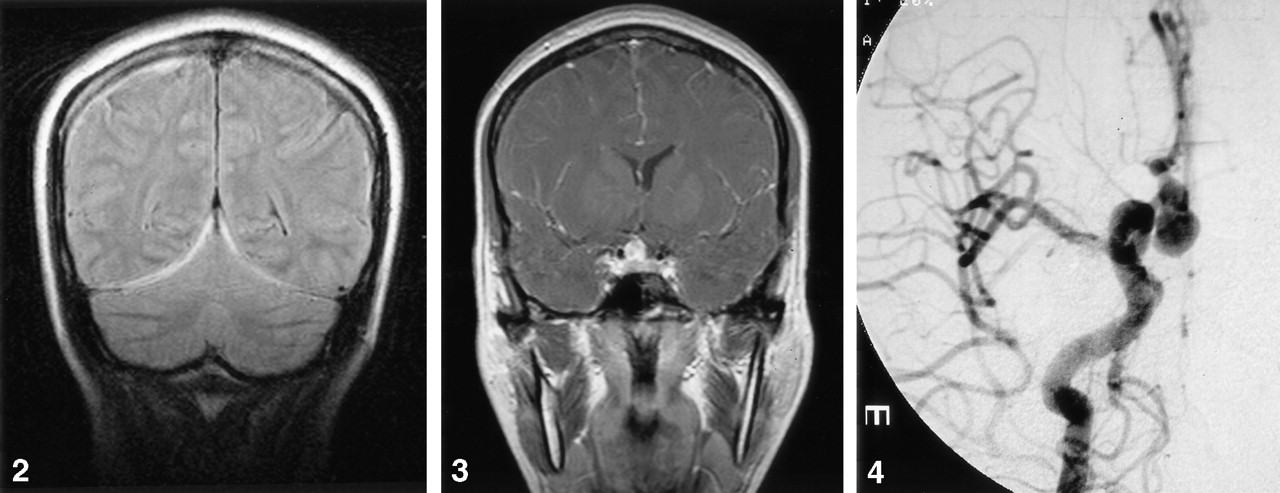
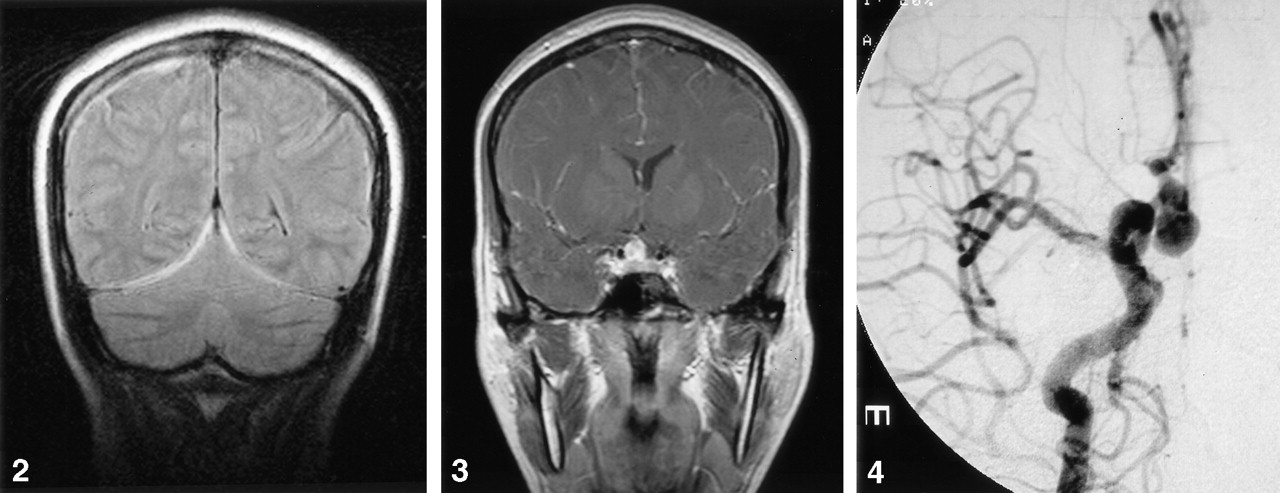
A 42-year-old, right-handed female patient with a history of hypertension presented to the emergency department reporting sudden-onset, severe headache approximately 4 hours before admission. The headache was described as bilateral and retro-orbital in location and was associated with photophobia, nausea, and lightheadedness. The patient reported having had mild headache on each of the 4 days before admission as well as a similar episode of severe headache 3 months before admission, all of which had been treated with oral analgesic medications. Upon admission, the patient was sleepy but easily arousable and was oriented to person, place, and time. Her pupils were equal and reactive, and there was no meningismus. Her reflexes were equal and symmetric with plantar flexion of the toes. Noncontrast cranial CT revealed diffuse thickening and increased attenuation of the tentorium cerebelli bilaterally (Fig 1). MR imaging revealed the presence of a 3-mm extra-axial collection extending from the tentorium symmetrically to envelop both cerebral hemispheres, as well as a collection dorsal to the clivus extending inferiorly below the foramen magnum. This collection was isointense relative to brain on T1-weighted images and hyperintense on T2-weighted MR images (Fig 2). These findings were interpreted as consistent with acute subdural hematoma (SDH). No evidence of subarachnoid hemorrhage was noted on either CT or MR images. MR angiography (MRA) and subsequent conventional angiography showed the presence of a 10-mm anterior communicating artery aneurysm extending inferiorly and posteriorly from its parent vessel (Fig 3). No vasospasm was present (Fig 4). Lumbar puncture was performed 2 days after admission. CSF analysis revealed an rbc of 28,000/μL, a wbc of 80/μL, protein of 651 mg/dL, and glucose of 78 mg/dL; however, no xanthochromia was seen. Surgery was performed 6 days after admission. Intraoperatively, an anterior communicating artery aneurysm extending inferiorly with the dome embedded anteriorly in the optic chiasm was identified and a clip placed therein. The patient also had a large amount of subdural blood overlying the convexity under the craniotomy that was irrigated with lactated ringers and evacuated. No evidence of subarachnoid blood was seen intraoperatively. She awoke from surgery with no neurologic deficits and had an uneventful convalescence.

Axial noncontrast CT scans show thickening of the tentorium bilaterally and no evidence of subarachnoid hemorrhage.

Coronal FLAIR MR image reveals hyperintensities along the tentorium consistent with acute blood.

Coronal T1-weighted MR image reveals enhancing suprasellar mass consistent with an anterior communicating artery aneurysm.

Submentovertex view of a right internal carotid artery-injection cerebral angiogram reveals a 10-mm anterior communicating artery aneurysm.
Discussion
Although the incidence of acute SDH secondary to intradural aneurysm rupture is well documented, occurring in 0.5–7.9% of all cases, acute SDH without radiologic evidence of SAH is rare (1–4). Only 150 cases of SDH without SAH have been reported in the literature since 1855 (5). Only three describe hematomas of the tentorium, all of which resulted from ruptures of internal carotid artery aneurysms (6). This case appears to be the first in the literature to describe a tentorial SDH from an aneurysm arising from the anterior communicating artery. Two possible mechanisms for the development of SDH associated with aneurysm rupture have been proposed in the literature (1, 3, 4, 6). One theory suggests the force of the rupture results in a tearing of the arachnoid with subsequent spilling of blood into the subdural space. The second proposes that one or more “sentinel” hemorrhages result in the formation of adhesions between the aneurysm and the arachnoid, creating a path for blood to enter the subdural space with subsequent rupture. The history of headaches 3 months before ictus in this case may represent a prior rupture. Furthermore, the adhesions from the aneurysm to the optic chiasm would support the theory of previous hemorrhage. Although this appears to be the first report of an aneurysm in this location causing a tentorial SDH, there have undoubtedly been other cases that have gone undiagnosed. In this case, the unusual pattern of the SDH, along with the history, led to MRA, which yielded the diagnosis. With the continuing advancement of MR imaging technology and more widespread use of MRA and CT angiography, perhaps more cases of SDH without SAH from aneurysm rupture will be diagnosed.
- Received August 6, 2003.
- Accepted after revision September 23, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.