
The phrase “vertebroplasty versus kyphoplasty” evokes images of competitive procedures and groups of entrenched physicians locked in battle. Our involvement in the development and introduction of percutaneous vertebroplasty (PV) and kyphoplasty (KP) in the United States has given us a unique perspective on the safety and efficacy of both procedures. We feel that PV and KP both offer potential benefit with acceptable safety when used by skilled physicians. The real hurdles now are to further assess and develop the appropriate indications, advantages, and shortcomings of each procedure. We must then select the appropriate method of therapy to maximally benefit our patients. Finally, all practitioners must venture beyond the dogma of their respective subspecialties and understand the full spectrum of tools and techniques that are available to treat vertebral compression fractures.
History
The history of the development of each procedure explains how a competitive environment has arisen between PV and KP, as with many of the physicians that utilize them. PV had its introduction in France, in 1984, by the interventional neuroradiologist Hervé Deramond (1). It was found useful for the treatment of pain associated with vertebral fracture resulting from benign and malignant tumors, as well as osteoporotic compression fractures (1, 2). Neuroradiologists in the United States began to use the technique in 1993, and the first U.S. case series reported was in 1997 (3). It has remained popular in the radiologic community.
Since the early clinical work, many reports have documented the biomechanical effects of PV and the pain relief resulting from this treatment for vertebral compression fractures (1–3, 7–21). A review of this literature shows that all reports reveal favorable results of pain relief and restoration of activities of daily living following PV. (A prospective, randomized series comparing PV to alternative therapy, however, has not yet been accomplished.) Clinical complications are rare in the hands of experienced operators. Some studies do report a higher risk of complications in patients with malignant disease, which includes myeloma and osteolytic metastases (myeloma is thought to be less risky than osteolytic malignancy).
The idea of attempting to treat a vertebral compression fracture with an inflatable balloon tamp (and thereby restore the vertebral body height and minimize the associated kyphotic deformity) was conceived by an orthopedic surgeon, Dr. Mark Reiley, in the early 1990s. The initial biomechanical investigations of the Kyphx inflatable balloon tamp (Kyphon Corporation, Sunnyvale, CA) were performed as a combined effort by this orthopedic surgeon and a neuroradiologist familiar with PV (4–6). The device was given 510k approval by the U.S. Food and Drug Administration as a “bone tamp.” A randomized clinical trial that compared “kyphoplasty” to conservative medical management was attempted, but patient entry was slow and this initiative was ultimately abandoned in favor of a clinical registry tabulating the results of patients treated with KP. Thus, like PV, KP has not been tested in a comparison trial against conservative therapy. There are only a few peer-reviewed studies available to judge safety and efficacy of KP (22, 23). Case reports and opinion papers are also found, although they are few in number (24–28).
In one study, pain relief was found to be similar to that observed with PV, and the perioperative complication rate was 10%, though no complications related to the procedure were claimed by the authors (22). An asymptomatic cement leak rate of 8.5% was observed. The authors enthusiastically reported height restoration, but analysis of their data reveals that the average height gained per vertebra treated was 3 mm at the center of vertebral endplate. This leaves open for debate the effectiveness of the KP procedure for predictably restoring vertebral height in vertebral compression fractures.
In another early series, all 15 patients who underwent 24 uncomplicated KP procedures for osteoporotic vertebral compression fractures that were present for an average duration of 14 weeks experienced immediate pain relief (23). The mean height restoration as measured on lateral radiographs was 1.5 mm in the posterior vertebral body, 4.7 mm in the midvertebral body, and 3.7 mm in the anterior vertebral body. In a larger series of 226 consecutive KP procedures, similar results with respect to height restoration were reported (24). A 1% complication rate in this series included one case of epidural hematoma that required surgical decompression, one case of spinal cord injury, and one case with transient adult respiratory distress syndrome. A multicenter registry of 1,439 patients with 2,194 treated fractures with KP showed an efficacy of 90% with respect to pain relief and a major complication rate of 0.2% per fracture (25).
Only one report is available with respect to KP as a treatment of pathologic vertebral compression fractures. In a series of 18 patients with multiple myeloma who underwent 55 uncomplicated KP procedures, significant pain relief was achieved in all patients (26). Height restoration was only reported in 39 treated levels and was listed as 34% (leaving in doubt the validity of this measurement for the entire treatment group).
The initial reports and editorials concerning KP were generated primarily in the orthopedic literature and reflected an unqualified, positive opinion. Some of this literature seemed simply to echo marketing statements that were, as yet, unproved by clinical or laboratory investigation. The procedure, however, was not as well received in the radiologic community. This initial difference of opinion has not been substantially altered. KP has flourished in the surgical community, a group that has directly benefited from extensive marketing and educational support. Its members tend to see KP as a potential “high-dollar” replacement for PV. There has been growing competition for patients between the two groups that favor one or the other of these two procedures. Unfortunately, the competitive environment between radiologists and surgeons has been compounded by limited access to KP training courses for radiologists.
Substantial differences exist in the cost of PV and KP. The KP kit (without bone cement) is approximately $3,400, whereas a PV kit (with bone cement) is less than $400. Although not a requirement of the procedure, KP is often performed in the operating room with general anesthesia. The patients may be kept overnight in the hospital for observation. PV is usually performed with intravenous sedation only and a brief period of observation followed by discharge home after the procedure. All of these differences combine to make KP cost 10–20 times more than PV. This cost difference is acceptable only if there are proved, substantial positive benefits for the more expensive procedure. KP marketing claims that these benefits include improved safety because of fewer symptomatic cement leaks and substantial height restoration with kyphosis reduction that might improve pulmonary and gastrointestinal function. Actual published data that address these claims directly are sparse, but an attempt here is made to compare and contrast results based on that information.
Jargon versus Reality
It seems that most physicians would agree that both PV and KP relieve the pain associated with vertebral compression fractures. This would seem logical, because KP relies on the same vertebral stabilization principal used in PV, the introduction of bone cement into a compromised vertebra. KP is even sometimes referred to as “balloon-assisted vertebroplasty” (29). Biomechanical data comparing the mechanical stabilization by PV and KP show similar results (4).
Beyond these basics, reality seems to be blurred by the jargon. Manufacturers and champions of any device describe their individual advantages. This has been no less true of KP proponents, who routinely point out the reduced likelihood for cement leaks with this procedure compared with PV (30). This is alleged to occur because the injection of cement in PV is purportedly under “high pressure,” whereas KP fills a void created by the bone tamp and is therefore “low pressure.” For years this marketing-driven claim went unchallenged and is often repeated by physicians even though no scientific data existed that actually measured or compared the injection pressures with these devices. Recently, one group of investigators demonstrated quantitatively that, under usual operating conditions, “high-pressure” injections were not observed with any of these percutaneous vertebral fracture reduction procedures. In fact, the variables that seemed to influence intravertebral pressure measurements were the rate of injection and the size of the cannula. Higher intravertebral pressures were recorded with higher injection rates, larger bore systems, and when a metal trocar was used to drive cement through the cannula (31).
Lieberman et al reported a cement leak rate during KP of 8.6% (22). Fortunately, as with PV, most cement leaks were asymptomatic. KP reports have noted a very high cement leak incidence with PV, but they have failed to distinguish between symptomatic and asymptomatic leaks. When this is done, little difference seems to exist between the two procedures. Symptomatic cement leaks have occurred with both procedures (39) (Figs 1 and 2). Concern for patient safety prompted the FDA to issue a warning regarding the use of polymethylmethacrylate in both PV and KP in April 2003 (32).

CT scan of a thoracic vertebra following KP. There was a lateral blowout fracture of the vertebra caused by balloon inflation and a large cement leak (arrow) into the mediastinum. The patient had severe pain requiring hospitalization and protracted analgesic therapy for weeks following therapy. (From JM Mathis. Percutaneous vertebroplasty. AJNR Am J Neuroradiol 2003; 24:1697–1706; by permission.)

Radiograph following PV and KP, showing small, asymptomatic cement leaks at both levels. The PV level (above) had a small cement leak into an adjacent vein (arrows). The KP level (below) had small cement leaks into both adjacent disk levels (arrowheads).
Even in vitro, the capability of KP to reliably produce height restoration in fractures and compressed vertebral bodies remains controversial (Fig 3). Biomechanical evaluations by Belkoff and Mathis reported “significant” height restoration with KP compared with PV (5). Their investigation, however, looked only at vertebra that had a maximum height loss of 25%. PV was noted to experience height recovery, but less than KP. The actual height gain difference achieved by KP was on the order of 3 mm. Unfortunately, no in vitro investigations are available that determine whether this effect can be achieved, without destroying the vertebra, when compression is more severe that 25%. Indeed, Lieberman et al’s data, which show an average height restoration of approximately 3 mm per vertebra treated, suggest that KP may have a limited effect at height restoration in many patients (22). Alternatively, this limited clinical result could be due to indiscriminate patient selection. Patients in Lieberman et al’s series, where the average symptom duration was 5.9 months, were treated relatively late after fracture and many of these patients could have experienced partial fracture healing before KP. Although these reports are anecdotal, it does seem that vertebral compression fractures that are treated closer to their date of incidence tend to experience more height restoration (22). Whereas the average height restoration in a clinical setting ranges from 2.5 to 3.5 mm (33), no clinical trials are available that help us select those patients who will predictably get maximum height restoration by using KP. Pain relief seems less sensitive to “time since fracture.” Pain relief in Lieberman et al’s series was not adversely affected by treatment delay or the amount of height restoration achieved and was similar to that seen with PV (22).
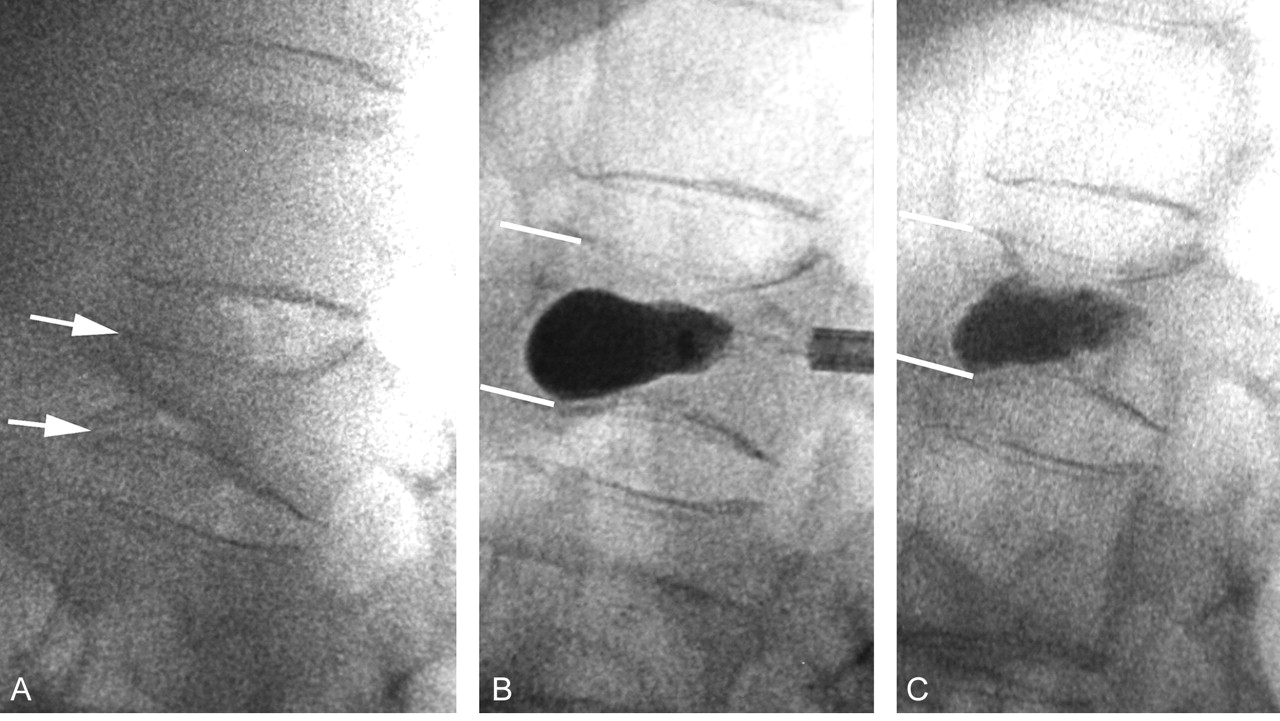
A, Compression fracture with anterior cleft before KP. Endplates are marked (arrows). The height is estimated at 50% of the height of the adjacent level above.
B, Fluoroscopic image showing balloon inflation during KP.
C, After cement injection, the height gain is approximately 4 mm, or 25% of a vertebral height (when compared with the adjacent level above). There was essentially no kyphosis to start with, and this vertebrae had a cleft originally and therefore would be expected to be a good candidate for height restoration.
Vertebral height restoration reported in some KP studies has been linked to correction of associated kyphotic deformity of the spine (23, 34). Theodorou et al reported an average kyphosis correction of 62.4% ± 16.7% (23); however, patients who are pain free following PV or KP usually experience less muscle spasm and tend to stand straighter with the elimination of spine pain. Mathis demonstrated this effect in a PV case with 50% kyphosis reduction after PV alone (39) (Fig 4). Teng et al reported kyphosis improvement following PV in 45 of 53 patients, with 49% having a kyphotic angle reduction of 5° or more (41). Studies on the secondary benefits of kyphosis correction, such as improved pulmonary function, are not yet available. Obviously, this is another place where the corrections of both PV and KP need to be compared with control to determine the relative difference between the therapies.

A, Radiograph of a compression fracture and 18° of kyphosis.
B, Following PV, there is modest height gain, estimated at 3–4 mm, and a reduction in kyphosis to 9°. (From JM Mathis. Percutaneous vertebroplasty. AJNR Am J Neuroradiol 2003; 24:1697–1706; by permission.)
What has often been neglected in the controversy regarding height restoration with KP is that PV can, in selected patients, also restore vertebral body height (Fig 4). Hiwatashi et al have shown that vertebral body height can be augmented by an average of 2.2 mm with PV simply by hyperextending the affected spinal segment (35). Similarly, McKiernan et al demonstrated dynamic fracture mobility in 35% of 65 vertebral compression fractures that they treated. Using PV alone, they reported that the “average anterior vertebral height increased 106% compared with initial fracture height (absolute increase, 8.41 ± 0.4 mm)” in patients with these mobile fractures. Their kyphotic angle reduction was 40% (40). If some height restoration can be expected from PV alone, the meager height recovery found in a series like that of Lieberman et al may be partially measuring the effect due to prone positioning rather than just that due to the balloon inflation.
Authors’ Opinions
Without doubt, additional trials are needed to establish conclusively the effectiveness of both PV and KP compared with conservative medical therapy and each other. Attempts to perform these types of studies have been stymied by poor patient enrollment in the control arm of each trial. This occurs because of the positive public awareness about these augmentation techniques and the dramatic benefit that previously treated patients have experienced. Few patients are willing to accept the chance of undergoing a sham procedure when the available treatments seem reliably safe and effective. A randomized comparison of PV and KP would also help establish patient selection criteria and individual procedure advantages allowing physicians to better utilize these procedures to the patients’ benefit. Until these data are available, we will likely continue to hear considerable jargon and relentless marketing claims about the relative safety and therapeutic advantages of each procedure.
We believe that both procedures relieve pain and can be performed with acceptable complication rates by prudent, well-trained physicians. We do note the large differential in cost of the procedures. If KP is going to be worthwhile, it should reliably produce significantly more height restoration than does PV. In our practices, we believe we employ KP differently but agree to its use when height restoration (beyond that usually achieved by PV) is feasible and would be beneficial. Our implementation of KP is driven by the “time since fracture” and is markedly different within our own ranks. One extreme requires fractures of 3 weeks or less (J.M.M.), while another tack includes fractures of less than 3 months (O.O.). Even with these guidelines, we are unable to assure large height restoration in all patients.
At present, we recommend that both procedures be available in the treatment armamentarium of all operators, thus allowing the physician, not the marketplace, to determine patient selection criteria. All vertebral compression fractures are not the same, and certain fracture subtypes may be more amenable to one or the other procedure. Regardless of which procedure is chosen, safety depends upon operator experience, excellent imaging equipment, and adequate cement opacification. Complications that have occurred with either procedure most often have been a result of poor operator judgment and experience or inadequate anatomic and cement visualization. Time and accumulated data will tell whether the promise of reliable height restoration with KP is realistic. Until then, careful use of either procedure should successfully relieve the pain associated with vertebral compression injury.
References
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Racial and Health Insurance Disparities of Inpatient Spine Augmentation for Osteoporotic Vertebral Fractures from 2005 to 2010
- Post-Vertebral Augmentation Back Pain: Evaluation and Management
- Trends of Inpatient Spine Augmentation: 2001-2008
- Comparative Hospital Economics and Patient Presentation: Vertebroplasty and Kyphoplasty for the Treatment of Vertebral Compression Fracture
- Role of cementoplasty in the management of compression vertebral body fractures
- Interventional Therapies for Cancer Pain Management: Important Adjuvants to Systemic Analgesics
- Unsuspected Lymphoma Diagnosed with Use of Biopsy During Kyphoplasty
- Clnical Study of the Treatment of Patients with a Metastatic Spinal Tumor by Percutaneous Vertebroplasty under the Guidance of DSA